CHAPTER 14 GASTROINTESTINAL PATHOLOGY





ESOPHAGUS
HISTOLOGICAL VARIANTS OF NORMAL ESOPHAGUS



ESOPHAGEAL ATRESIA AND TRACHEO-ESOPHAGEAL FISTULA









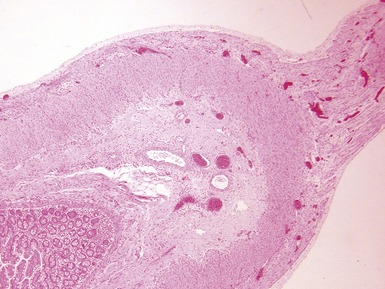
Histopathological features (Dutta, Mathur, Bhatnagar 2000)
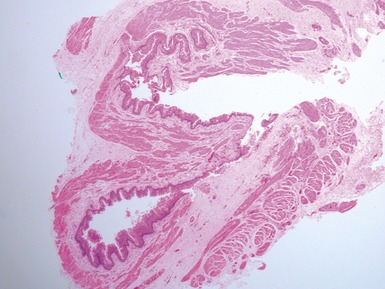
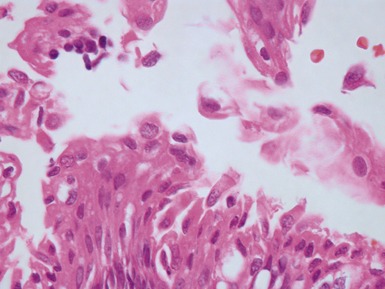
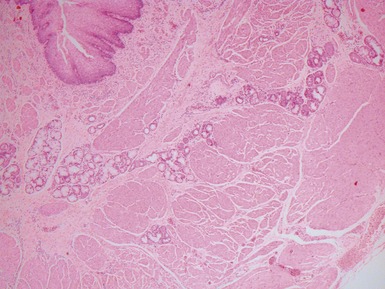
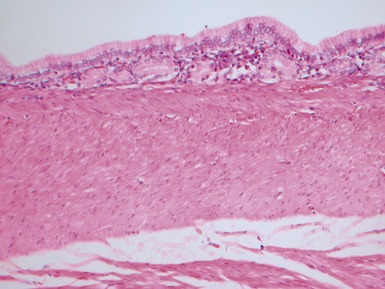
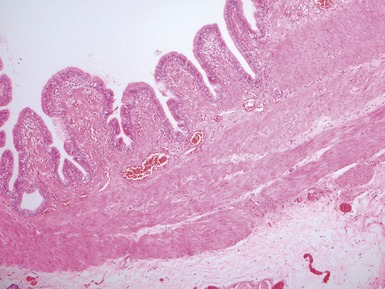
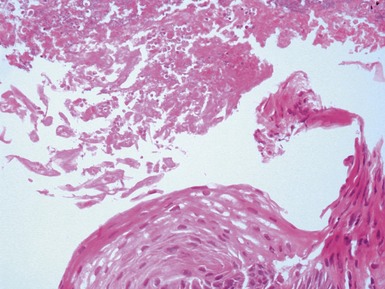
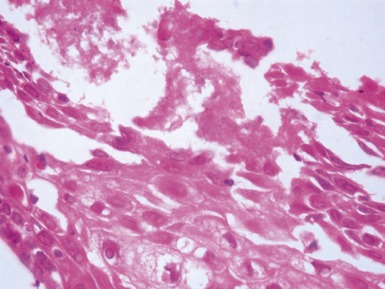
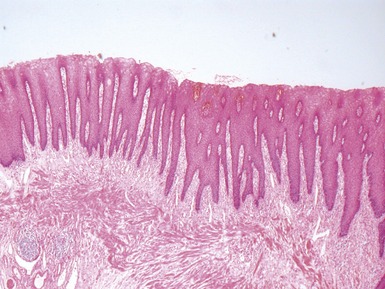
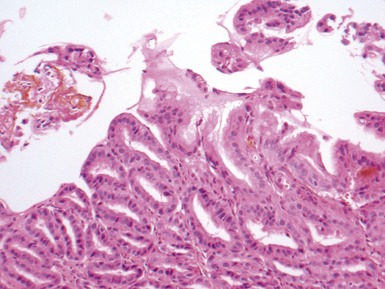
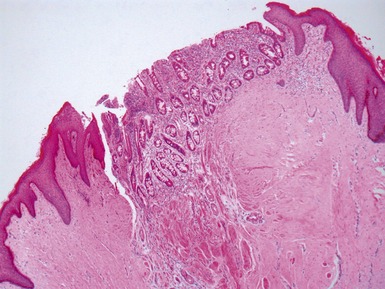
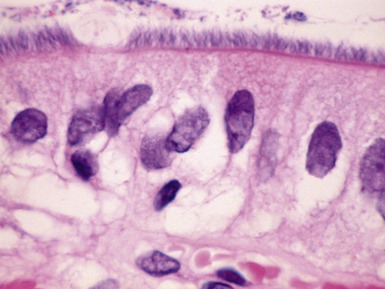
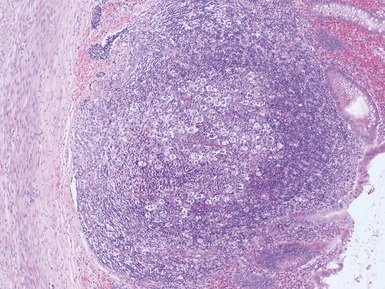
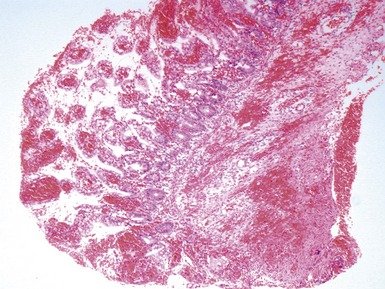
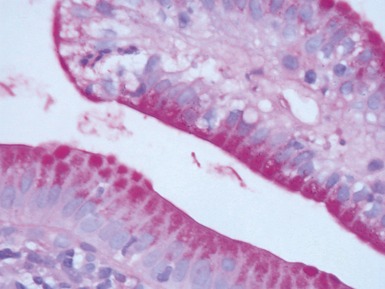
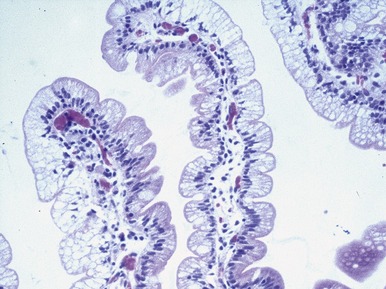
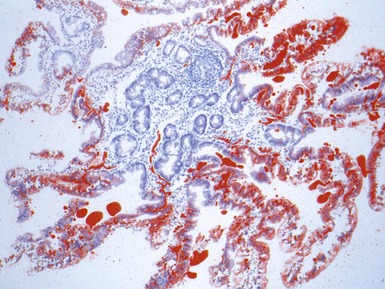
Fig 14.2 One-day-old girl with esophageal atresia and tracheo-esophageal fistula. The specimen is the tip of the proximal esophageal pouch. Photomicrograph of the specimen demonstrating the pouch comprising the usual elements of esophageal wall. The mucosa shows some ciliated epithelium. Unusually, no striated muscle was present in the muscular coat.








