[level-membership-for-radiology-category] Rigler triad of small bowel (SB) obstruction, gas in biliary tree, and ectopic gallstone
• Location: Points of luminal narrowing of bowel; duodenum, ligament of Treitz, ileocecal valve, sigmoid colon
• CT findings
Gallstone surrounded by gas in bowel loop
– Cholesterol stones near-water density, often with calcified rim
Collapsed gallbladder, pneumobilia (gas within GB ± bile duct lumen)
Dilated bowel with transition to collapsed bowel at impacted gallstone
TOP DIFFERENTIAL DIAGNOSES
• Intussusception
• Dropped gallstone (intraperitoneal, not intraluminal)
PATHOLOGY
• Occurs with chronic cholecystitis
• Delayed (up to 2 months) complication of ERCP
• Diagnosis frequently delayed or missed
CLINICAL ISSUES
• Most common signs/symptoms: Intermittent acute colicky abdominal pain (20-30%), nausea, vomiting, fever, distension, obstipation
• Gallstone erodes inflamed GB wall, passes into GI tract (usually duodenum) → bowel obstruction
DIAGNOSTIC CHECKLIST
• Consider in elderly woman with recurrent RUQ pain, recently more severe and prolonged vomiting
(Left) Axial CECT in a 65-year-old woman presenting with crampy abdominal pain demonstrates a thick-walled gallbladder with air within its lumen and a gas-filled fistula to the duodenum .
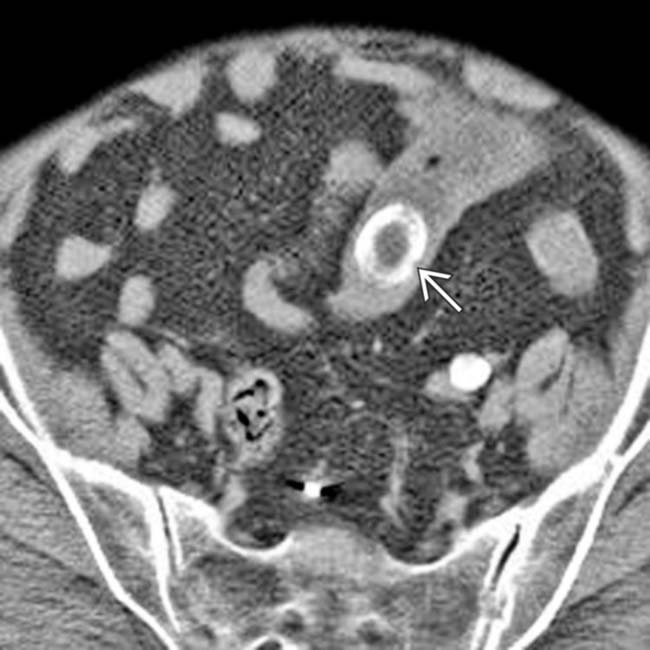
(Right) Axial CECT in the same patient identifies the obstructing gallstone , which is impacted in the distal jejunum. The proximal small bowel is dilated, while the distal SB and colon are collapsed.
(Left) Axial CECT in a patient presenting with bloating and abdominal pain demonstrates gas in the gallbladder , a typical finding in gallstone ileus, also known as gallstone obstruction.
(Right) Axial CECT in the same patient demonstrates dilation of the proximal small bowel and decompressed, nondilated distal small bowel . The high-density obstructing gallstone is seen, as a laminated calcification, at the site of transition from the dilated to the decompressed bowel.
Axial NECT shows gas in the gallbladder adjacent to a large gallstone .
Axial NECT at a more caudal level in the same patient demonstrates a calcified gallstone obstructing the distal small bowel.
Anteroposterior radiograph shows dilated small bowel confirming obstruction, as well as gas in the gallbladder .
Axial CECT shows a dilated proximal small bowel and laminated filling defect at the transition point, which proved to represent an obstructing gallstone.
Axial CECT shows a cholecystoduodenal fistula from a prior episode of GSI. Note the gas in the gallbladder and the close proximity of the GB to the duodenum .
