163
Granuloma annulare

Over time, the papules and patches of granuloma may coalesce in to large confluent areas.

The ankle is a common site for granuloma annulare, as are the dorsal hands and fingers. Although rare, granuloma annulare can be generalized.
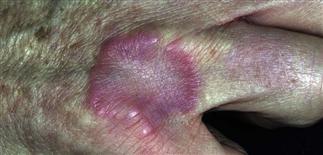
Granuloma annulare lesions are pink to flesh-colored annular patches or plaques, with an elevated border and central clearing. It is often misdiagnosed as ringworm.

Solitary red to pink arcuate plaque on the dorsal hand knuckles with raised border, no scale and central clearing, characteristic of granuloma annulare.
DESCRIPTION
A slowly progressive, self-limited, granulomatous-like dermal skin disease. Characterized by round or annular plaques that may initially resemble tinea and spontaneously disappear over time. There is both a localized and more rare, generalized form.
HISTORY
• About 70% of patients with granuloma annulare are younger than 30 years, and 40% are younger than 15 years. • Duration is highly variable. • The conditions in half of patients resolves within 2 years, but 40% experience recurrence at the same site. • Lesions tend to be asymptomatic. Patients become more concerned when multiple lesions in multiple areas develop and expand.
PHYSICAL FINDINGS
• The disease begins with an asymptomatic, flesh-colored papule that undergoes central involution. Small, firm, flesh-colored or violaceous papules then develop in a ring-like fashion. • Over months, a ring of papules coalesce into a concentric annular plaque that slowly increases in diameter up to 5 cm. • The localized form, most common in young women, is most frequently found on the lateral or dorsal surfaces of the hands and feet. Individual lesions may persist for many years then vanish, only to appear later in life at the same or different locations. • Disseminated or generalized granuloma annulare occurs in adults and appears with numerous flesh-colored or violaceous papules, some of which form annular rings. The papules may be accentuated in sun-exposed areas. The course is variable but may persist for many years. • Granuloma annulare is most often confused with tinea. • Granuloma annulare is rarely associated with diabetes mellitus.
TREATMENT
• Localized lesions are asymptomatic and are usually left untreated. • Superpotent topical steroids used daily in 2- to 3-week intervals are sometimes effective. Lower-potency topical steroids can be occluded for shorter periods of time. • Intralesional triamcinolone acetonide can be injected only into the elevated border. This is predictably effective and induces long periods of remission. • Disseminated or generalized granuloma annulare has been reported to occasionally respond to dapsone, isotretinoin, etretinate, hydroxychloroquine, and niacinamide.






