Glucose metabolism and diabetes mellitus
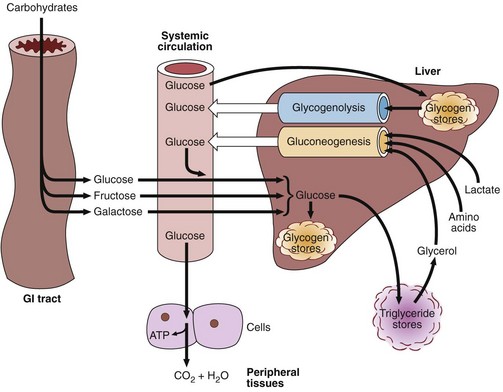
Dietary carbohydrate is digested in the gastrointestinal tract to simple monosaccharides, which are then absorbed. Starch provides glucose directly, while fructose (from dietary sucrose) and galactose (from dietary lactose) are absorbed and also converted into glucose in the liver. Glucose is the common carbohydrate currency of the body. Figure 31.1 shows the different metabolic processes that affect the blood glucose concentration. This level is, as always, the result of a balance between input and output, synthesis and catabolism.
Insulin
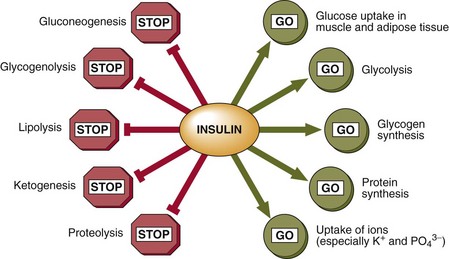
Insulin signals the fed state. It switches on pathways and processes involved in the cellular uptake and storage of metabolic fuels, and switches off pathways involved in fuel breakdown (Fig 31.2). It should be noted that glucose cannot enter the cells of most body tissues in the absence of insulin.
Diabetes mellitus
Primary diabetes mellitus is generally subclassified into Type 1 or Type 2. These clinical entities differ in epidemiology, clinical features and pathophysiology. The contrasting features of Types 1 and 2 diabetes mellitus are shown in Table 31.1.
Table 31.1
Type 1 versus Type 2 diabetes mellitus
| Main features | Type 1 | Type 2 |
| Epidemiology | ||
| Frequency in northern Europe | 0.02–0.4% | 1–3% |
| Predominance | N. European | Worldwide |
| Caucasians | Lowest in rural areas of developing countries | |
| Clinical characteristics | ||
| Age | <30 years | >40 years |
| Weight | Low/normal | Increased |
| Onset | Rapid | Slow |
| Ketosis | Common | Under stress |
| Endogenous insulin | Low/absent | Present but insufficient |
| HLA associations | Yes | No |
| Islet cell antibodies | Yes | No |
| Pathophysiology | ||
| Aetiology | Autoimmune destruction of pancreatic islet cells | Impaired insulin secretion and insulin resistance |
| Genetic associations | Polygenic | Strong |
| Environmental factors | Viruses and toxins implicated | Obesity, physical inactivity |
Late complications of diabetes mellitus
 Microangiopathy is characterized by abnormalities in the walls of small blood vessels, the most prominent feature of which is thickening of the basement membrane. It is associated with poor glycaemic control.
Microangiopathy is characterized by abnormalities in the walls of small blood vessels, the most prominent feature of which is thickening of the basement membrane. It is associated with poor glycaemic control.
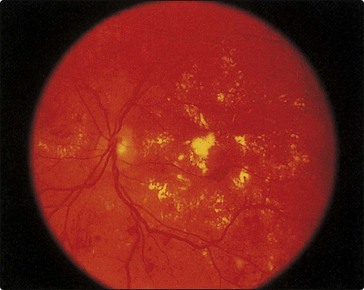
 Retinopathy may lead to blindness because of vitreous haemorrhage from proliferating retinal vessels, and maculopathy as a result of exudates from vessels or oedema affecting the macula (Fig 31.3).
Retinopathy may lead to blindness because of vitreous haemorrhage from proliferating retinal vessels, and maculopathy as a result of exudates from vessels or oedema affecting the macula (Fig 31.3).



 Clinical note
Clinical noteGlucose metabolism and diabetes mellitus
 Glucose is the carbohydrate currency of the body, all other carbohydrates being converted to glucose after digestion and absorption.
Glucose is the carbohydrate currency of the body, all other carbohydrates being converted to glucose after digestion and absorption.
 Insulin controls blood glucose by promoting the storage of metabolic fuels.
Insulin controls blood glucose by promoting the storage of metabolic fuels.

 Type 1 diabetes mellitus is caused by a complete lack of insulin and is most common in the young.
Type 1 diabetes mellitus is caused by a complete lack of insulin and is most common in the young.
 Type 2 diabetes mellitus accounts for 85% of all diabetics and can occur at any age.
Type 2 diabetes mellitus accounts for 85% of all diabetics and can occur at any age.
 Late complications of diabetes mellitus are a result of micro- and macroangiopathies.
Late complications of diabetes mellitus are a result of micro- and macroangiopathies.
