CHAPTER 14 Geriatrics
I. Definitions
A. Geriatrics is the branch of medicine concerned with the health care of the elderly. It aims to promote health and to prevent and treat disease and disabilities in older adults.
B. A geriatrician is a medical doctor who is specially trained to prevent and manage the unique and, oftentimes, multiple health concerns of older adults. Geriatricians are able to treat older patients, manage multiple disease symptoms, and develop care plans that address the special health care needs of older adults.
II. Conditions Commonly Seen in Geriatric Patients
A. Parkinson disease
1. Pathophysiology and epidemiology
a. Progressive, neurologic disorder due to degeneration of presynaptic dopaminergic neurons in the substantia nigra equals the loss of postsynaptic dopamine activity in the striatum (dopamine involved in inhibition of cholinergic and glutamatergic loops and increased activity in these systems)
b. Mean age of diagnosis: 55–60 years; incidence approximately 20/100,000; mortality not greatly increased
c. Etiology of idiopathic Parkinson disease unknown: possibly a combination of genetic predisposition and environmental factors. Hereditary accounts for less than 2% of all diagnosed cases. Oxidative stress and free radical damage may contribute to neuronal degeneration.
d. Drug-induced: Caused by antidopaminergic agents (metoclopramide, prochlorperazine, neuroleptics, reserpine, methyldopa, etc.); rarely amiodarone, selective serotonin reuptake inhibitors (SSRIs), valproic acid, diltiazem, verapamil
2. Signs and symptoms (Figure 14-1)
b. Minor: difficulty with fine coordinated movements; postural disturbance (later in disease state); flattened facial expression (masked facies); voice may become hypophonic, monotonal; shuffling gait; micrographia; drooling, difficulty swallowing liquids; pain in affected limb; depression or dementia; constipation; orthostatic hypotension; urinary frequency; sweating; dermatitis; sexual dysfunction
3. Treatment
a. The goal is to improve motor symptoms (tremor, bradykinesia, rigidity), inhibit cholinergic action, ease dopaminergic action
b. Guidelines differ regarding initial therapy: dopamine first line versus last. Treatment should not be initiated in most patients until motor symptoms significantly impair quality of life (QOL) and/or daily function.
c. All treatments are patient specific: doses must be tailored and changed according to patient’s disease state, progression, and side effects.
5. Medications
a. Levodopa/carbodopa (Sinemet, Sinemet CR)
1) Mechanism of action: Levodopa is a dopamine precursor that can cross the blood-brain barrier and replace dopamine in the brain (metabolized by dopa-decarboxylase to dopamine). Carbidopa inhibits peripheral dopa-decarboxylase and allows more dopamine to enter brain, which allows lower levodopa dose, more-rapid dosage titration, and reduced peripheral side effects (nausea/vomiting, arrhythmias, orthostatic hypotension).
2) Usual dose: minimum 75–100 mg/day carbidopa required. Initial dose is one carbidopa 25 mg/levodopa 100 mg tablet PO three times per day. Levodopa absorption is impaired by high-protein meals.
3) Side effects (levodopa): nausea/vomiting, insomnia or sedation, confusion, hallucinations, dyskinesias, muscle cramping (dystonias), wearing off phenomenon (end-of-dose failure), hypersexuality
4) Levodopa/carbidopa (Sinemet): Approximately 5 years after initiation, many patients experience motor complications (wearing off phenomenon, dyskinesia). Recent guidelines recommend initiating a dopamine agonist early in therapy, which delays need for levodopa and complications of therapy. As disease progresses, dopamine will be needed.
b. Amantadine (Symmetrel): mildly effective against tremor and rigidity
1) Mechanism of action: unclear, may be an NMDA (N-methyl d-aspartate) antagonist; blocks uptake and enhances the release of dopamine
c. Selegiline (Eldepryl): mild to moderate symptom relief as monotherapy in early disease; also used for adjunctive therapy late in disease to prevent wearing-off phenomenon. Some studies show increased morbidity when used with levodopa. Multiple other studies do not show increased morbidity; however, may want to avoid if patients have history of dementia, frequent falls, or postural hypotension
1) Mechanism of action: selective, irreversible MAO-B inhibitor. Selectivity is lost if the dose is >20 mg/day; metabolized to amphetamine/methamphetamine
2) Side effects: insomnia, sedation, confusion, agitation, hallucinations, vivid dreams; may enhance levodopa-induced dyskinesias
d. Dopamine receptor agonists: bromocriptine (Parlodel), pergolide (Permax), pramipexole (Mirapex), ropinirole (Requip)
1) Dopamine agonists may be used as monotherapy early in the disease; adjunctive therapy in late disease to manage motor complications
2) Usual dose: start doses low and titrate slowly. It may take months to achieve therapeutic dosage; taper up and taper down. Reduce the dose in patients with renal disease.
a) Bromocriptine: 1.25 mg PO twice daily, increasing the total daily dose by 2.5 mg every 14–28 days until the desired therapeutic response occurs
e. Cateochol-O-methyltransferase (COMT) inhibitors: tolcapone (Tasmar), entacapone (Comtan)
3) COMT inhibitors work with levodopa and prolong its action. Because they affect levodopa metabolism, they are only effective in patients receiving levodopa therapy.
