Chapter 18
Fractures in the older person
Karen Hertz1 and Julie Santy-Tomlinson2
1 University Hospital of North Staffordshire, Stoke-on-Trent, UK
2 University of Hull, Hull, UK
Introduction
As the world’s population ages, musculoskeletal trauma in the older person presents a growing challenge to healthcare systems. Although management of older people following trauma needs to follow the general considerations described in Chapter 17, there are also some differences and specific considerations which must be taken into account when caring for the older patient.
There are several different mechanisms of injury of trauma in older people including many of those to which younger patients are subjected. The most common cause of injury in older people, however, is a fall and it will be fall-related trauma which is the focus of this chapter. The care of older trauma patients requires highly skilled, specialised care whatever the cause. The practitioner also needs to be aware of the issues surrounding patients being admitted as a result of elder abuse and ensure that local policies for reporting are followed in order to protect vulnerable older people from further harm (see Chapter 1).
The global development of orthogeriatric models of care, particularly in the management of patients with a hip fracture, has become a key feature of improvements in care delivery over the last few decades. This chapter aims to provide an overview of evidence-based fracture management, care and rehabilitation for older people, focusing specifically on fragility fractures. The intention is to assist the practitioner in providing skilled, high quality, age-sensitive care. Such care must consider the specific needs of older people and minimise the complications of injury, hospitalisation and surgery whilst facilitating the restoration of functional ability.
Fragility fracture
Older people with fractures normally present as a result of a fragility fracture. It is estimated that there is one fragility fracture worldwide every three seconds, equating to 25 000 per day (International Osteoporosis Foundation 2012). Almost all result in attendance at an emergency department (ED), admission to hospital or a general practitioner visit. ‘Fragility’ fracture is defined as a fracture that results from ‘low energy’ trauma and is caused by mechanical forces that would not ordinarily result in a fracture. The World Health Organization (WHO) has noted that the injury results from a fall from a standing height or less affecting an older person with osteoporosis or osteopoenia (Kanis et al., 2001). Osteoporosis is a chronic disease that weakens bone strength and is characterised by low bone mass and structural deterioration of bone tissue, with a consequent increase in bone fragility leading to susceptibility to fracture (Chapter 13). The onset is often asymptomatic and may only be recognised after a person falls and sustains a fracture. The annual numbers of fragility fractures in most developed countries are very high and considered to be a major challenge for health services. According to the National Osteoporosis Society almost half of all women and one in six men will experience an osteoporotic fracture during their lifetime. It is expected that incidence will continue to increase as the population ages. Osteoporosis already affects one in three women and one in 12 men aged over 50, particularly post-menopausal women. The incidence in both sexes is known to rise rapidly with age due to increased bone loss after the menopause in women and age-related bone loss in both women and men. The prevalence of osteoporosis increases markedly with age: from 2% at 50 years to more than 25% at 80 years in women. As the longevity of the population increases, so will the incidence of osteoporosis and associated fragility fractures (NICE, 2012). Individuals may have a life expectancy of up to forty years after their first fragility fracture potentially resulting in a need for long-term management of the issues and associated risks.
Fragility fractures occur most commonly in the spine (vertebrae), hip (proximal femur) and wrist (distal radius) and less often in the arm (humerus), pelvis, ribs and other bones. They result in significant pain and severe disability, often leading to a reduced quality of life. Hip and vertebral fractures are also associated with decreased life expectancy. Every fragility fracture signals an increased risk of future fractures – at least doubling the risk of further fractures as well as risk of premature mortality. Figure 18.1 demonstrates how the progress of osteoporotic fractures occurs across the lifetime. At its worst, the individual’s experience of osteoporosis can be one of remorseless progression: from Colles’ fracture and minor (and perhaps minimally symptomatic) vertebral fractures to the major distress, dependency and disability of hip fracture.
