SECTION I GENERAL APPROACH TO HISTORY AND EXAMINATION
NERVOUS SYSTEM – EXAMINATION
Neurological disease may produce systemic signs and systemic disease may affect the nervous system. A complete general examination must therefore accompany that of the central nervous system. In particular, note the following
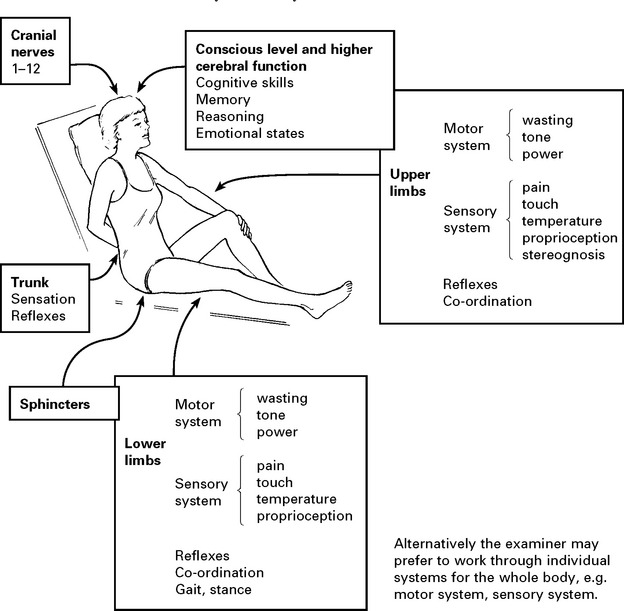
CNS examination is described systematically from the head downwards and includes:
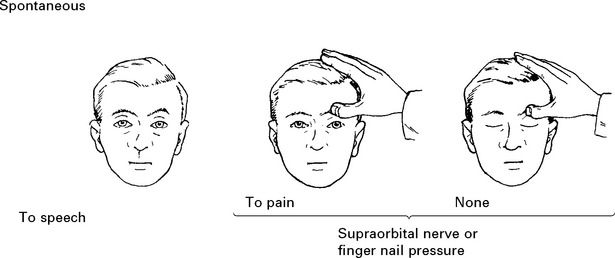
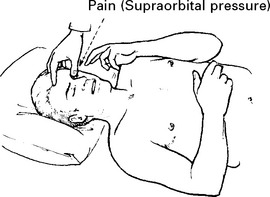
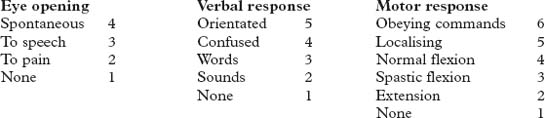
MOTOR RESPONSE – 5 categories


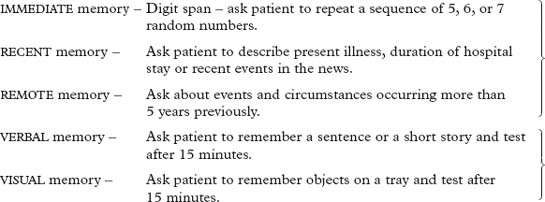
EXAMINATION – HIGHER CEREBRAL FUNCTION
COGNITIVE SKILL
e.g. ‘Hold up both arms, touch the right ear with the left fifth finger.’
Non-dominant hemisphere disorders
| Note patient’s ability to find his way around the ward or his home. | Geographical agnosia |
| Can the patient dress himself? | Dressing apraxia |
| Note the patient’s ability to copy a geometric pattern, e.g. ask patient to form a star with matches or copy a drawing of a cube. | Constructional apraxia |
Mini Mental Status Examination (MMSE) is used in the assessment of DEMENTIA (page 127).
REASONING AND PROBLEM SOLVING
Ask patient to reverse 3 or 4 random numbers.
Ask patient to explain proverbs.
