Near gastroesophageal (GE) junction, on posterior aspect of lesser curvature of stomach
• Usually 1-3 cm, up to 10 cm in diameter
• On upper GI series
Barium-filled diverticulum with air-fluid level
• CT findings
Often in suprarenal location
– Mimics adrenal or pancreatic mass
Connection to stomach may be subtle
Air-filled, fluid-filled, or contrast-filled mass
No enhancement of contents
TOP DIFFERENTIAL DIAGNOSES
• Adrenal mass
• Pancreatic tumor
• Abdominal abscess
• Ectopic pancreatic tissue
PATHOLOGY
• Pouch/sac includes 3 normal layers of bowel wall: Mucosa, submucosa, and muscularis propria
CLINICAL ISSUES
• Complications (rare)
Bleeding
Ulceration
Carcinoma
• No treatment needed unless complications occur
DIAGNOSTIC CHECKLIST
• Incidental finding that may be mistaken for adrenal mass on CT or MR
Barium studies or CT in supine and prone position with oral contrast and gas granules will differentiate diverticulum from mass
(Left) Upright film from an upper GI series shows a typical gastric diverticulum with an air-contrast level seen within an outpouching near the gastric cardia.
(Right) Axial CECT in the same patient shows a near water density mass projecting posterior to the gastric fundus . The connection to the stomach is much more difficult to see on CT. Distention of the stomach with oral contrast or gas granules may be required to make the diagnosis on a CT scan.
(Left) CECT shows an oval mass containing water density fluid and gas. On more cephalic sections, the “mass” was contiguous with the posterior wall of the fundus.
(Right) On a slightly more inferior image, note how the diverticulum extends dorsal to the pancreas and splenic vein. Without the presence of the air-fluid level it would be difficult to distinguish this from an adrenal mass. An upper GI series confirmed a typical juxtacardiac diverticulum.
TERMINOLOGY
Definitions
• Pouch or sac opening from stomach
IMAGING
General Features
• Best diagnostic clue
Barium-filled diverticulum from fundus, near gastroesophageal (GE) junction
• Other general features
2 types of gastric diverticula
– True gastric diverticula (congenital)
– Intramural or partial gastric diverticula (acquired)
Radiographic Findings
• Fluoroscopic-guided barium studies
True diverticula
– Most (> 75%) are juxtacardiac diverticula: Diverticula near GE junction, on posterior aspect of lesser curvature of stomach
– Usually 1-3 cm, up to 10 cm in diameter
– Barium-filled diverticulum with air-fluid level
– Pooling of barium; mimics ulceration
– In antrum (rare); mimics ulcer craters
Intramural or partial gastric diverticula
– Most are prepyloric diverticula: Diverticula at greater curvature of distal antrum
– Heaped-up area overlying diverticulum; mimics ectopic pancreatic rest on greater curvature
CT Findings
• Abnormal rounded “lesion”
Often in suprarenal location; mimics adrenal mass
Connection to stomach may be subtle
• Air-filled, fluid-filled, or contrast-filled mass
• No enhancement of contents
Imaging Recommendations
• Best imaging tool
Fluoroscopic-guided barium studies
• Protocol advice
Juxtacardiac diverticula are best seen in lateral views on barium studies
Obtain CT in supine and prone position: Air will usually fill diverticulum
DIFFERENTIAL DIAGNOSIS
Adrenal Mass
• CT: Diverticular contents do not enhance, adrenal masses (except cysts) do enhance
• Distinguished by barium studies
Pancreatic Tumor
• e.g., any cystic or solid lesion
Abdominal Abscess
• Air- or fluid-filled mass with thick wall
• Distinguished by clinical history (e.g., fever)
Ectopic Pancreatic Tissue
• May also cause outpouching from antrum within mound of tissue
PATHOLOGY
General Features
• Etiology
True gastric diverticula: Congenital
Intramural or partial gastric diverticula: Acquired
– Associated with peptic ulcer disease, pancreatitis, cholecystitis, malignancy, or outlet obstruction
• Uncommon or rare
0.02% of autopsy specimens
0.04% of upper gastrointestinal series
> 75% of gastric diverticula are juxtacardiac
Gross Pathologic & Surgical Features
• True gastric diverticula
Pouch/sac includes 3 normal layers of bowel wall: Mucosa, submucosa, muscularis propria
CLINICAL ISSUES
Presentation
• Most common signs/symptoms
True gastric diverticula
– Asymptomatic (most common)
– Vague upper abdominal pain
Intramural or partial gastric diverticula
– Asymptomatic, or related to associated diseases (e.g., peptic ulcer)









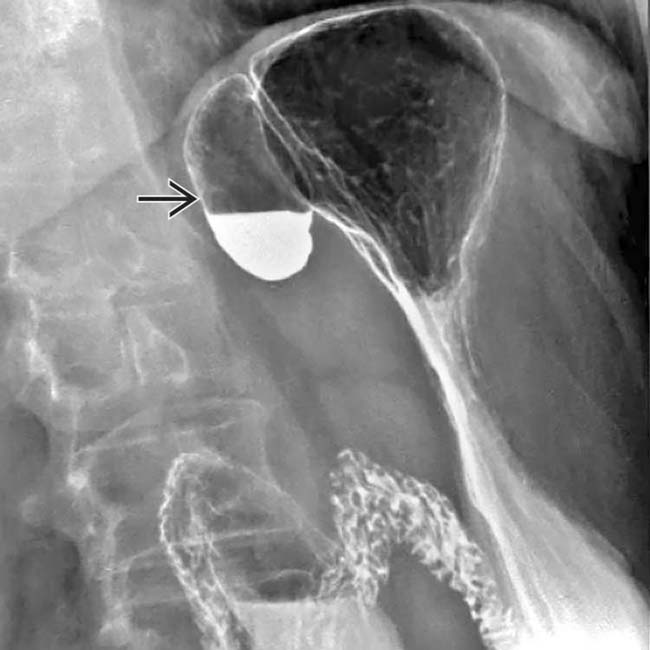
 with an air-contrast level seen within an outpouching near the gastric cardia.