Figure 18.1 Fracture morbidity. Adapted from BOA/BGS 2007 with permission
The usual care people receive after fragility fracture can be inadequate. There is frequently a failure to recognise osteoporosis as the cause of the fracture and to initiate long-term management of the condition. Problems with coordinating the key elements of care including: case-finding those at high risk; providing falls prevention; bone protection; fracture surgery and rehabilitation, can result in sub-optimal care and associated poor outcomes for patients. Recent thinking, however, acknowledges that ‘optimal care is cheaper than suboptimal care’ (DOH, 2009) on the basis that better care results in better outcomes as well as reduced complications and length of stay with a greater chance of return to independent living. Focusing on high quality, optimal care is, therefore, an essential aim of service/practice development.
Several studies have shown that a previous fracture at any site is associated with a doubling of risk of further fracture (McLellan et al., 2004, Kanis et al., 2004) highlighting the need to identify (or ‘case-find’) those who have sustained such a fracture in order to initiate early clinical assessment, investigation and treatment. For patients aged over 50 proactive case-finding in acute hospitals by fracture liaison services involves identification, by a specialist practitioner, of any patients presenting with a fragility fracture either through emergency care, fracture clinics or orthopaedic wards or by identification of vertebral fractures on X-rays performed for the specific purpose or other reasons. The following steps are recommended:
- investigate bone density
- commence drug treatment according to national guidelines/local policy (Chapter 13)
- referral to falls services
- monitor and support medication compliance.
As many as half of post-menopausal women who have had a prior fragility fracture, will go on to sustain a hip fracture. Targeting these at risk groups in primary care and through fracture liaison in acute services provides ready access to those at greatest risk of hip fractures and offers some chance of reducing the numbers of fractures in the future and treatment reduces the fracture risk by 50% (DoH 2009).
Caring for older patients following trauma
Looking after older people following trauma must follow the same principles for trauma management for all age groups as discussed in Chapter 16. It must be recognised, however, that the normal and abnormal changes that occur with ageing, relating to anatomy and physiology, and compounded by past medical history and active co-morbidities, mean that mortality increases in older people as a result of morbidity and that the normal physiological responses will be different to those of a younger adult. Specific considerations relating to ageing include:
- Airway – ageing can cause degeneration of the physiological airway and musculoskeletal pathology such as osteoarthritis. It can also reduce neck and spine flexibility, making airway management difficult.
- Breathing – loss of respiratory resilience, particularly with chronic obstructive pulmonary disease, means that patients can hypoventilate when supplemental oxygen is considered. They still need oxygen therapy, but require closer monitoring in recognition of this. Older people are also more at risk of respiratory failure because of the increased work of breathing.
- Circulation – reduction in cardiopulmonary reserve means that there is an increased risk of fluid overload when administering intravenous fluids (particularly colloids), requiring closer monitoring. Normal heart rate and blood pressure are not a guarantee of normal cardiac output and the use of beta blockers and anti-hypertensive agents can mask the signs of deterioration. In the event of cardiac arrest, beta blockers and antiplatelet medications will negatively influence outcome.
- Disability – prolonged inactivity and disuse often limits ultimate functional outcome and impacts on survival.
- Exposure – skin and connective tissue undergo extensive changes in the ageing process, resulting in diminished thermoregulation, increased risk of infection, poor wound healing and increased susceptibility to hypothermia.
It is important to consider older people following trauma as individuals and make sure that a full and comprehensive history is obtained that includes relevant co-morbidities and medication history along with an overview of previous functional ability and personal and social history. Assessment and subsequent care is best provided and managed by effective teams working to sound orthogeriatric principles. These include treating the fracture while considering the causes of the fall and any unstable co-morbidities as well as initiating effective rehabilitation while assessing and treating bone health with the aim of preventing further fractures. Over the last few years, hospital mortality has reduced in care settings where orthogeriatric input is available. In addition to the principles of fracture management described in Chapter 17, there are a number of specific considerations when managing fractures in older people. Osteoporosis, for example, not only makes fracture more likely, it also means that fractures are more likely to be comminuted – making anatomical reduction of the fracture problematic. The condition slows fracture healing and makes achieving sound internal fixation more difficult, meaning that fixation needs to be more robust and durable.