Axial CECT shows gas in a collapsed gallbladder. Note the fistula to the duodenum .
Axial CECT shows a large gallstone within the dilated small bowel. Note that the bowel distal to the gallstone is collapsed.
Axial CECT shows gas in a thick-walled collapsed gallbladder. Note the fistula to the duodenum.
Axial CECT shows small bowel obstruction with a large, laminated gallstone “stuck” near the ileocecal valve.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Rigler triad of small bowel (SB) obstruction, gas in biliary tree, and ectopic gallstone
• Location: Points of luminal narrowing of bowel; duodenum, ligament of Treitz, ileocecal valve, sigmoid colon
• CT findings
Gallstone surrounded by gas in bowel loop
– Cholesterol stones near-water density, often with calcified rim
Collapsed gallbladder, pneumobilia (gas within GB ± bile duct lumen)
Dilated bowel with transition to collapsed bowel at impacted gallstone
TOP DIFFERENTIAL DIAGNOSES
• Intussusception
• Dropped gallstone (intraperitoneal, not intraluminal)
PATHOLOGY
• Occurs with chronic cholecystitis
• Delayed (up to 2 months) complication of ERCP
• Diagnosis frequently delayed or missed
CLINICAL ISSUES
• Most common signs/symptoms: Intermittent acute colicky abdominal pain (20-30%), nausea, vomiting, fever, distension, obstipation
• Gallstone erodes inflamed GB wall, passes into GI tract (usually duodenum) → bowel obstruction
DIAGNOSTIC CHECKLIST
• Consider in elderly woman with recurrent RUQ pain, recently more severe and prolonged vomiting
Buy Membership for Radiology Category to continue reading. Learn more here



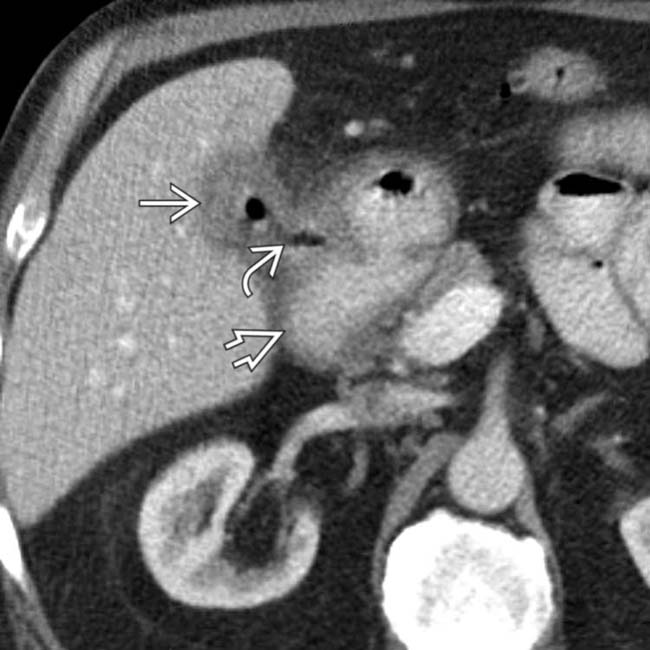
 with air within its lumen and a gas-filled fistula
with air within its lumen and a gas-filled fistula  to the duodenum
to the duodenum  .