4) Entacapone is a reversible peripheral COMT inhibitor. It is the preferred COMT inhibitor because it does not require liver function test (LFT) monitoring. Tolcapone is a peripheral and central COMT inhibitor. It achieves greater COMT inhibition than entacapone. However, its use is restricted due to occurrence of fatal hepatotoxicity; discontinue tolcapone use after 3 weeks if patient fails to show expected benefit from the drug. Patients must give consent, and LFTs should be performed every 2 weeks for the first 12 months, then every 4 weeks for the next 6 months, and then every 8 weeks for the duration of therapy.
5) Usual dose
6) Side effects: exacerbation of levodopa side effects, such as nausea, urine discoloration (dark yellow to orange-brown), diarrhea (after several weeks). Be alert to signs of liver problems, such as worsening abdominal pain, yellowing of the skin or whites of the eyes (especially with tolcapone). Retroperitoneal fibrosis and other lung problems are rare.
d. Drug side effects
1) Nausea/vomiting: Patients should take levodopa and dopamine agonists with nonprotein snack. If antiemetics are needed, do not use dopamine receptor blockers (see section on drug-induced Parkinson disease).
B. Alzheimer disease and dementia
1. Pathophysiology/epidemiology
a. Genetic factors: known to play a role in some cases of Alzheimer disease (AD). Some families with a history of early-onset AD have a mutation on the amyloid beta precursor protein (APP) gene. Another gene, the apolipoprotein (Apo) E gene, also has been implicated in the disease. Apo E is a protein found with beta amyloid (a protein found in the brains of patients with AD) in neuritic (inflamed nerve) plaques. Together, these genetic mutations account for less than 10% of all patients with AD.
b. Plaques and tangles: The causes of AD are poorly understood, but its effect on brain tissue has been demonstrated clearly. AD damages and kills brain cells. Neurons generate electrical and chemical signals that are relayed from neuron to neuron to help an individual think, remember, and feel (physically and emotionally). Brain chemicals called neurotransmitters help these signals flow seamlessly between neurons. Initially in people with AD, neurons in certain locations of the brain begin to die. When they die, lower levels of neurotransmitters are produced, creating signaling problems in the brain. One neurotransmitter, acetylcholine, has been found to be deficient in the brains of those with AD. Medication treatment is based around increasing the amount of acetylcholine in the brain.
1) Plaques and tangles in brain tissue are considered hallmarks of AD. Plaques are made up of beta-amyloid, a normally harmless protein. Although the ultimate cause of neuron death in AD is not known, mounting evidence suggests that a form of beta-amyloid protein may be the cause. The plaque is responsible for memory deterioration in individuals with AD.
c. Inflammation: Researchers have observed inflammation in the brains of some people with AD. As beta-amyloid plaques develop in the spaces between neurons, immune cells are getting rid of dead cells and other waste products in the brain. Although research has found that the inflammation occurs before plaques have fully formed, it is not known how this development relates to the disease process. There is also debate about whether inflammation has a damaging effect on neurons or whether it is beneficial in clearing away plaques.
d. Age is the most important risk factor for AD. The number of people with the disease doubles every 5 years beyond age 65 years.
e. It is estimated that about five million Americans have AD, and about 360,000 people are newly diagnosed every year. AD affects about 10% of people ages 65 years and older, and the number doubles roughly every 10 years after age 65 years. Half of the population ages 85 years and older may have AD.
f. Signs and symptoms
1) Mild symptoms: mental deterioration, such as memory impairment and confusion, difficulty learning and remembering new information, difficulty with daily tasks, and depression (sadness, decreased interest in usual activities, loss of energy)
2) Moderate symptoms: forgetting old facts, continually repeating stories, and/or asking the same questions over and over, deficiencies in intellect and reasoning, a lack of concern for appearance, hygiene, and sleep
g. Medications
1) Cholinesterase inhibitors: donepezil (Aricept), rivastigmine (Exelon), galantamine (Razadyne), and tacrine (Cognex)
a) Mechanism of action: inhibits the degradation of acetylcholine by inhibiting the enzyme acetylcholinesterase
b) Usual doses
(1) Donepezil (Aricept): initial 5 mg/day at bedtime; may increase to 10 mg/day at bedtime after 4–6 weeks
c) Side effects: gastrointestinal effects (diarrhea, nausea, vomiting, anorexia) are most common and may require dose reductions for some agents (e.g., galantamine). Increased salivation, increased respiratory secretions, bradycardia, headache, fatigue, and vertigo are other side effects. Hepatotoxicity has been attributed to the use of tacrine and has limited the drug’s clinical use.