Hip fracture
Hip fracture is the plain English term for a proximal femoral fracture (or PFF). It refers to a fracture occurring in the area between the edge of the femoral head and 5 cm below the lesser trochanter (Figure 18.2). Such fractures are mostly fragility fractures occurring in older people. Half of all patients admitted with a hip fracture have had a previous fragility fracture – a ‘signal’ fracture that gives health care providers the opportunity to commence treatment to reduce the likelihood of hip fracture occurring. It is important to stress that identifying those patients at risk of this is central to decreasing the number of patients sustaining a hip fracture in the future.
Figure 18.2 Classification of hip fracture. From Parker and Johanssen 2006 with permission
Hip fracture is the commonest reason for admission to an orthopaedic unit, accounting for more than 20% of orthopaedic bed occupancy. In women over 45 years hip fractures can account for a higher proportion of hospital bed occupancy than other common conditions (DoH 2009), making the injury a major challenge as a common serious injury which is predominantly a phenomenon of later life. The average age of a person with a hip fracture is 83 years for men and 84 years for women. In the UK, for example, about 70–75 000 hip fractures occur annually and the total annual cost (including medical and social care) for all UK cases is estimated to be about £2 billion (NHFD, 2010). A similar picture is reported in many other developed nations such as Australia, Canada and Sweden (Kanis et al., 2012) although statistics suggest that rates are beginning to decline in some areas (Leslie et al., 2009, Pasco et al., 2011). The majority of expenditure is accounted for by hospital bed days and by health and social aftercare costs. It is predicted that by 2020 the number of people experiencing hip fracture in the UK will be in the region of 101 000 (BOA/BGS 2007).
For many previously fit patients, sustaining a hip fracture means loss of mobility and, for some of the frailer patients, the permanent loss of their ability to live at home. At present about a quarter of patients admitted to hospital following hip fracture come from institutional care and around 10–20% of those admitted from home ultimately move to institutional care.
It is widely documented that mortality at one year following hip fracture is approximately 30% (Parker and Anand 1991, SIGN 2009, BOA/BGS 2007). However, fewer than half of deaths are attributable to the fracture itself, reflecting the frailty of the patients and associated high prevalence of co-morbidities and complications. It is often the occurrence of a fall and consequent fracture that signals underlying ill health. Hence, hip fracture is by no means an exclusively surgical concern. Its effective management requires the coordinated application of nursing, medical, surgical, anaesthetic and multidisciplinary rehabilitation skills and a comprehensive approach covering the entire journey from emergency care to discharge. Increasingly the approach of an orthogeriatric model has been adopted in caring for patients following hip fracture – demonstrating significant improvements in care and patient outcomes along with reduced mortality.
Diagnosis
Patients with a hip fracture typically present to emergency services unable to walk and may exhibit shortening and external rotation of the affected limb. Frequently, but not exclusively, they give a history of trauma and have hip pain. In some instances patients may complain only of vague pain in their buttocks, knees, thighs, groin or back and their ability to walk may be unaffected. The majority of hip fractures are easily identified using plain X-rays, but an apparently normal X-ray does not necessarily exclude a fractured hip. Where there is doubt regarding the diagnosis (for example, a radiologically normal hip X-ray in a patient who remains symptomatic) and where the radiographs have been reviewed by a radiologist, alternative imaging should be performed. Magnetic resonance imaging (MRI) should be offered where hip fracture is suspected despite negative anteroposterior pelvis and lateral hip X-rays. If MRI is not available within 24 hours, or is contraindicated, computed tomography (CT) should be undertaken (NICE 2011).
Management
Surgical intervention is the treatment of choice for almost all patients following hip fracture. Exceptions are those in whom the fracture is already healing in a satisfactory alignment and those whose expected survival is, for reasons unrelated to hip fracture, very short. The NHFD report (2012) identified that less than 3% of patients did not have surgery. The timing of surgery has been shown to be important and this is discussed in Box 18.1.