CRANIAL NERVE EXAMINATION
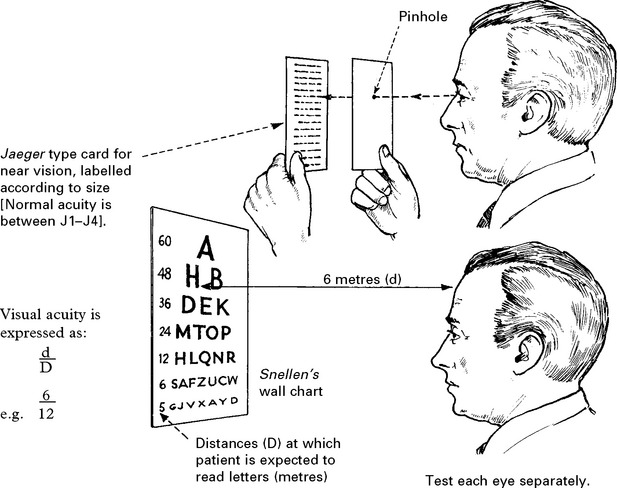
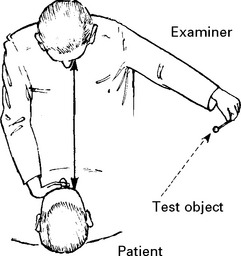
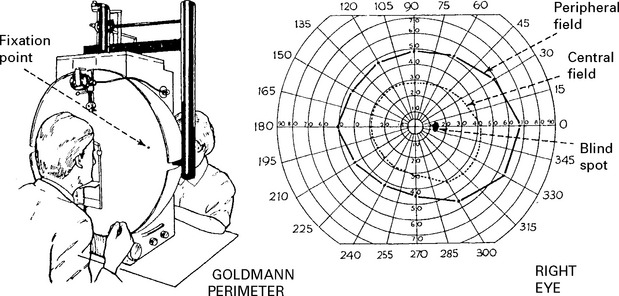
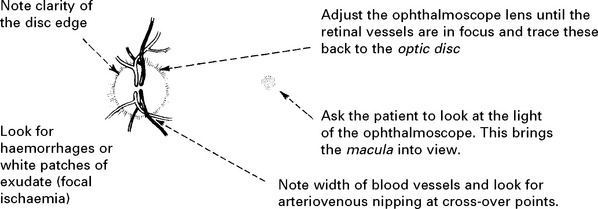
OPTIC NERVE (II)

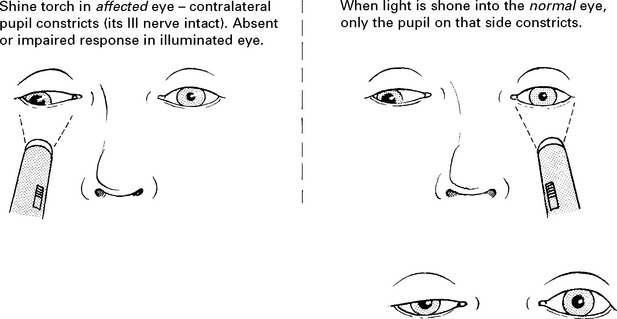
OCULOMOTOR (III), TROCHLEAR (IV) AND ABDUCENS (VI) NERVES
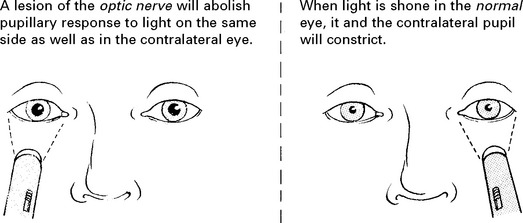
Pupil: The pupil dilates and becomes ‘fixed’ to light.
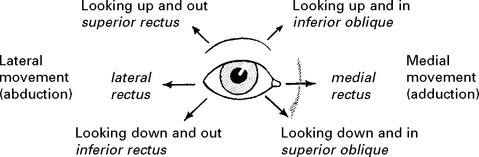
Ocular movement

Note any malalignment or limitation of range.