GASTRO-ESOPHAGEAL REFLUX DISEASE









COLUMNAR EPITHELIAL LINED ESOPHAGUS (CELE)



















INFECTIVE ESOPHAGITIS






























CROHN’S DISEASE OF THE ESOPHAGUS









STOMACH

GASTRITIS


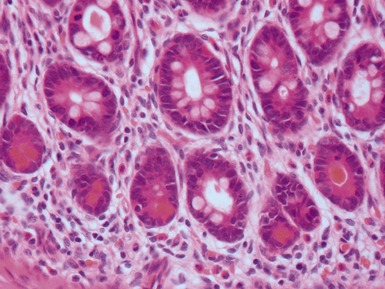
Helicobacter pylori gastritis




Crohn’s disease associated gastritis




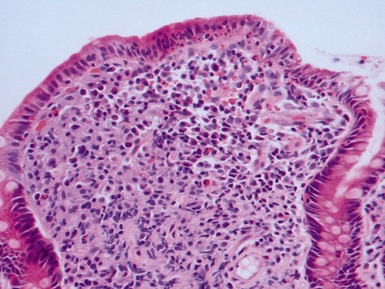
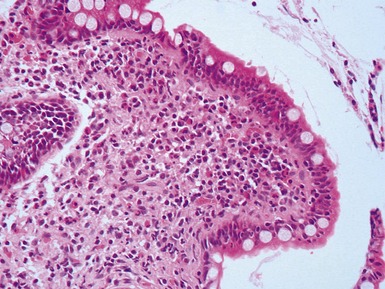
Lymphocytic gastritis


