Box 18.1 Evidence digest:
Hip fractures are divided into two main groups depending on their relationship to the capsule of the hip joint (Figures 18.2 and 18.3). Those within the joint capsule are termed intracapsular or femoral neck fractures. Those below the insertion are extracapsular. The extracapsular group is then further sub-classified into trochanteric and subtrochanteric fractures. There is a practical basis to the division into intracapsular and extracapsular fractures relating to both the blood supply of the femoral head and the mechanics of fixation (Figures 18.3 and 18.4a and b). It is, therefore, inaccurate to classify all hip fractures as fractures of the neck of the femur as this region is involved only in some fractures and the terminology should be used carefully to avoid confusion, since the classification has a significant impact on the treatment and care required. The recommended surgical procedure for the different fracture groups is as follows:
Figure 18.3 The blood supply to the head and neck of femur
Figure 18.4 a and b Examples of disruption of the blood supply to the head and neck of femur following fracture a) Minimal disruption of the blood supply following extracapsular fracture e.g. intertrochanteric fracture, and b) Significant disruption of the blood supply following intracapsular fracture e.g. subcapital fracture
Undisplaced intracapsular fractures
Surgical treatment is almost mandatory. Some impacted fractures may be difficult to diagnose but prognosis for impacted or undisplaced fractures is good following internal fixation conducted with a widely used method that is familiar to the surgeon such as cancellous bone screws (Mak et al., 2010).
Displaced intracapsular fractures
Surgical treatment is almost mandatory for displaced intracapsular fractures as they will not unite without fixation or replacement. Replacement arthroplasty is used in patients with a displaced intracapsular fracture (e.g. hemi-arthroplasty or total hip replacement) because of the risk of avascular necrosis of the femoral head as a result of disruption to local blood supply resulting from displacement of the fracture. The femoral head derives its blood supply from three sources (Figures 18.3 and 18.4): the nutrient artery and vessels from the joint capsule and the ligament teres. When the femoral head is displaced the blood supply from all but the ligament teres is disrupted and this may be severe enough to cause ischaemia, resulting in bone death (avascular necrosis) and subsequent collapse of the femoral head. This leads to destruction of the joint, causing ongoing pain and deformity. Hemi-arthroplasty (Figure 18.5) is commonly performed for displaced intra-capsular fractures. Compared to uncemented arthroplasty, cemented arthroplasty is said to improve hip function and is associated with lower residual pain post-operatively. Blood loss from an intracapsular fracture at the time of injury is minimal because of the poor vascular supply at the fracture site (AAGBI 2011).
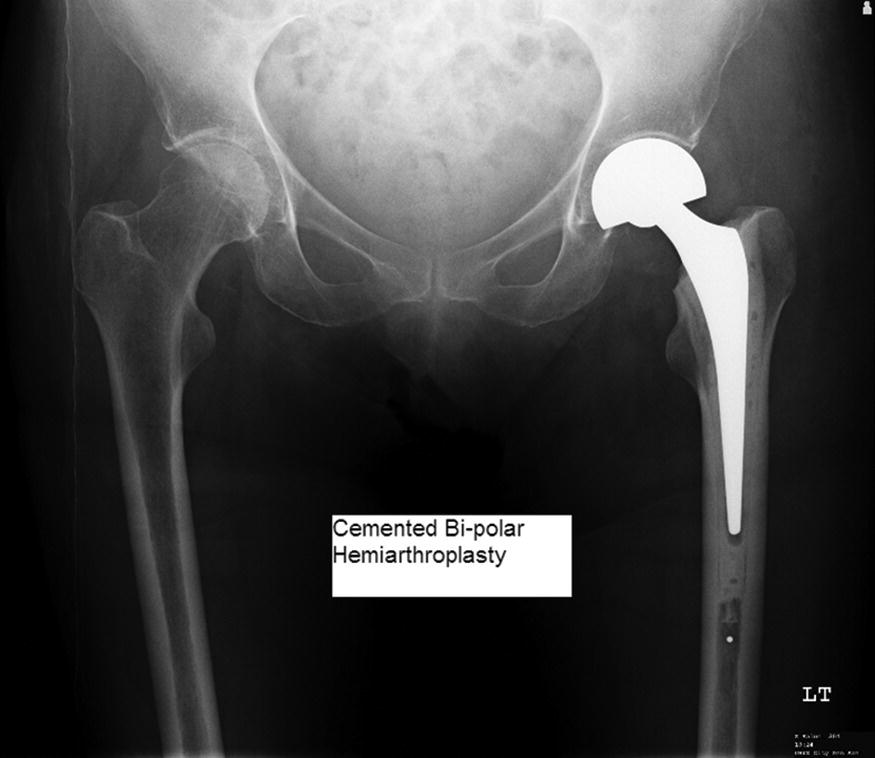
Figure 18.5 Hemiarthroplasty. Reproduced with permission from Mr Philip John Roberts
There is an increasing body of evidence to support total hip replacement (THR) over hemi-arthroplasty in selected patients (Figure 18.6). This is recommended by NICE (2011) who suggest that total hip replacements are offered to patients with a displaced intracapsular fracture who prior to the fracture:
- were able to walk independently and
- are not cognitively impaired and
- are medically fit for anaesthesia and the procedure.