.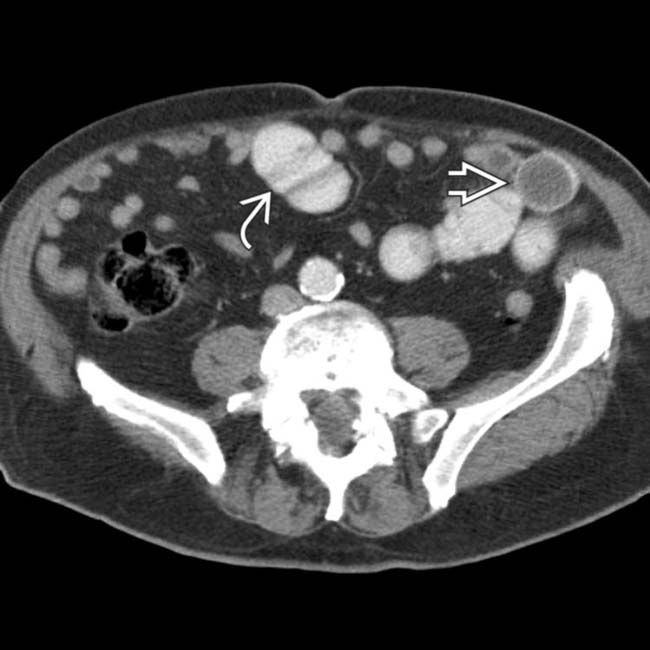
 , which is impacted in the distal jejunum. The proximal small bowel
, which is impacted in the distal jejunum. The proximal small bowel  is dilated, while the distal SB and colon are collapsed.
is dilated, while the distal SB and colon are collapsed.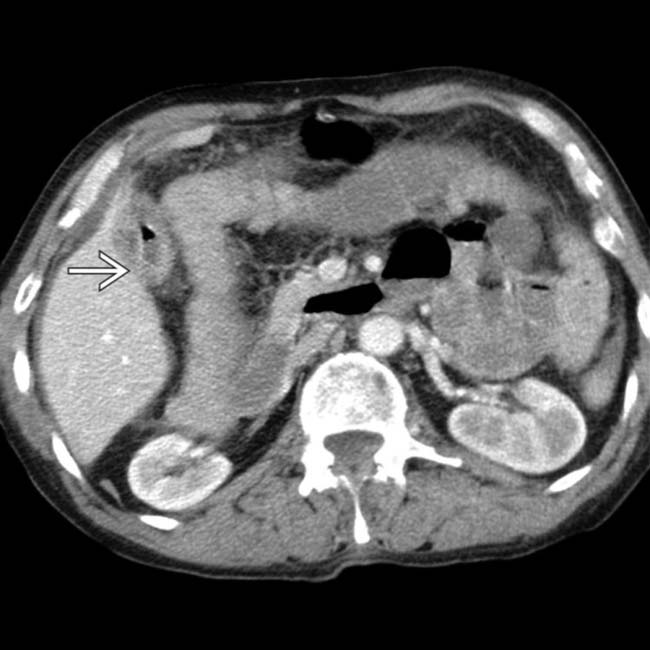
 , a typical finding in gallstone ileus, also known as gallstone obstruction.
, a typical finding in gallstone ileus, also known as gallstone obstruction.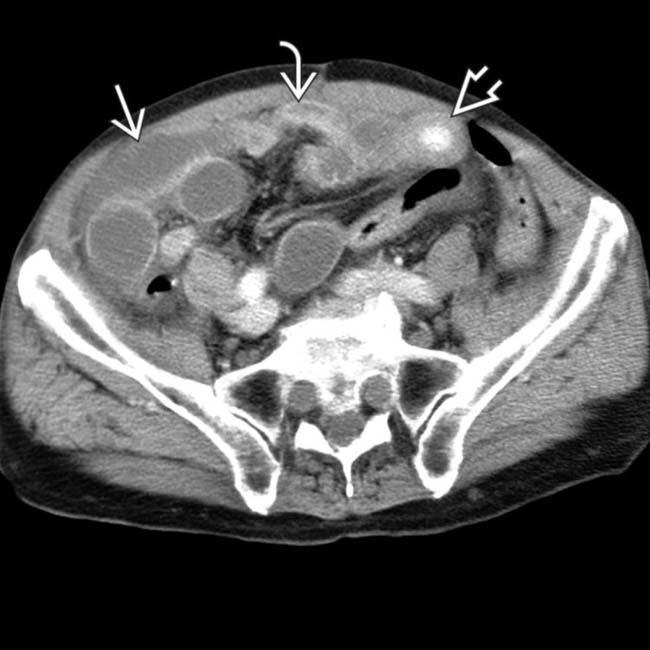
 and decompressed, nondilated distal small bowel
and decompressed, nondilated distal small bowel  . The high-density obstructing gallstone
. The high-density obstructing gallstone  is seen, as a laminated calcification, at the site of transition from the dilated to the decompressed bowel.
is seen, as a laminated calcification, at the site of transition from the dilated to the decompressed bowel.
