[level-membership-for-opthalmology-category]6.1
Glaucoma
Clinical Features:
The hallmark of glaucomatous optic neuropathy is a progressive loss of RNFL tissue eventually culminating in visual field loss, with associated changes in the ONH (Fig. 6.1.1). This may be associated with elevated intraocular pressure. The RNFL loss can be noted qualitatively on careful clinical examination, and is best appreciated with red-free illumination of the fundus. Slit-lamp biomicroscopy with a handheld lens is the best method of optic disc examination, since it provides good stereopsis and magnification. Optic disc stereo photographs are complementary and may identify findings missed on slit-lamp examination. Progressive changes in the ONH follow the RNFL loss, including focal or diffuse loss of neuroretinal rim tissue and enlargement of the cup.
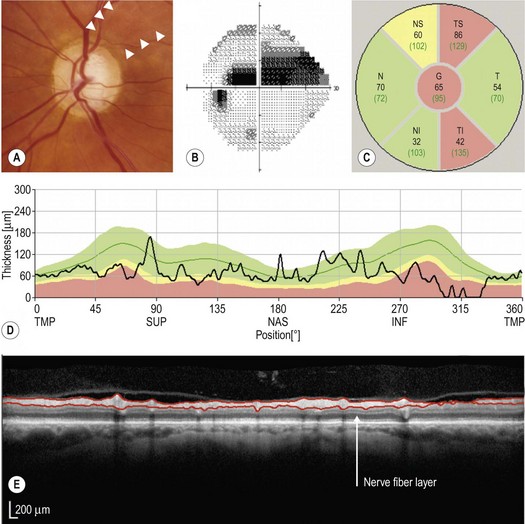
Figure 6.1.1 Composite figure showing (A) the left optic disc photograph, (B) the visual field, (C) the six sectors OCT map, (D) the TSINT map, and (E) the OCT scan with the RNFL automated segmentation of a patient with moderate glaucoma (visual field mean deviation −6.4 dB). The optic disc (A) shows an inferotemporal focal absence of neuroretinal rim tissue (notch) and superotemporal focal thinning of the neuroretinal rim tissue (notching) with the corresponding RNFL defect (between arrowheads). The visual field (B) shows a defect in the superior hemifield threatening fixation. The OCT (C, D and E) shows markedly RNFL thinning of the superotemporal and inferotemporal sectors with ‘outside normal limits’ classification for both and ‘borderline’ classification in the superonasal sector. The OCT scan shows pronounced RNFL thinning in the inferotemporal sector, noticed in the segmented RNFL (arrow in E). (Courtesy of Dr Marcelo Nicolela, Dalhousie University.)
OCT Features:
The key anatomical features assessed on the ONH scan are:
Most commercially available OCT machines have software permitting comparison of change over time.
Ancillary Testing:
Visual field testing estimates the functional damage in glaucomatous eyes. However, it has been shown that up to 50% of the RNFL may be lost prior to any change in the visual field. Moreover, visual field testing is dependent on patient cooperation and often exhibits large variation between visits. Detection of visual field changes often requires several repetitions of the test, which may delay the diagnosis (Fig. 6.1.1B).
[/level-membership-for-opthalmology-category][not-level-membership-for-opthalmology-category]6.1
Glaucoma
Clinical Features:
The hallmark of glaucomatous optic neuropathy is a progressive loss of RNFL tissue eventually culminating in visual field loss, with associated changes in the ONH (Fig. 6.1.1
[/not-level-membership-for-opthalmology-category]