THR is recommended for active patients or those with pre-existing joint disease, rather than hemi-arthroplasty because of acetabular wear and inferior functional outcome experienced with a hemi-arthroplasty. THR is, however, unsuitable for patients with dementia due to their reduced ability to follow postoperative movement restrictions and a consequently higher dislocation rate. Patients need to be able to understand and follow the post-operative guidance to prevent dislocation, but if able to do so will achieve higher functional outcomes and patients with underlying joint destruction will experience less pain.
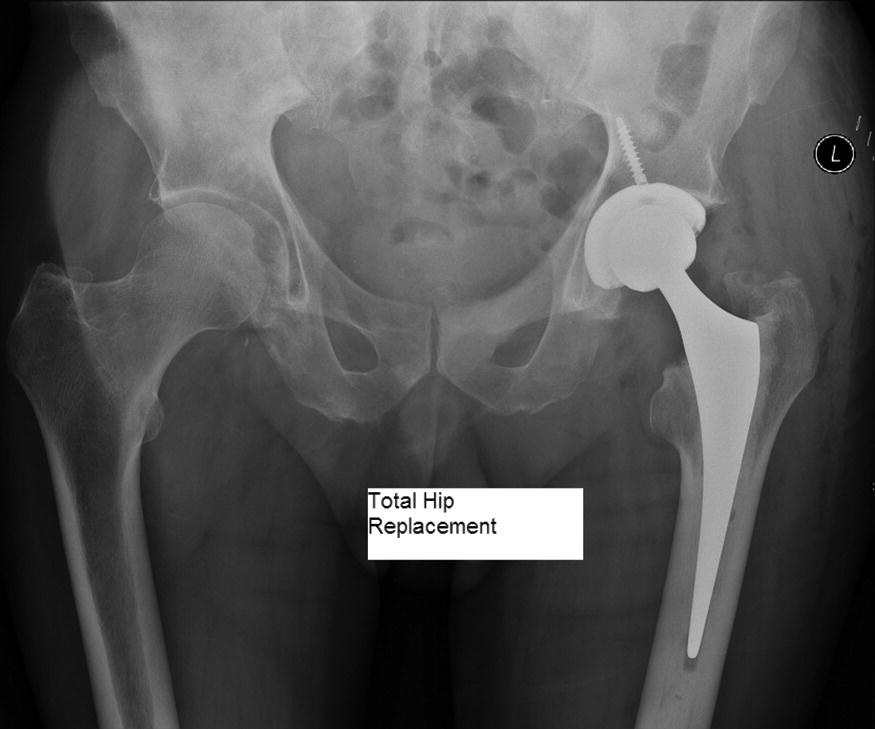
Figure 18.6 Total hip replacement. Reproduced with permission from Mr Philip John Roberts
Extracapsular fractures
Management of extra capsular fractures should reflect the differences in presentation and symptoms. Blood loss from an extracapsular fracture is much greater than that from an intracapsular fracture; loss from the cancellous bone at this site may exceed one litre. The greater the degree of comminution and the larger the size of the bone fragments, the greater the blood loss. In addition, greater periosteal disruption causes extracapsular fractures to be considerably more painful than intracapsular fractures. They can be treated conservatively, healing after six to eight weeks of traction and bed rest, but such management is associated with greatly increased morbidity and mortality and a considerably reduced chance of the patient regaining independence and/or returning home (AAGBI 2011). Undisplaced extracapsular fractures are often treated with cannulated screws (Figure 18.7). Surgical intervention for other fractures is recommended as follows.
