CHAPTER 1 General Setup and Techniques
Definition and Philosophy
A VATS procedure is not a compromise operation; it is the same operation that can be performed by a thoracotomy.1,2 The standard operation is performed with visualization on a monitor and through incisions without spreading the ribs. Procedures such as a video-assisted lobectomy provide the same complete cancer operation that is performed through a thoracotomy.3–12
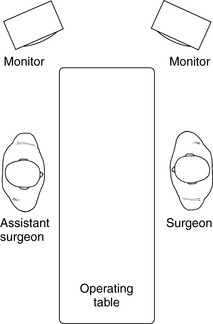
Positioning
Incisions
Placement of the incisions (Figure 1-2) is key to the performance of VATS. Proper placement of the incisions creates the best angles for the instruments to perform these procedures.
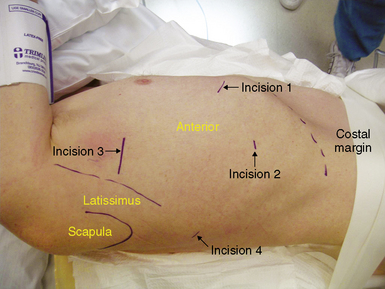
Incision 1
Incision 2
Incision 3
Instruments

Visualization and Lenses
Operative Techniques and Complications
Decompression of the Lung



Hypoxia During Video-Assisted Thoracic Surgery
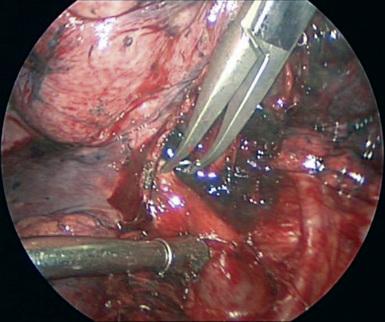
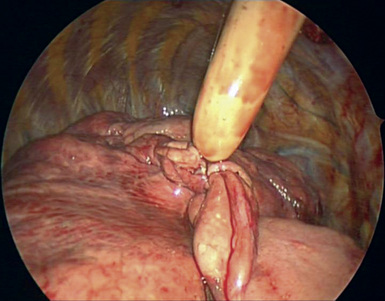
Dissection
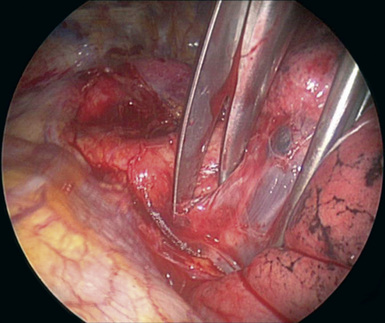
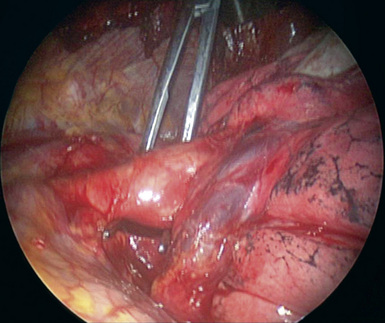
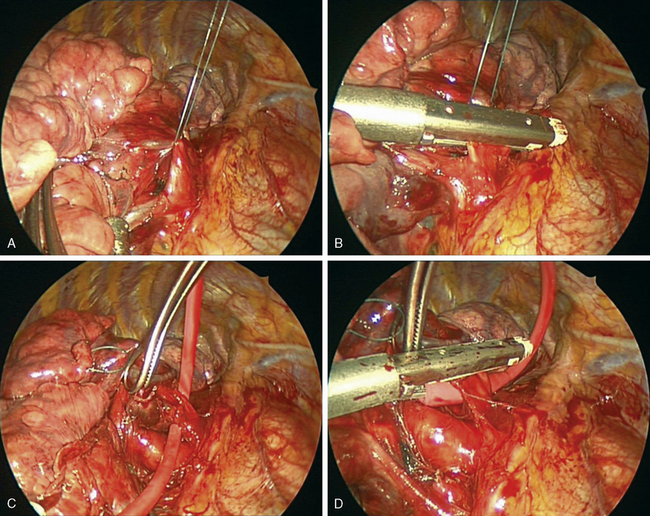
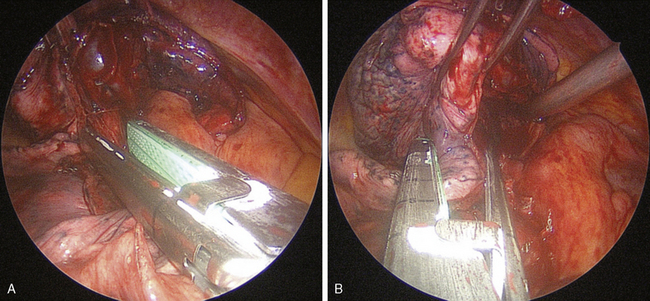
Stapling Blood Vessels
 Usually, passing the stapler from the proper angle allows the anvil of the stapler to pass through the tunnel behind the vessel.
Usually, passing the stapler from the proper angle allows the anvil of the stapler to pass through the tunnel behind the vessel.