SMALL INTESTINE
INTESTINAL ATRESIA















MECKEL’S DIVERTICULUM














DUPLICATION CYSTS



INTUSSUSCEPTION





















VOLVULUS








MECONIUM ILEUS






Histopathological features



CROHN’S DISEASE


















INTESTINAL INFECTIONS




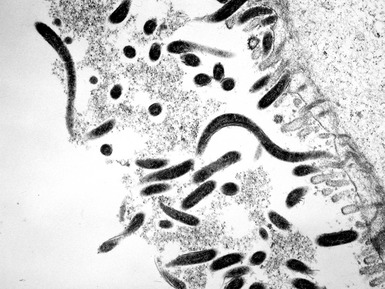
Cryptosporidiosis





Astrovirus















NEONATAL NECROTIZING ENTEROCOLITIS













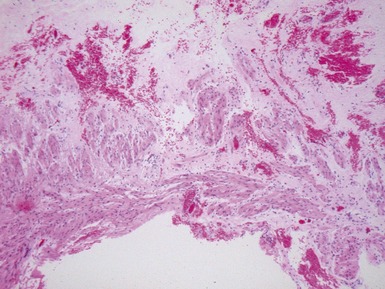
Histopathological features








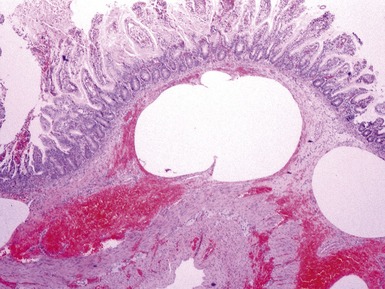
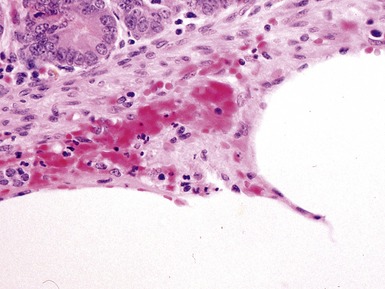
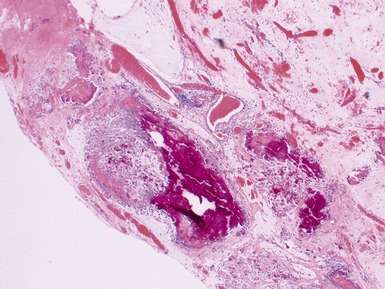
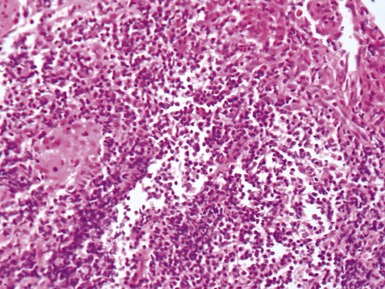
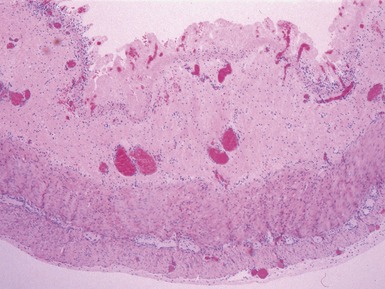
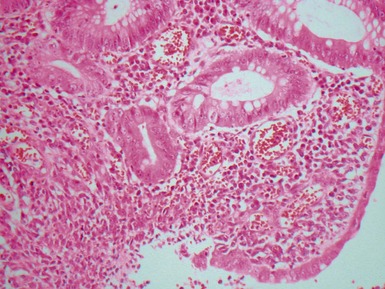
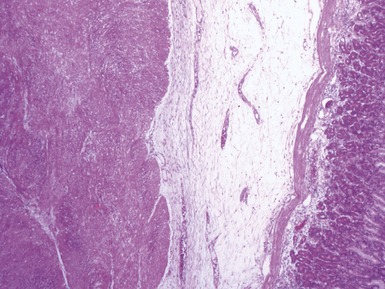
Fig 14.52 Necrotizing enterocolitis. Photomicrograph at a higher power of the same lesion as in Fig 14.51 demonstrating the edge of one of the gas-filled areas. There is hemorrhage and a neutrophil polymorph infiltrate.