2) Memantine (Namenda)
a) Mechanism of action: NMDA antagonist, blocks glutamate activity and prevents excessive influx of calcium and, thereby, neuronal death
4) Adjunct therapies
a) Depression that occurs during the early stages is commonly treated with antidepressant medications, such as selective serotonin reuptake inhibitors (SSRI) including fluoxetine (Prozac) and sertraline (Zoloft), and the tricyclic antidepressants (TCA), including amitriptyline (Elavil). Side effects include drowsiness, fatigue, and sedation. TCA may increase mental confusion.
b) Agitation may be treated with an antipsychotic medication, such as haloperidol (Haldol), risperidone (Risperdal), olanzapine (Zyprexa), and quetiapine (Seroquel). NOTE: Antipsychotics are not FDA approved to treat behavioral symptoms of AD and may increase the risk for death in elderly patients with dementia. Side effects include sedation, confusion, and tardive dyskinesia (an irreversible movement disorder characterized by lip smacking, facial grimacing, and unsteady walking).
C. Glaucoma
1. Pathophysiology and epidemiology
a. Glaucoma is the name given to a group of conditions caused by increased intraocular (inside the eye) pressure (IOP), resulting either from a malformation or malfunction of the eye’s drainage system. Left untreated, an elevated IOP may cause irreversible damage to the optic nerve and retinal fibers, resulting in a progressive, permanent loss of vision. However, early detection and treatment can slow or even halt the progression of the disease.
b. It is estimated that more than three million Americans have glaucoma but only half of those know they have it. Most individuals with glaucoma are not aware of problems with their vision. This is because the central vision (for reading and recognizing people) is only affected when glaucoma has advanced to a late stage. Even when central vision is still good, glaucoma may affect the vision needed for driving and other daily functions, including seeing stair steps or reading.
c. Approximately 120,000 are blind from glaucoma, accounting for 9%–12% of all cases of blindness in the United States. About 2% of the population 40–50 years old and 8% older than 70 years of age have elevated IOP.
2. Most common forms of glaucoma
a. Open-angle glaucoma (chronic): Open angle (also called chronic open angle or primary open angle) is the most common type of glaucoma and usually causes no symptoms at first. Even though the anterior structures of the eye appear normal, aqueous fluid builds within the anterior chamber, causing the IOP to become elevated. Left untreated, this may result in permanent damage of the optic nerve and retina.
b. Angle-closure glaucoma (acute): Acute angle closure glaucoma, or closed-angle glaucoma, occurs because of an abnormality of the trabecular mesh work and the canal of Schlemm in the eye that keeps aqueous humor fluid from draining. In most of these cases, the space between the iris and cornea is narrower than normal, putting pressure on the canal of Schlemm and leaving a smaller channel for the aqueous humor to drain. If the flow of aqueous becomes completely blocked, the IOP rises sharply, causing a sudden angle closure attack. Only about 10% of the population with glaucoma has acute angle closure glaucoma.
c. Secondary glaucoma: Secondary glaucoma can develop as complications of other medical conditions, such as inflammation, trauma, previous surgery, diabetes, or a tumor. These types of glaucoma are sometimes associated with eye surgery or advanced cataracts, eye injuries, certain eye tumors, uveitis (eye inflammation), and certain medications (including topical steroid creams, cocaine, chlorpromazine or Thorazine, and phenelzine or Nardil).
5. Medications
a. Prostaglandin analogs
2) Adverse effects: may change the pigment of the iris (may be permanent); may change direction of eyelashes (may be permanent) and increase growth of eyelashes
c. Beta blockers (nonselective)
2) Caution: Beta blockers are absorbed systemically and should be used cautiously in patients with heart, lung, or endocrine disorders. The use of lacrimal occlusion technique upon administration reduces potential for systemic absorption of the eye drops.
d. Beta blockers (beta-1 selective)
D. Osteoporosis
1. Pathophysiology and epidemiology
a. Osteoporosis is more common in older individuals and non-Hispanic white women, but it can occur at any age, in men as well as in women, and in all ethnic groups.
b. In the United States, about eight million women and two million men have osteoporosis. Those older than 50 years are at greatest risk of developing osteoporosis and suffering related fractures. In this age group, one in two women and one in six men will have an osteoporosis-related fracture at some point in their lives.
