[level-membership-for-dermatology-category]
Genitourinary medicine
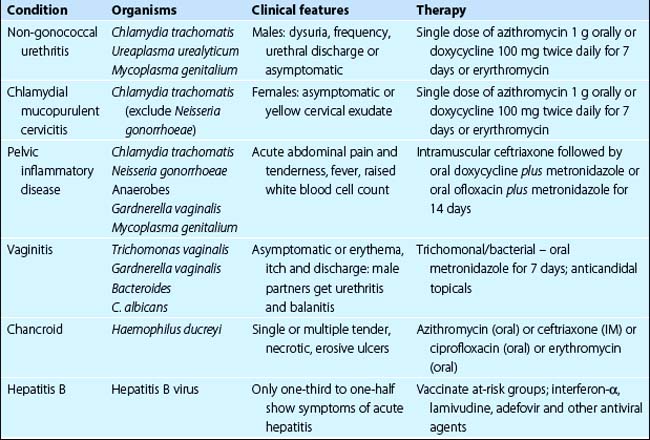
In the UK and Ireland, genitourinary medicine has traditionally been a separate specialty from dermatology, but the two are combined as ‘dermatovenereology’ in many countries. It has become increasingly important for those treating skin disease to know more about genitourinary disorders. Genitourinary diseases range as follows (see also Table 1): syphilis, gonorrhoea, human immunodeficiency virus (HIV) infection (p. 56), chlamydial infection, pelvic inflammatory disease, vaginitis, chancroid viral warts (p. 52), genital herpes simplex (p. 54), hepatitis B and hepatitis C, vulval/perianal dermatoses, penile/scrotal dermatoses.
Syphilis (lues)
Clinical presentation
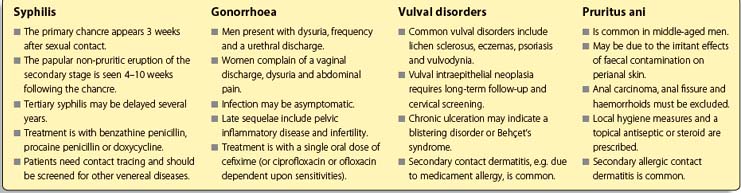
 Primary chancre. About 3 weeks after sexual contact, a primary chancre, a painless ulcerated button-like papule, develops at the site of inoculation. This is usually genital (Fig. 1), but oral and anal chancres are seen in men who have sex with men. Regional lymphadenopathy is common. Without treatment, the chancre clears spontaneously in 3–10 weeks. Serology is not positive until 4 weeks after infection, but spirochaetes can be isolated from the chancre.
Primary chancre. About 3 weeks after sexual contact, a primary chancre, a painless ulcerated button-like papule, develops at the site of inoculation. This is usually genital (Fig. 1), but oral and anal chancres are seen in men who have sex with men. Regional lymphadenopathy is common. Without treatment, the chancre clears spontaneously in 3–10 weeks. Serology is not positive until 4 weeks after infection, but spirochaetes can be isolated from the chancre.
 Secondary stage. This phase starts 4–10 weeks after the onset of the chancre. It is characterized by a non-itchy pink or copper-coloured papular eruption on the trunk, limbs, palms and soles (p. 42). Untreated, the eruption resolves in 1–3 months. Serology is positive.
Secondary stage. This phase starts 4–10 weeks after the onset of the chancre. It is characterized by a non-itchy pink or copper-coloured papular eruption on the trunk, limbs, palms and soles (p. 42). Untreated, the eruption resolves in 1–3 months. Serology is positive.
 Tertiary stage. About 30% of patients with untreated syphilis will develop late lesions, usually after a latent period of years. Painless nodules, sometimes with scaling, develop in annular or arcuate patterns on the face or back. Subcutaneous granulomatous gumma – usually on the face, neck or calf – ulcerate, scar and never heal completely (Fig. 2). Cardiovascular syphilis and neurosyphilis may coexist.
Tertiary stage. About 30% of patients with untreated syphilis will develop late lesions, usually after a latent period of years. Painless nodules, sometimes with scaling, develop in annular or arcuate patterns on the face or back. Subcutaneous granulomatous gumma – usually on the face, neck or calf – ulcerate, scar and never heal completely (Fig. 2). Cardiovascular syphilis and neurosyphilis may coexist.