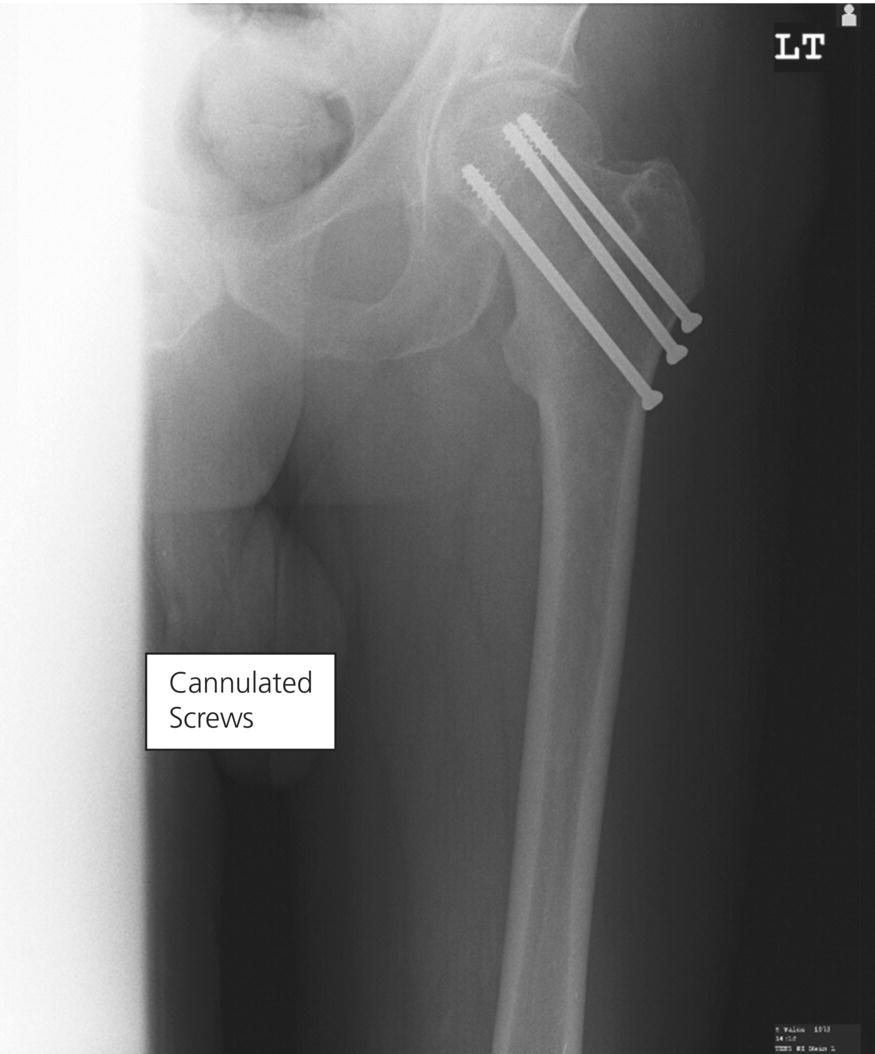
Figure 18.7 Cannulated screws. Reproduced with permission from Mr Philip John Roberts
Intertrochanteric fractures
Extra medullary implants such as a sliding hip screw are used in the fixation for patients with trochanteric fractures above and including the lesser trochanter (NICE 2011) (Figure 18.8). This stabilises the fracture, reduces pain and allows early mobility. The movement allowed by the implant in only one plane and axial loading of the fracture encourages bone healing.