FOOD ALLERGY



PRIMARY INTESTINAL FAILURE / NEONATAL-INFANTILE ENTEROPATHIES

















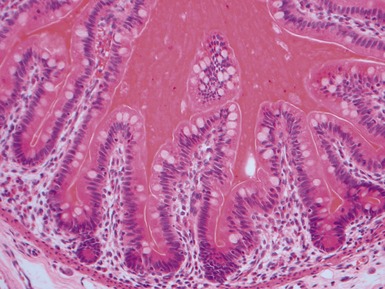
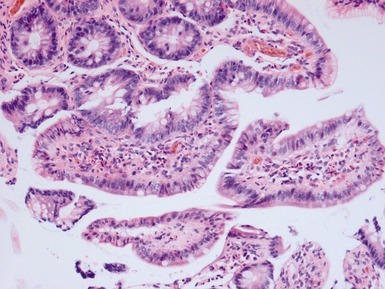
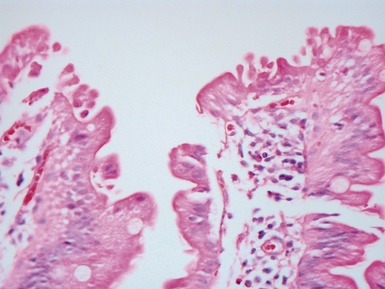
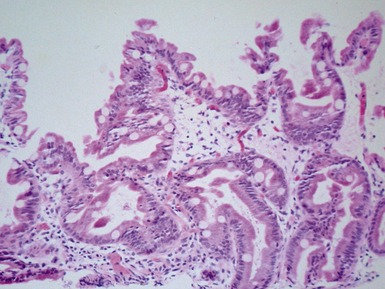
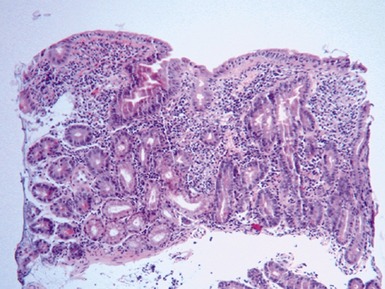
CELIAC DISEASE (GLUTEN SENSITIVE ENTEROPATHY)

Clinical features (Fasano et al 2008)










Histopathological features








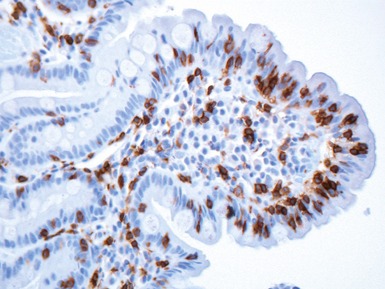
Differential diagnosis and diagnostic pitfalls











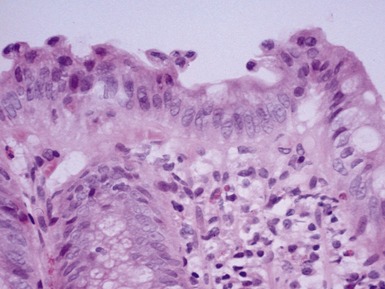
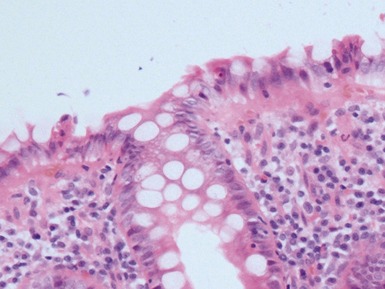
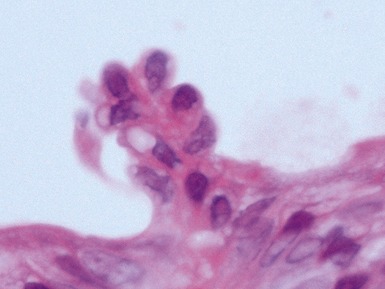
TUFTING ENTEROPATHY