Gonorrhoea
Clinical presentation
Gonococcaemia is rare but, when observed, results in fever, arthritis and pustules that are few in number and generally distributed on the hands, feet or near the large joints. This is a type of septic vasculitis which, like some other systemic infections (e.g. Neisseria meningitidis), may be purpuric.
Vulval disorders

 eczemas including allergic contact dermatitis (Fig. 3) and seborrhoeic dermatitis (p. 38)
eczemas including allergic contact dermatitis (Fig. 3) and seborrhoeic dermatitis (p. 38)



Herpes simplex (p. 54), viral warts (p. 52), candidiasis (p. 58), venereal infections (see above) and extramammary Paget’s disease (p. 88) also occur. Other specific disorders include the following:
 Vulval intraepithelial neoplasia (VIN): includes in situ squamous cell carcinoma and Bowenoid papulosis (Fig. 4). Cervical intraepithelial neoplasia can coexist and screening is required. Human papillomavirus infection may predispose to the precancerous change. There is a small risk of progression to invasive squamous cell carcinoma. Treatment is by cryosurgery or excision (for small areas), topical fluorouracil and laser therapy. Follow-up is needed.
Vulval intraepithelial neoplasia (VIN): includes in situ squamous cell carcinoma and Bowenoid papulosis (Fig. 4). Cervical intraepithelial neoplasia can coexist and screening is required. Human papillomavirus infection may predispose to the precancerous change. There is a small risk of progression to invasive squamous cell carcinoma. Treatment is by cryosurgery or excision (for small areas), topical fluorouracil and laser therapy. Follow-up is needed.

 Genital ulceration: may occur with pemphigoid or pemphigus (p. 78), or acutely with erythema multiforme. It is also seen with Behçet’s syndrome, a multisystem disorder in which recurrent oral aphthous ulceration and iridocyclitis also occur.
Genital ulceration: may occur with pemphigoid or pemphigus (p. 78), or acutely with erythema multiforme. It is also seen with Behçet’s syndrome, a multisystem disorder in which recurrent oral aphthous ulceration and iridocyclitis also occur.

Penile and scrotal eruptions
Balanitis (inflammation of the penile skin; Fig. 5) and scrotal eruptions can be caused by a similar list of conditions to those outlined above for vulval dermatoses. Specific disorders include:



Pruritus ani
The perianal skin is frequently involved in infective, inflammatory and occasionally neoplastic conditions, as for the genitalia. Pruritus ani is common in middle-aged men. Whatever the underlying dermatosis, faecal contamination of the perianal skin with bacteria, enzymes and allergens causes inflammation and itch. Persistent rubbing induces lichen simplex (p. 39) or maceration, and secondary infection with bacteria or fungi. A compounding contact dermatitis due to allergy to ‘over-the-counter’ creams is common. Anal carcinoma, fissure or haemorrhoids, and threadworm infestation in children, should be excluded.
[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
Genitourinary medicine
In the UK and Ireland, genitourinary medicine has traditionally been a separate specialty from dermatology, but the two are combined as ‘dermatovenereology’ in many countries. It has become increasingly important for those treating skin disease to know more about genitourinary disorders. Genitourinary diseases range as follows (see also Table 1): syphilis, gonorrhoea, human immunodeficiency virus (HIV) infection (p. 56), chlamydial infection, pelvic inflammatory disease, vaginitis, chancroid viral warts (p. 52), genital herpes simplex (p. 54), hepatitis B and hepatitis C, vulval/perianal dermatoses, penile/scrotal dermatoses.
Syphilis (lues)
Clinical presentation
Primary chancre. About 3 weeks after sexual contact, a primary chancre, a painless ulcerated button-like papule, develops at the site of inoculation. This is usually genital (Fig. 1), but oral and anal chancres are seen in men who have sex with men. Regional lymphadenopathy is common. Without treatment, the chancre clears spontaneously in 3–10 weeks. Serology is not positive until 4 weeks after infection, but spirochaetes can be isolated from the chancre.
Secondary stage. This phase starts 4–10 weeks after the onset of the chancre. It is characterized by a non-itchy pink or copper-coloured papular eruption on the trunk, limbs, palms and soles (p. 42). Untreated, the eruption resolves in 1–3 months. Serology is positive.
Tertiary stage. About 30% of patients with untreated syphilis will develop late lesions, usually after a latent period of years. Painless nodules, sometimes with scaling, develop in annular or arcuate patterns on the face or back. Subcutaneous granulomatous gumma – usually on the face, neck or calf – ulcerate, scar and never heal completely (Fig. 2). Cardiovascular syphilis and neurosyphilis may coexist.
[/not-level-membership-for-dermatology-category]