 .
.
 obstructing the distal small bowel.
obstructing the distal small bowel.
 confirming obstruction, as well as gas in the gallbladder
confirming obstruction, as well as gas in the gallbladder  .
.
 and laminated filling defect
and laminated filling defect  at the transition point, which proved to represent an obstructing gallstone.
at the transition point, which proved to represent an obstructing gallstone.
 and the close proximity of the GB to the duodenum
and the close proximity of the GB to the duodenum  .
.
 .
.
 within the dilated small bowel. Note that the bowel distal to the gallstone is collapsed.
within the dilated small bowel. Note that the bowel distal to the gallstone is collapsed.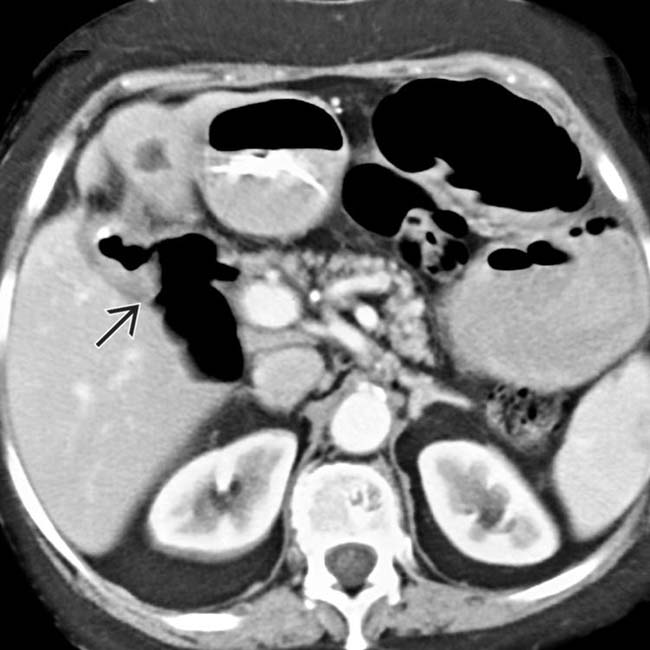
 to the duodenum.
to the duodenum.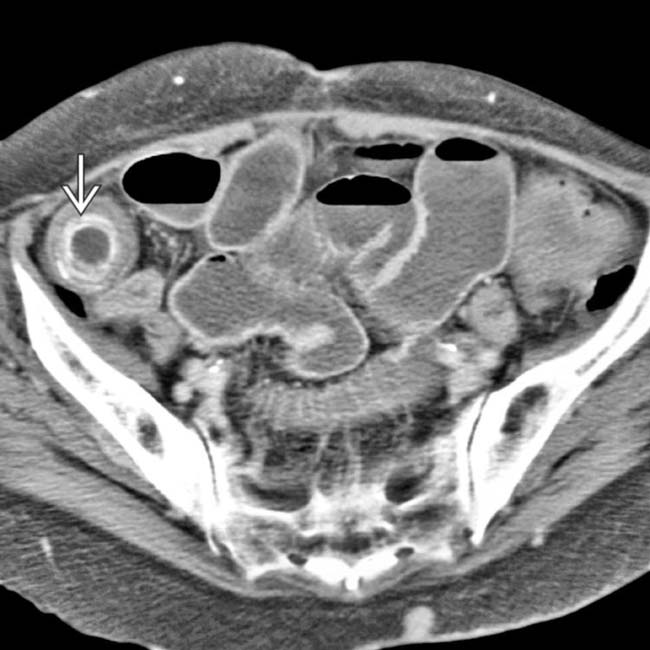
 “stuck” near the ileocecal valve.
“stuck” near the ileocecal valve.