Weight Gain
Weight gain is extremely common and the most frequent cause is simple obesity. Excessive weight gain itself has deleterious effects on general health. With the exception of simple obesity and pregnancy, other conditions account for less than 1% of patients presenting with weight gain.
Causes
Increased Fat
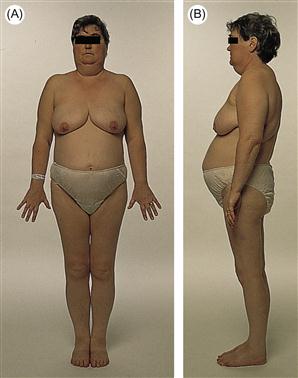
Figure 67 (A,B) Cushing’s syndrome.
Note the central rather than peripheral obesity. This patient also has typical facial features and a ‘buffalo hump’.
Increased Fluid
History
General
Enquire about the possibility of pregnancy and any changes in dietary habits that may result in simple weight gain. Rapid weight gain is often secondary to increased fluid, as opposed to an increase in dry weight. A drug history is taken to exclude the use of anabolic steroids and growth hormone, especially in body builders. Enquire about a family history, diet and amount of activity in relation to simple obesity.
Cushing’s syndrome
Patients with Cushing’s syndrome present with moon face, ‘buffalo hump’ (deposits of fat on the back of neck and shoulders), hair growth, acne, abdominal striae, muscle weakness, back pain, amenorrhoea, thin skin, bruising and depression. A drug history should be taken to exclude exogenous corticosteroids as the cause.
Hypothyroidism
With hypothyroidism, patients may complain of lethargy, anorexia, cold intolerance, goitre, dry hair, dry skin, constipation and menorrhagia.
Polycystic ovarian syndrome
Women with this condition present with hirsutism, obesity and menstrual irregularities. It is also associated with insulin resistance.
Hypothalamic disease
Prior history of neurosurgery, craniopharyngioma or other brain tumours may have resulted in damage to the hypothalamus. As it is the regulatory centre for appetite, uncontrolled excessive eating may result.
Cardiac failure
Fluid retention from cardiac failure may be accompanied by symptoms of exertional dyspnoea, orthopnoea, paroxysmal nocturnal dyspnoea. Ascites and peripheral oedema may also result from congestive heart failure.
Renal failure
Patients with renal failure may present with lethargy, fragile pigmented skin, peripheral oedema, periorbital oedema, thirst and polyuria.
Ascites
See p. 35.
Examination
Inspection
The distribution of body fat should be noted. Patients with Cushing’s syndrome have truncal obesity with proximal muscle wasting. Hirsutism is a feature of both polycystic ovarian syndrome and Cushing’s syndrome. With hypothyroidism, there may be loss of the outer third of the eyebrows and a ‘peaches and cream’ complexion.
Inspection of the trunk may reveal thin skin with easy bruising in both Cushing’s syndrome and renal failure. In addition, striae and thoracic kyphosis may be present with Cushing’s from wedge fractures caused by osteoporosis.
Proximal muscle weakness is found in both Cushing’s syndrome and hypothyroidism. Check for the physique of a ‘body builder’.
Palpation and auscultation
Peripheral oedema may be a feature of fluid overload with renal, hepatic and cardiac failure. Non-pitting oedema is characteristically found with hypothyroidism. The JVP should be examined and will be elevated with congestive cardiac failure and fluid overload with renal or hepatic failure. The pulse is taken and bradycardia may be noted with hypothyroidism. The blood pressure is measured and hypertension may be due to incorrect cuff size or may occur as a complication of Cushing’s disease. A third heart sound may be present with cardiac failure, and widespread pulmonary crepitation suggests pulmonary oedema from cardiac failure or fluid overload in renal or hepatic failure.
Further examination of the abdominal system may reveal the presence of ascites (p. 35), which may result from liver disease, malignancy or cardiac failure. A complete neurological examination is performed to screen for neurological deficits, which will warrant diagnostic imaging to look for lesions involving the hypothalamus. If there is any suspicion that a patient is taking body-building drugs, e.g. anabolic steroids, check for testicular atrophy and prostatic hypertrophy.
General Investigations
■ Urine dipstick
+++glucose – diabetes from Cushing’s syndrome or as a complication of obesity.+++protein is present with nephrotic syndrome. Blood may be present with renal disease.
■ U&Es
K+ ↓ Cushing’s. Urea and creatinine ↑ renal failure.
■ LFTs
Deranged with liver disease.
■ TFTs
Screen for hypothyroidism.
■ Random cortisol
↑ evening levels may suggest Cushing’s syndrome; a normal result does not exclude it. Although commonly performed, has little diagnostic value.
Specific Investigations
■ 24-hour urinary free cortisol
↑ with Cushing’s.
■ 24-hour urine collection for protein
>3.5 g with nephrotic syndrome.
■ Low-dose dexamethasone test
Failure of cortisol suppression with Cushing’s.
■ US abdomen and pelvis
Renal disorders, polycystic ovaries, ascites.
■ Echocardiography
Cardiac failure.
■ CT/MRI head
Hypothalamic disease.
■ Renal biopsy
To determine the aetiology of renal parenchymal disease.