2. Signs and symptoms
a. In the early stages of bone loss, there usually is no pain or symptoms. After bones have been weakened by osteoporosis, signs and symptoms may include back pain, which can be severe with a fractured or collapsed vertebra; loss of height over time, with an accompanying stooped posture; and fracture of the vertebrae, wrists, hips, or other bones.
3. Treatment
a. Nutrition and lifestyle
1) Dietary factors: calcium intake of 1200 mg daily is recommended for adults older than 50 years. Adequate vitamin D intake is also important for calcium absorption and to maintain muscle strength; adults older than 60 years of age should take 600–800 IU per day. Milk and milk products are calcium-dense foods providing about 300 mg of calcium per serving. These foods also contain other nutrients important to bone health such as vitamin D (if fortified), phosphorus, and magnesium.
2) Weight-bearing exercises: Weight-bearing aerobic activities, involving the bones supporting body weight, have a positive effect in maintaining and increasing bone mass and preventing osteoporosis. These activities include weight-lifting, jogging, hiking, stair-climbing, step aerobics, dancing, racquet sports, and other activities that require muscles to work against gravity.
b. Medications
1. Bisphosphonates
b) Dose: Alendronate (Fosamax) or risedronate (Actonel) can be taken daily or are available in a once-weekly dosage form; ibandronate (Boniva) can be taken once a month. An IV form of ibandronate is infused every 3 months. Another IV bisphosphonate is zoledronic acid (Reclast); it is infused once yearly.
c) Side effects: nausea, abdominal pain, and the risk of an inflamed esophagus or esophageal ulcers, especially if the individual has had acid reflux or ulcers in the past. Osteonecrosis of the jaw is a rare but serious side effect.
1) A baseline and pre-dose determination of serum creatinine is necessary in individuals receiving IV bisphosphonates to determine kidney function.
2) When taking an oral bisphosphonate, proper administration is necessary to reduce the risk of esophageal side effects. Proper directions include: On the day of dosing, take dose first thing in the morning. Do not eat or drink anything before taking medicine. Swallow with a full glass (6 to 8 fluid ounces) of plain water only. Do not chew or crush. After taking, do not eat breakfast, drink, or take any other medicines or vitamins for at least 30 minutes. Stand or sit up for at least 30 minutes after taking; do not lie down.
2. Calcitonin salmon (Miacalcin):
a) A naturally occurring hormone produced by the thyroid gland that can be given as an injection or is more commonly used in ambulatory settings as a nasal spray.
E. Benign prostatic hyperplasia (BPH)
1. Pathophysiology/epidemiology
a. Benign prostatic hyperplasia (BPH) is a normal, gradual enlargement of the prostate caused by hormonal fluctuations, such as decreases in testosterone and increases in dihydrotestosterone (DHT) and estrogen in prostate tissue. BPH usually begins in middle age. BPH does not lead to cancer. BPH does not generally cause pain, but there is often a general discomfort (a feeling of pressure) in the groin area.
b. As the prostate enlarges, it presses against the urethra and interferes with urination. At the same time, the bladder wall becomes thicker and irritated and begins to contract, even when it contains small amounts of urine, which causes more frequent urination. Additionally, as the bladder weakens, it may not empty completely, leaving some urine. Blocking or narrowing of the urethra by the prostate and partial emptying of the bladder cause many of the problems associated with BPH.
c. BPH affects about half of men older than 60 years, and 80% of men aged 80 years or older; it is considered to be a condition related to aging. Almost every man older than 45 years experiences some prostate enlargement, but symptoms are rarely felt before the age of 60 years. BPH affects all men differently and therefore treatment varies.
4. Treatment
a. Treatment options for BPH include lifestyle changes, “watchful waiting,” drug therapy, nonsurgical procedures, and major surgery. The goals of treatment are to improve urinary flow and decrease the symptoms an individual may be experiencing. Treatment should also delay or prevent the progression of BPH.