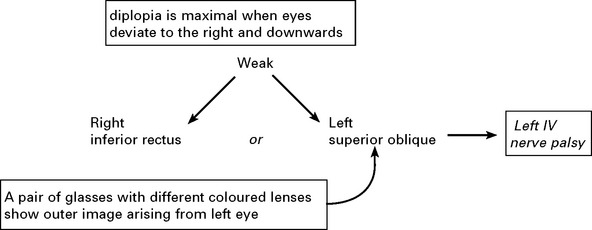
Question patient about diplopia; the patient is more likely to notice this before the examiner can detect impairment of eye movement. If present:
e.g.

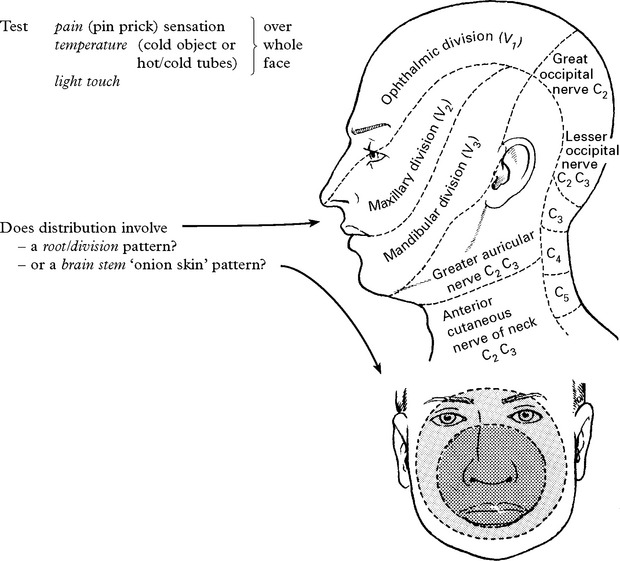
TRIGEMINAL NERVE (V)
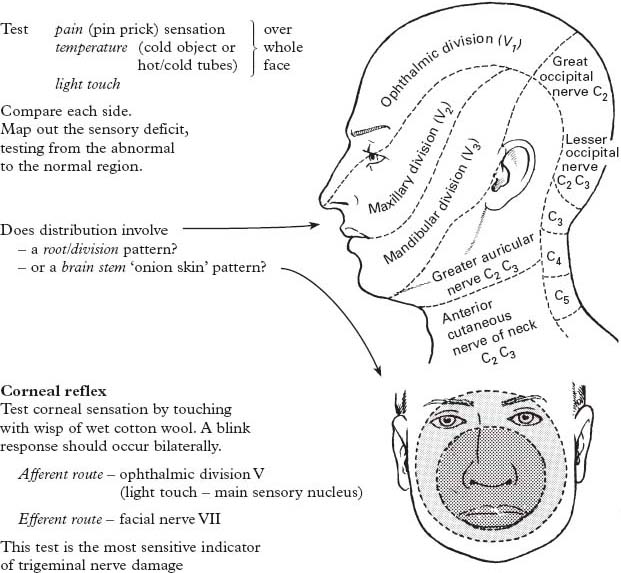
Compare each side. Map out the sensory deficit, testing from the abnormal to the normal region.
