CHAPTER 10 Glenoid Exposure
Whenever we question surgeons who routinely perform hemiarthroplasty instead of total shoulder arthroplasty for conditions such as primary osteoarthritis about why they chose not to resurface the glenoid, by far the most common response is that they encounter problems with glenoid exposure. When questioned further, it is evident that most of these surgeons simply lack the information necessary to correctly and reliably provide visualization of the osseous glenoid. Glenoid exposure can be simplified by following a sequence of surgical steps. This chapter outlines our systematic technique of capsular release that provides sufficient visualization for glenoid resurfacing.
TECHNIQUE FOR GLENOID EXPOSURE
Anterior Release
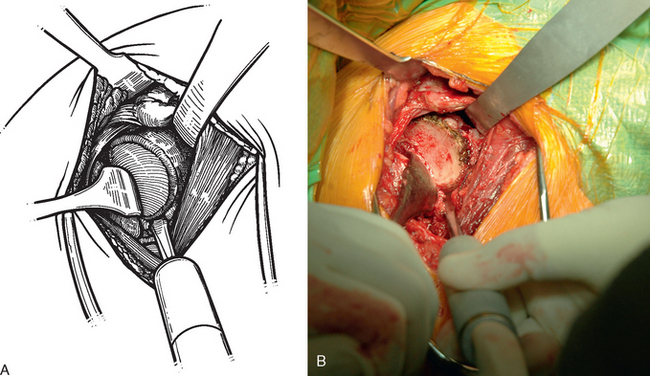
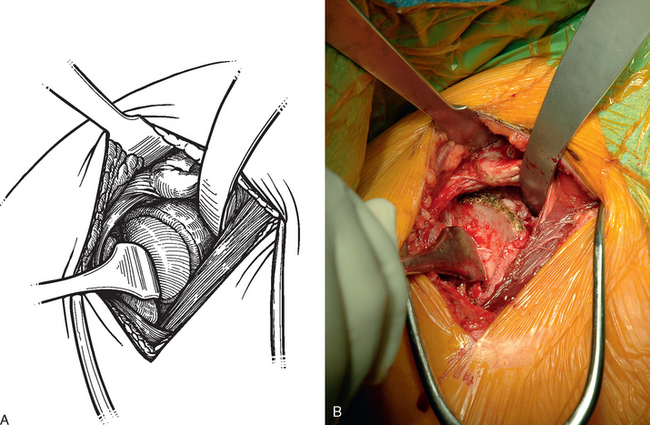
After the subscapularis is retracted medially with a sponge and small glenoid rim retractor, attention is turned to glenoid exposure. A needle tip electrocautery is used to excise any remaining labrum beginning at the base of the coracoid process and extending inferiorly to the 5 o’clock position in a right shoulder (7 o’clock in a left shoulder). This allows identification of the osseous anterior margin of the glenoid (Fig. 10-1).
Inferior Release
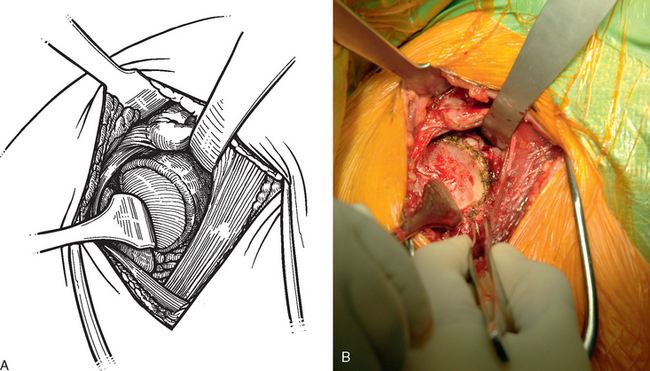
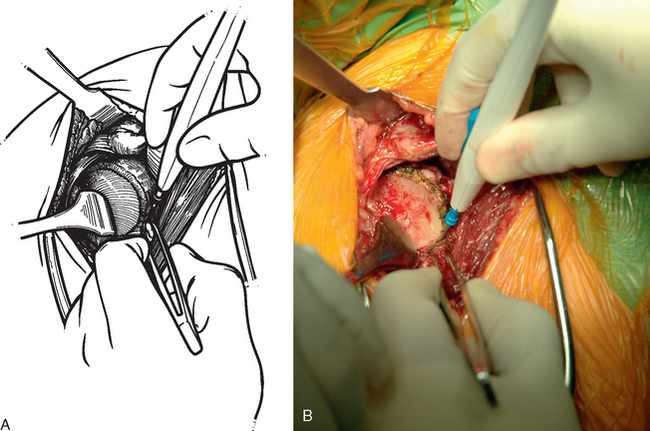
In nearly all cases, implantation of a glenoid component requires release of the inferior capsule to obtain adequate exposure. The tip of the electrocautery is used to release the inferior capsule directly off the rim of the glenoid bone (Fig. 10-2). To avoid damaging the axillary nerve, the tip of the electrocautery must be kept in contact with glenoid bone. This release is extended sufficiently medially toward the axillary border of the scapula to completely transect the capsule and expose the muscular fibers of the triceps inserting on the inferior osseous glenoid. Visualization of the muscular fibers of the triceps or the axillary border of the scapula indicates that dissection of the capsule is sufficient.
Posterior Release
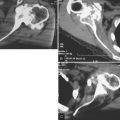
The amount of posterior subluxation present on preoperative secondary imaging studies (computed to-mography, magnetic resonance imaging) determines the posterior extent of release. In shoulders without posterior subluxation, the release continues posteriorly to the 8 o’clock position for right shoulders (4 o’clock position for left shoulders). In shoulders that have preexisting posterior subluxation, either with or without posterior glenoid erosion, the release continues initially to only the 6 o’clock position. These patients often have a distended posterior capsule, so to avoid further compromising these posterior structures, no more release is performed than is absolutely necessary. If release to only the 6 o’clock position proves inadequate later during glenoid reaming, the release can be extended at that time. A Cobb elevator can be used to check the release for completeness (Fig. 10-3). Figure 10-4 shows the completed release.