Histopathological features




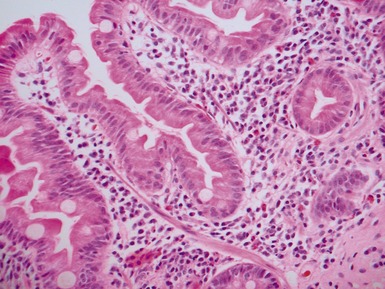
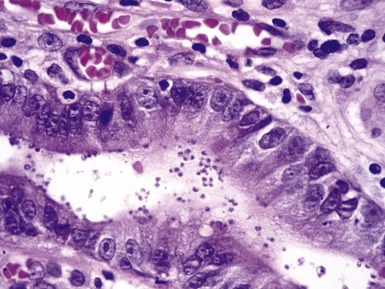
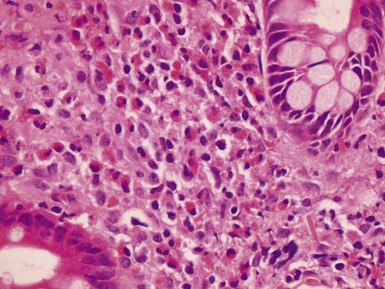
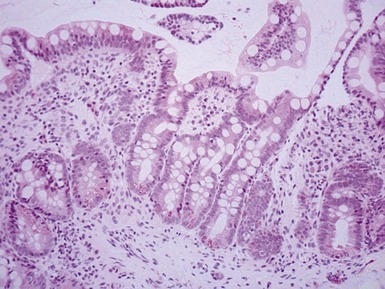
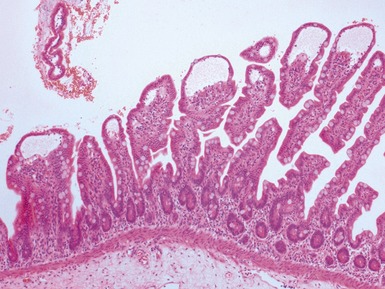
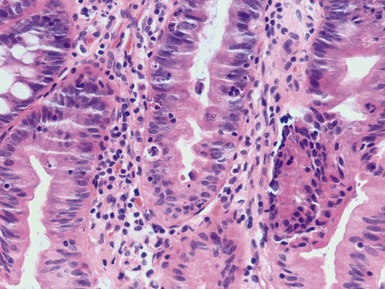
Fig 14.60 Tufting enteropathy inflammation. Photomicrograph demonstrating partial villous atrophy and an acute and chronic inflammatory cell infiltrate in the mucosa. No tufts are present in this field. The degree of inflammation present is very variable, but some degree is usually present.







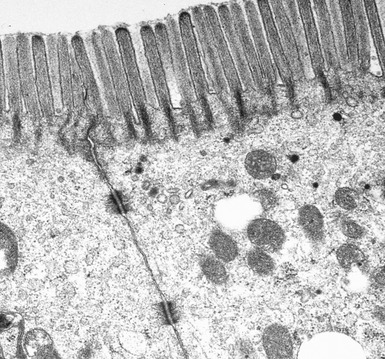
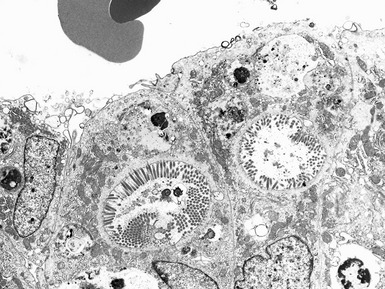
MICROVILLOUS INCLUSION DISEASE