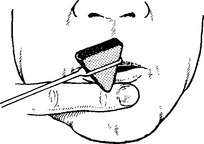
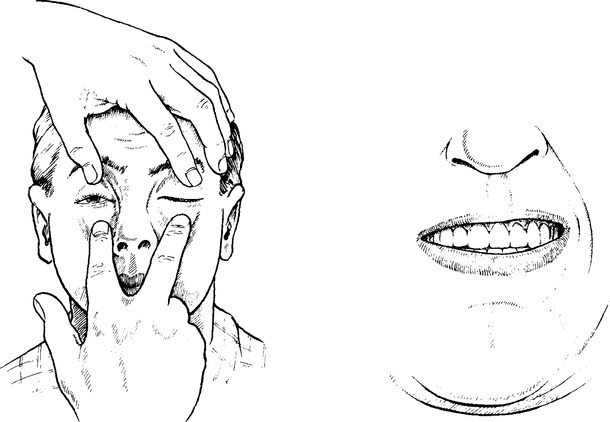
FACIAL NERVE (VII)
Observe patient as he talks and smiles, watching for:
AUDITORY NERVE (VIII)
Cochlear component
Differentiate conductive (middle ear) deafness from perceptive (nerve) deafness by:
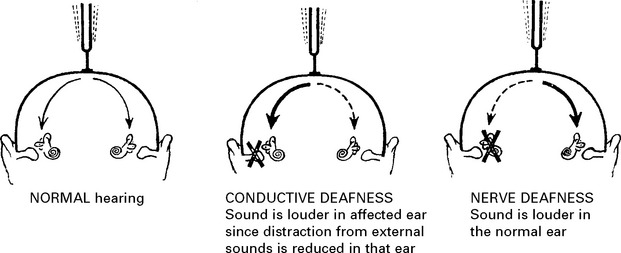
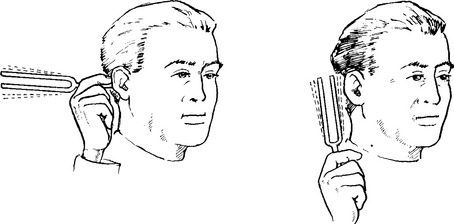
In conductive deafness, bone conduction is better than air conduction.
In nerve deafness, both bone and air conduction are impaired.
Further auditory testing and examination of the vestibular component requires specialised investigation (see pages 62–65).
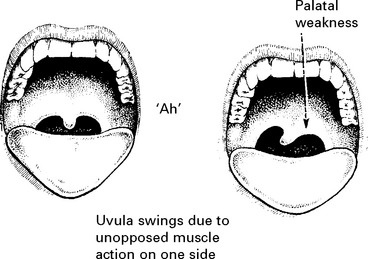
GLOSSOPHARYNGEAL NERVE (IX): VAGUS NERVE (X)
Note any swallowing difficulty or nasal regurgitation of fluids.
Ask patient to open mouth and say ‘Ah’. Note any asymmetry of palatal movements (X nerve palsy).
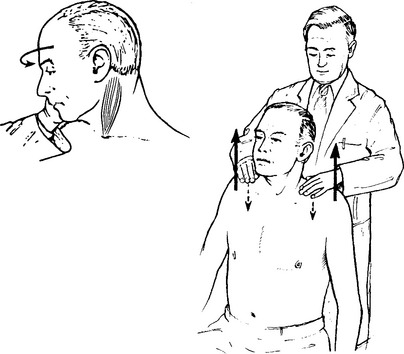
ACCESSORY NERVE (XI)

EXAMINATION – UPPER LIMBS
MOTOR SYSTEM
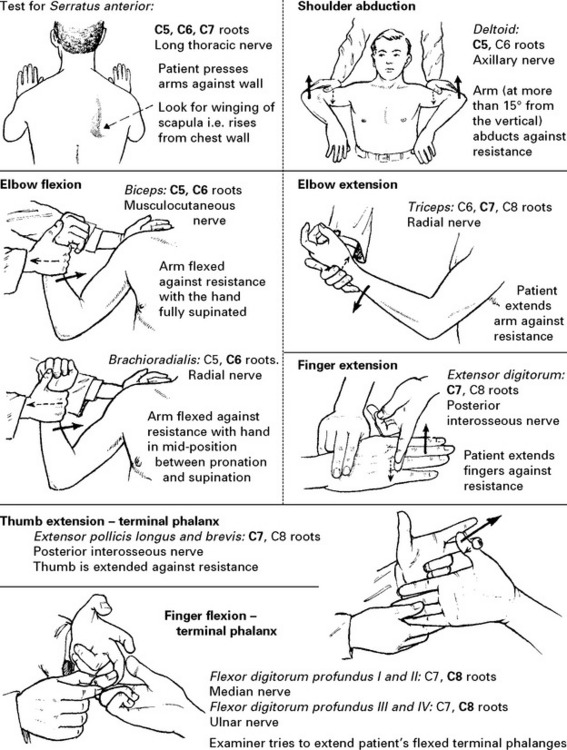
Power
Muscle weakness. The degree of weakness is ‘scored’ using the MRC (Medical Research Council) scale.