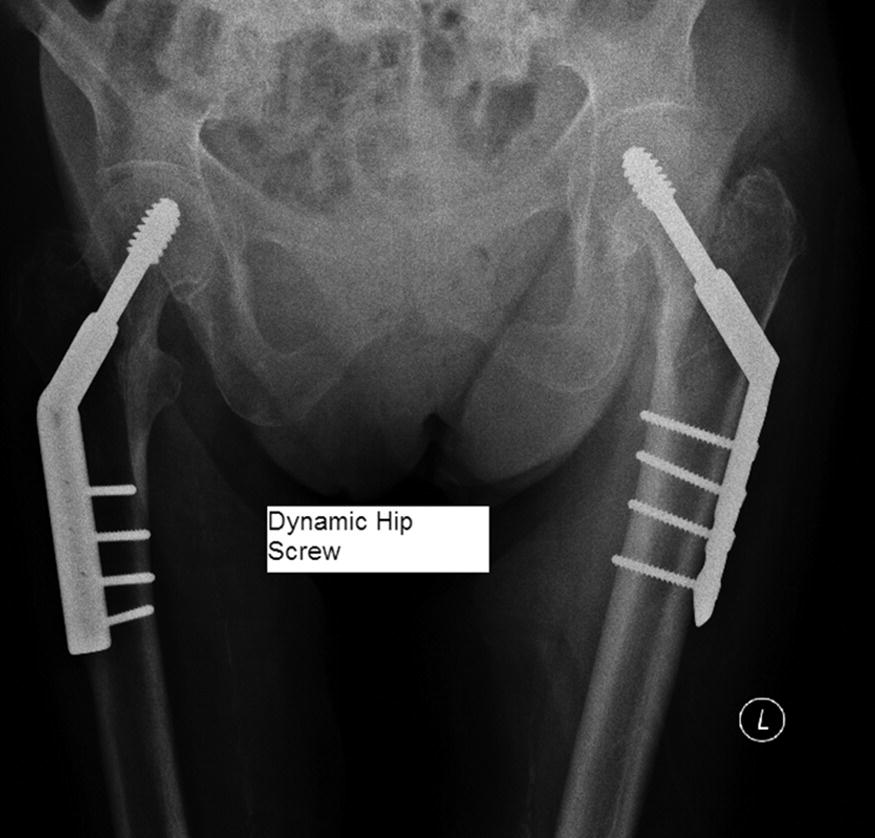
Figure 18.8 Dynamic hip screw. Reproduced with permission from Mr Philip John Roberts
Subtrochanteric fractures
These fractures are less common, accounting for about 5–10% of all hip fractures. They present a considerable challenge to the surgeon as the high mechanical forces in this region lead to an increased risk of fixation failure. NICE (2011) recommends the use of an intramedullary nail to treat patients with a subtrochanteric fracture such as the proximal femoral nail (Figure 18.9) which requires shorter duration of surgery and shorter hospital stay. It also results in fewer orthopaedic complications and there is less need for major re-operations than with other types of fixation (Mak et al., 2010).