DISSACHARIDASE ASSESSMENT OF JEJUNAL SPECIMENS







ABETALIPOPROTEINEMIA





PATHOLOGY OF INTESTINAL TRANSPLANTATION




























GASTROINTESTINAL NEUROMUSCULAR / MOTILITY DISEASES
Introduction











Investigation of intestinal motility disorders













ACHALASIA OF ESOPHAGUS











HYPERTROPHIC PYLORIC STENOSIS


Differential diagnosis of infantile gastric outlet obstruction




HIRSCHSPRUNG’S DISEASE (HSCR)
Genetics






































































Clinical features










Histopathological features






Primary diagnosis on rectal suction biopsy















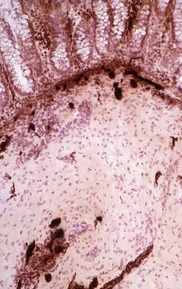
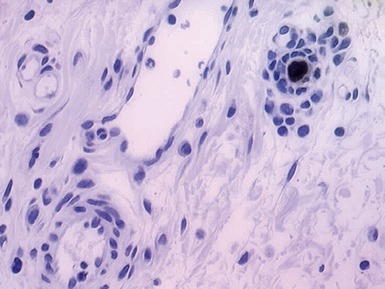
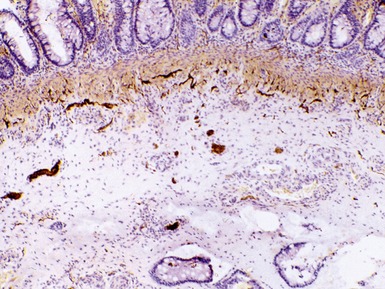
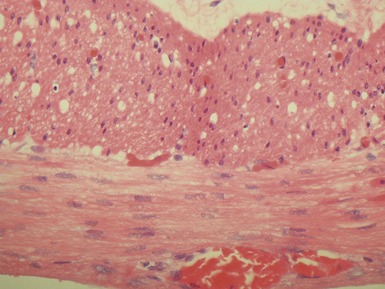
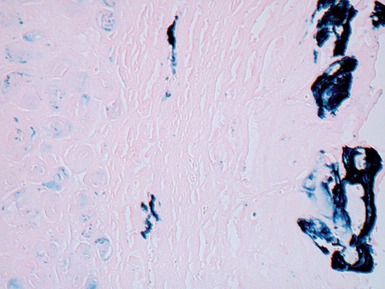
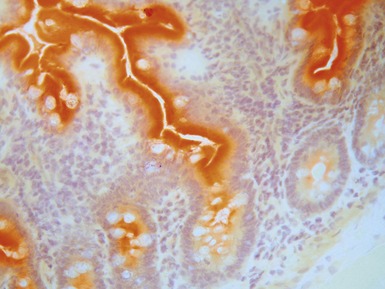
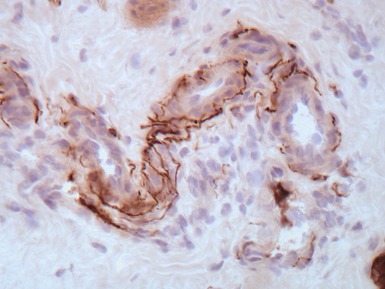
Fig 14.84 Photomicrograph of frozen section of normal rectal suction biopsy stained to display acetylcholinesterase activity demonstrating occasional fine nerves in the muscularis mucosae and lamina propria.
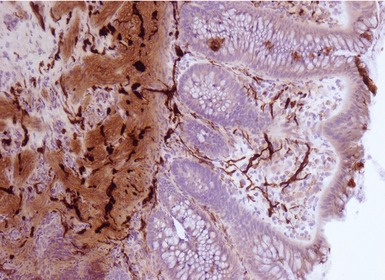

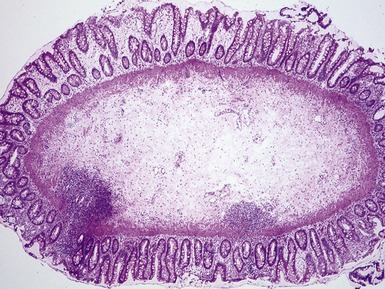
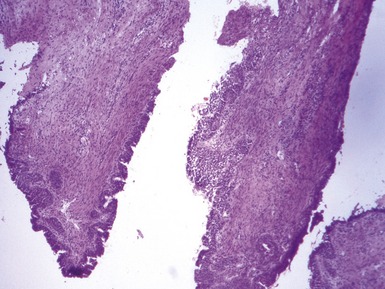
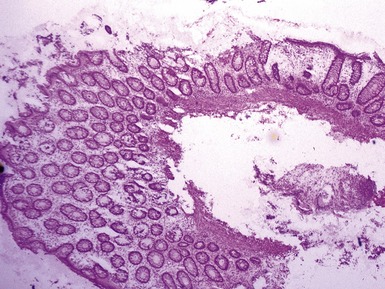
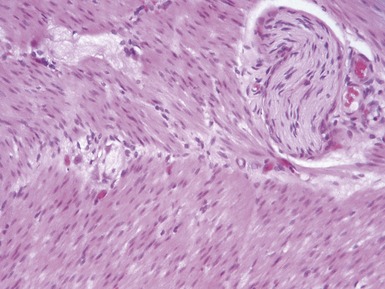
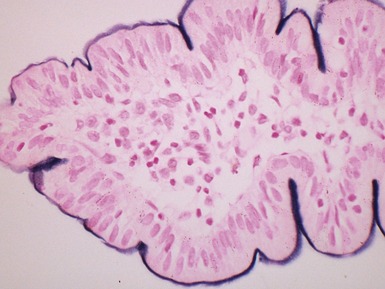
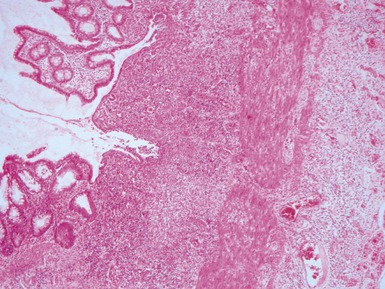
Fig 14.87 Photomicrograph of adequate rectal suction biopsy demonstrating large submucosal surface area.
Urgent