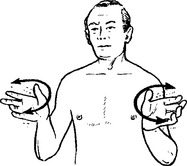
If a pyramidal weakness is suspect (i.e. a weakness arising from damage to the motor cortex or descending motor tracts (see pages 193–198) the following test is simple, quick, yet sensitive.
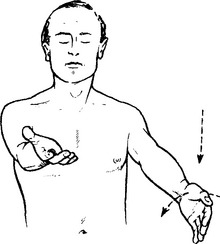
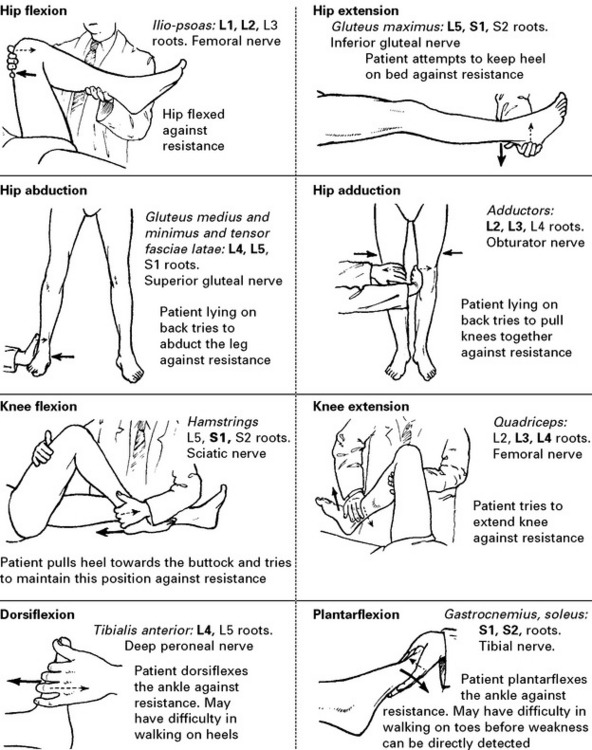
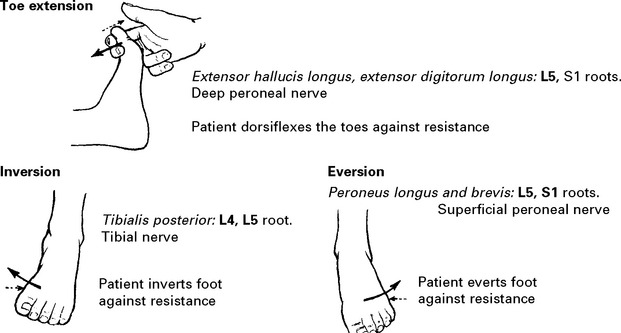
When testing muscle groups, think of root and nerve supply.
SENSATION
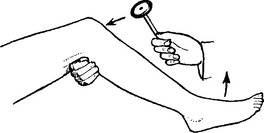
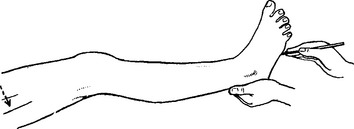
Joint position sense

Hold the sides of the patient’s finger or thumb and demonstrate ‘up and down’ movements.
Repeat with the patient’s eyes closed. Ask patient to specify the direction of movement.

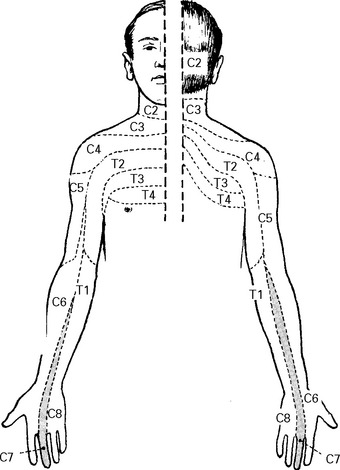
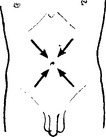
EXAMINATION – TRUNK
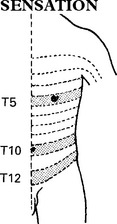
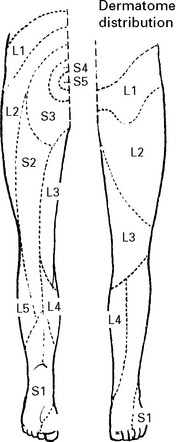
Test pin prick and light touch in dermatome distribution as for the upper limbs.