with an air-contrast level seen within an outpouching near the gastric cardia.
 projecting posterior to the gastric fundus
projecting posterior to the gastric fundus  . The connection to the stomach is much more difficult to see on CT. Distention of the stomach with oral contrast or gas granules may be required to make the diagnosis on a CT scan.
. The connection to the stomach is much more difficult to see on CT. Distention of the stomach with oral contrast or gas granules may be required to make the diagnosis on a CT scan.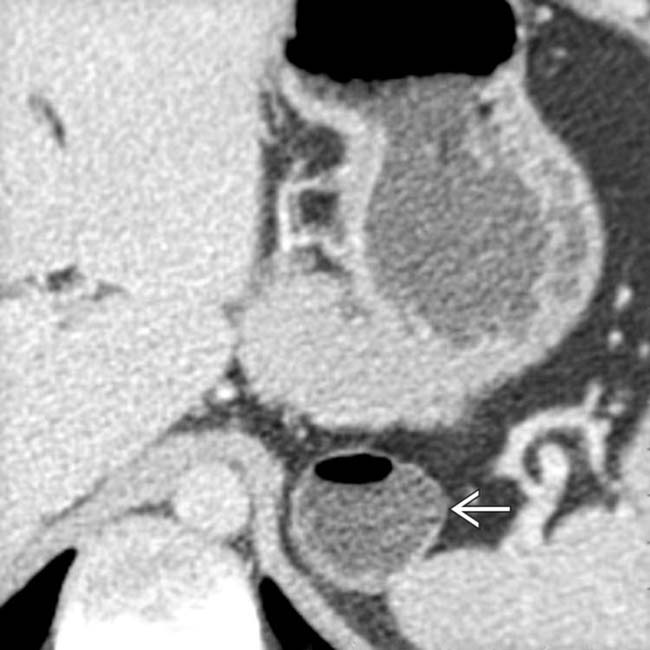
 containing water density fluid and gas. On more cephalic sections, the “mass” was contiguous with the posterior wall of the fundus.
containing water density fluid and gas. On more cephalic sections, the “mass” was contiguous with the posterior wall of the fundus.
 extends dorsal to the pancreas and splenic vein. Without the presence of the air-fluid level it would be difficult to distinguish this from an adrenal mass. An upper GI series confirmed a typical juxtacardiac diverticulum.
extends dorsal to the pancreas and splenic vein. Without the presence of the air-fluid level it would be difficult to distinguish this from an adrenal mass. An upper GI series confirmed a typical juxtacardiac diverticulum.




















 , which lies medial and posterior to gastric fundus.
, which lies medial and posterior to gastric fundus.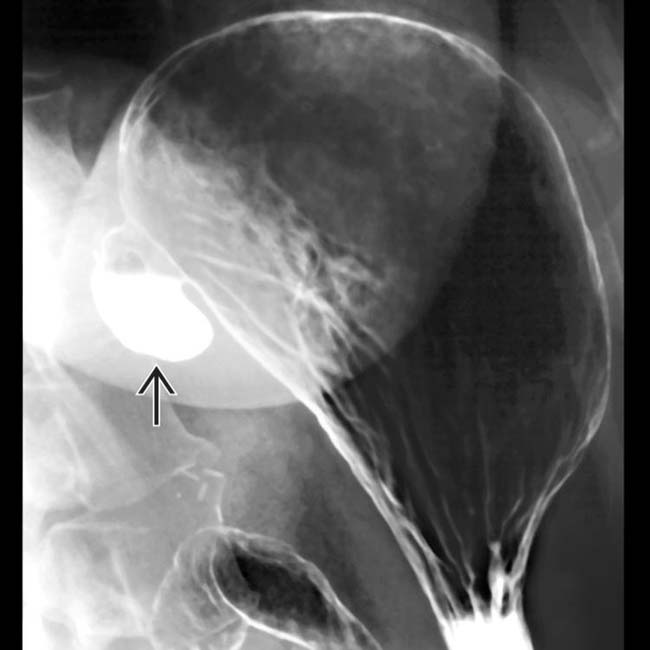
 , arising near the GE junction.
, arising near the GE junction.