Differential diagnosis and diagnostic pitfalls
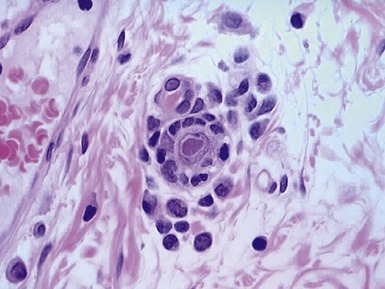
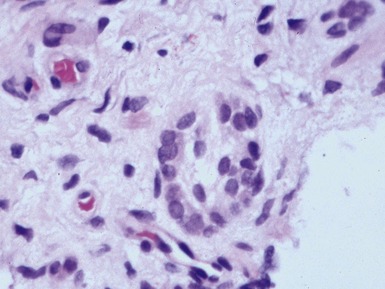
Identification of ganglion cells




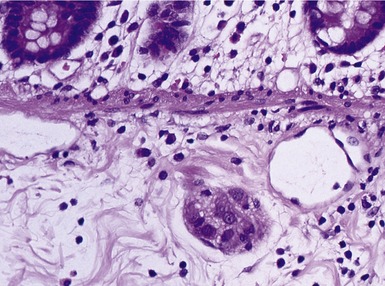
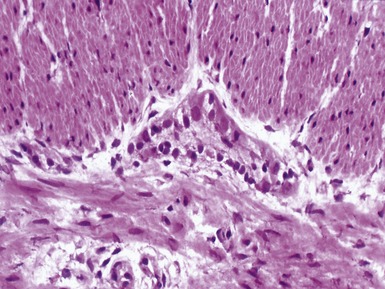
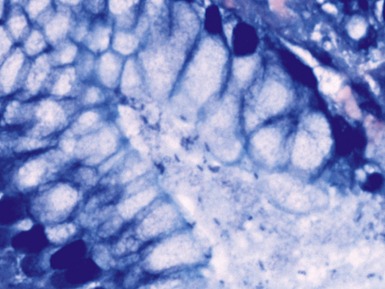
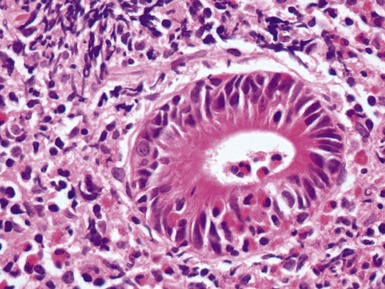
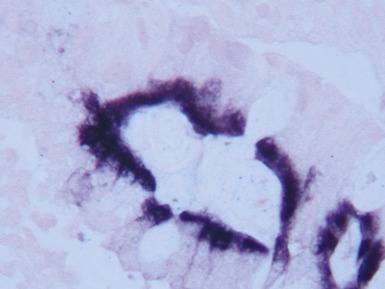
Fig 14.89 Photomicrograph of frozen section of rectal suction biopsy demonstrating normal submucosal ganglion cells. Note cluster of six cells with basophilic cytoplasm and prominent eccentric nucleus. Most do not show a nucleolus, a feature which is typical of neonatal specimens. Note also fine fibrillary neuropil and satellite cell nuclei.