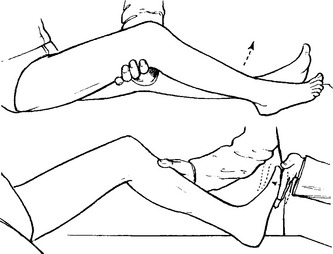
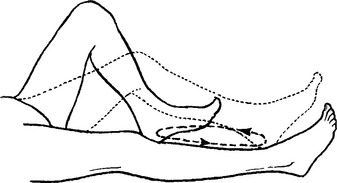
EXAMINATION – LOWER LIMBS
MOTOR SYSTEM






EXAMINATION OF THE UNCONSCIOUS PATIENT
GENERAL EXAMINATION
Lack of patient co-operation does not limit general examination and this may reveal important diagnostic signs. In addition to those features described on page 4, also look for signs of head injury, needle marks on the arm and evidence of tongue biting. Also note the smell of alcohol, but beware of attributing the patient’s clinical state solely to alcohol excess.
NEUROLOGICAL EXAMINATION
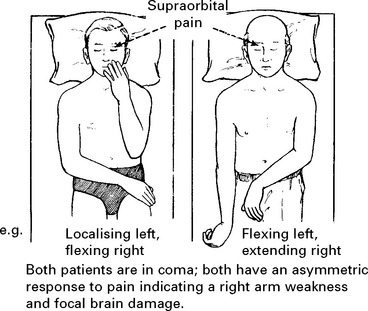
Conscious level: This assessment is of major importance. It not only serves as an immediate prognostic guide, but also provides a baseline with which future examinations may be compared. Assess conscious level as described previously (page 5) in terms of eye opening, verbal response and motor response.
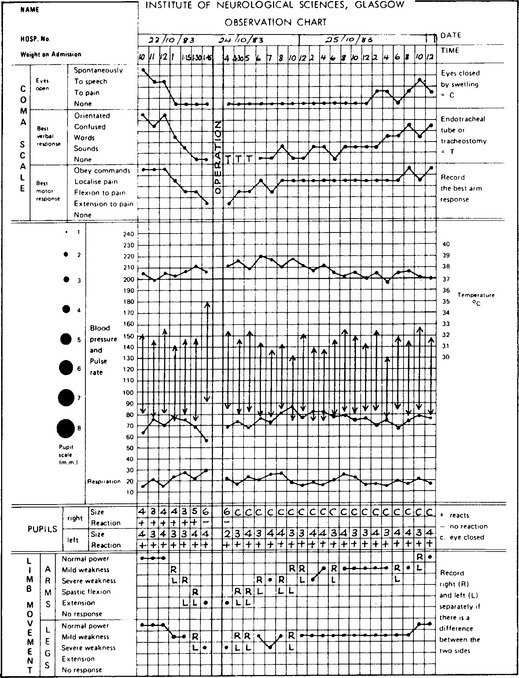
For research purposes, a score was applied for each response, with ‘flexion’ subdivided into ‘normal’ and ‘spastic flexion’, giving a total coma score of ‘15 points’. Many coma observation charts (page 31) still use a ‘14 point scale’ with 5 points on the motor score. The ‘14 point’ scale records less observer variability, but most guidelines for head injury management use the ‘15 point’ scale.

Eye movements
Observe any spontaneous eye movements.

Elicit the oculocephalic (doll’s eye) reflex.
Elicit the oculovestibular reflex (caloric testing, see page 65).