5. Medications
a. 5-Alpha reductase inhibitors: dutasteride (Avodart), finasteride (Proscar)
b. Alpha-1 blockers: alfuzosin (UroXatral), doxazosin (Cardura), tamsulosin (Flomax), terazosin (Hytrin)
1) Mechanism of action: blocks adrenergic receptors on smooth muscle of the prostate and bladder neck to improve urine flow and to reduce bladder outlet obstruction
2) Usual dose
b) Doxazosin (Cardura): immediate release: 1 mg once daily in morning or evening may titrate to response; goal of 4–8 mg/day; maximum dose 8 mg/day. Extended release: 4 mg once daily with breakfast; titrate based on response and tolerability every 3–4 weeks to maximum recommended dose of 8 mg/day
4) Contraindication and interaction: concurrent use with phosphodiesterase-5 (PDE-5) inhibitors (commonly used for erectile dysfunction) including sildenafil (>25 mg), tadalafil, or vardenafil. Substrate of CYP 3A4, avoid St. John’s wort, strong inhibitors (ketoconazole, itraconazole, ritonavir); beta blockers may enhance the orthostatic effect of alpha-1 blockers
F. Erectile Dysfunction (ED)
1. Pathophysiology and epidemiology
a. Erectile dysfunction (ED), sometimes called impotence, is the repeated inability to obtain or retain an erection firm enough for sexual intercourse. Impotence may also be used to describe other problems that interfere with sexual intercourse and reproduction, such as lack of sexual desire and problems with ejaculation or orgasm.
b. Medications
1. Phosphodiesterase-5 (PDE-5) inhibitors: sildenafil (Viagra), tadalafil (Cialis), and vardenafil (Levitra): first-line medication
a) Mechanism of action: inhibition of PDE-5 by sildenafil causes increased levels of cyclic guanosine monophosphate (cGMP) in the corpus cavernosum, resulting in smooth muscle relaxation and inflow of blood to the corpus cavernosum
b) Usual dose
1) Sildenafil: usual dose 50 mg once daily 1 hour (range 30 minutes to 4 hours) before sexual activity; dosing range 25–100 mg once daily
2. Prostaglandin E1 analogs: alprostadil (Muse, Caverject, Edex)
a) Mechanism of action: causes vasodilation by means of direct effect on vascular and ductus arteriosus smooth muscle; relaxes trabecular smooth muscle by dilation of cavernosal arteries when injected along the penile shaft, allowing blood flow to and entrapment in the lacunar spaces of the penis
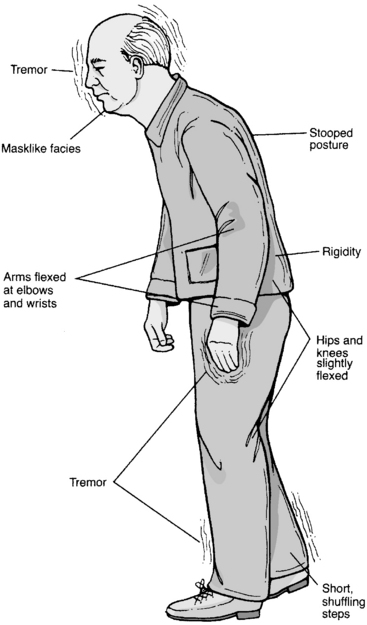
Figure 14-1 Signs and symptoms of Parkinson’s disease.
From Monahan FD, Drake T, Neighbors M: Nursing care of adults. Philadelphia, 1994, Saunders
PATIENT PROFILE
Allergies: No known drug allergies (NKDA)
History of iron-deficiency anemia, no longer treated
Frequent urinary tract infections (UTIs)
Laboratories at last medical appointment:
Liver function tests: within normal limits
CBC and differential: within normal limits
Urine: clear, no bacteria or protein
Alcohol use: None in recent years
Lodine XL 400 mg PO once daily
Hydrochlorothiazide 12.5 mg PO once daily
PATIENT PROFILE QUESTIONS


2. The physician would like to prescribe donepezil (Aricept) for this patient. Which of the following represents the correct starting dose?
3. Which of the following regarding donepezil are true?
I. Common side effects are cholinergic in nature and include nausea, diarrhea, GI disturbances, and dizziness.
4. After several months of treatment, SR is having difficulty swallowing her medications. The patient’s family would like her to remain on a cholinesterase inhibitor because they feel she has done well on the medications. However, they would like something that is not swallowed, if available. They are concerned about choking. Which medication comes in a nonoral dose form?
REVIEW QUESTIONS
(Answers and Rationales on page 361.)
2. Which of the following statements regarding Alzheimer disease is/are true?
7. Which of the following drugs improves symptoms of Parkinson disease by increasing levels of dopamine in the brain?
21. The most common community-acquired infection that results in hospitalization for the elderly patient is:
43. On ophthalmologic examination of an eye with glaucoma, which of the following findings is expected?
44. Which of the following is the appropriate dosage for immediate treatment of acute angle-closure glaucoma?