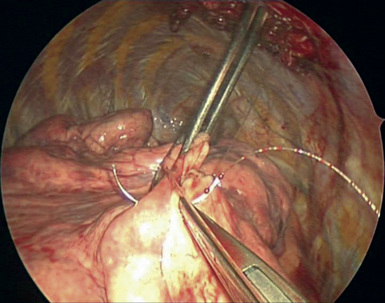
Alternative Techniques for Vessels
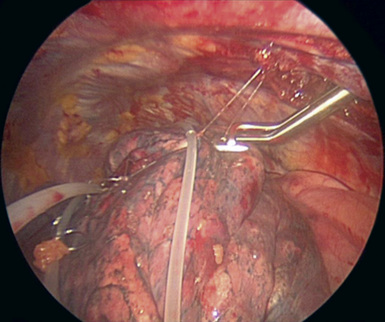
Stapling Parenchyma
Suturing
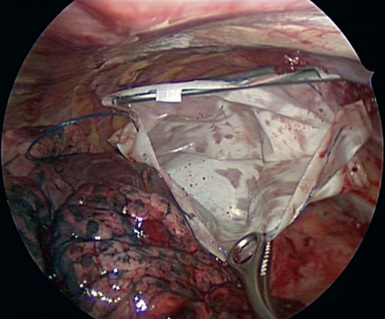
Removal of Specimens
1 McKenna R.J.Jr, Houck W., Fuller C.B. Video-assisted thoracic surgery lobectomy: experience with 1100 cases. Ann Thorac Surg. 2006;81:421-426.
2 Onaitis M.W., Petersen R.P., Balderson S.S., et al. Thoracoscopic lobectomy is a safe and versatile procedure: experience with 500 consecutive patients. Ann Surg. 2006;244:420-425.
3 Mahtabifard A., Fuller C.B., McKenna R.J.Jr. VATS sleeve lobectomy. Ann Thorac Surg. 2008;85(2):5279-5332.
4 McKenna R.J.Jr, Mahtabifard A., Fuller C.B. Fast tracking after VATS pulmonary resection. Ann Thorac Surg. 2007;84(5):1663-1667.
5 Cerfolio R.J., Bass C., Katholi C.R. Prospective, randomized trial compares suction versus water seal for air leaks. Ann Thorac Surg. 2002;73:1727-1731.
6 Whitson B.A., Boettcher A., Bardales R., Kratzke R.A., Dahlberg P.S., Andrade R.S., Maddaus M.A. Comparison of video assisted thoracoscopic surgery to thoracotomy for resection of clinical stage I non-small cell lung cancer. Presented at the American College of Surgeons Congress, Chicago, IL, October 10; 2006.
7 Nomori H., Ohtsuka T., Horio H., et al. Difference in the impairment of vital capacity and 6-minute walking after a lobectomy performed by thoracoscopic surgery, an anterior limited thoracotomy, an antero-axillary thoracotomy, and a posterolateral thoracotomy. Surg Today. 2003;33:7-12.
8 Nakata M., Saeki H., Yokoyama N., et al. Pulmonary function after lobectomy: video-assisted thoracic surgery versus thoracotomy. Ann Thorac Surg. 2000;70:938-941.
9 Demmy T.L., Curtis J.J. Minimally invasive lobectomy directed toward frail and high-risk patients: a case-control study. Ann Thorac Surg. 1999;68:194-200.
10 Demmy T.L., Plante A.J., Nwogu C.E., et al. Discharge independence with minimally invasive lobectomy. Am J Surg. 2004;188:698-702.
11 Nakajima J., Takamoto S., Kohno T., Ohtsuka T. Costs of videothoracoscopic surgery versus open resection for patients with lung carcinoma. Cancer. 2000;89(Suppl):2497-2501.
12 Petersen R.P., Pham D., Burfeind W.R., et al. Thoracoscopic lobectomy facilitates the delivery of chemotherapy after resection for lung cancer. Ann Thorac Surg. 2007;83:1245-1249. discussion 1250