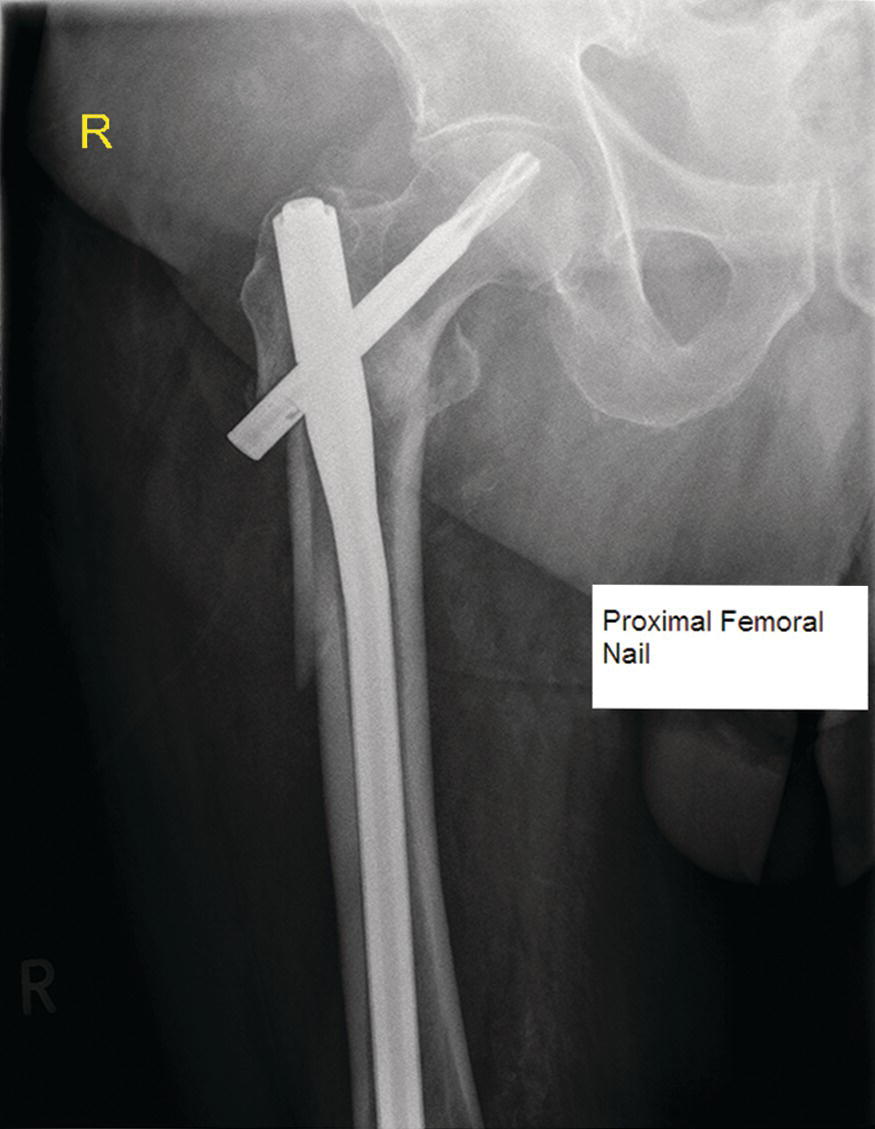
Figure 18.9 Proximal femoral nail. Reproduced with permission from Mr Philip John Roberts
Ethical considerations in treatment of patients with hip fracture
Approximately 25% of hip fracture patients have moderate or severe cognitive impairment and a further 15–25% have mild cognitive impairment. In order for the patient to consent to, or refuse, hip fracture surgery, they must be able to give consent voluntarily, based on a decision made following presentation and understanding of information about the procedure. The patient must be judged as having capacity to make that decision: they must be able to understand the information, remember it and use it to reach a decision. In this age group, the ability to assimilate information and communicate decisions may be impaired by poor vision, hearing or speech and steps should be taken to overcome these problems (AAGBI 2011). In some circumstances the operating team may be unable to satisfy themselves that the patient can give consent. If the patient does not have an advocate with a legal responsibility for decision making on their behalf an alternative approach needs to be found. Depending on national law and guidance and following close liaison with family or carers surgery may progress if two surgeons agree that it is in the patient’s best interests.
Nursing management of patients with a hip fracture
Older adults with hip fracture represent a growing number of the patients cared for by orthopaedic nurses around the world. This group are at increased risk of the more familiar peri-operative complications such as venous thromboembolism, pneumonia and urinary tract infections. Normal age-related changes, the stress of fracture, hospitalisation and chronic medical conditions also predispose them to other serious problems including inappropriately managed pain, malnutrition, dehydration, constipation, pressure ulcers, delirium, functional decline and death (Koval and Zuckerman, 1995; Mak et al., 2010). The majority of patients are admitted to an acute hospital where they are cared for by nurses who must also manage the care of patients with other traumatic injuries alongside the special care needs of the older adult. There are a number of guidelines related to best practice medical management strategies for this population but until recently there has been no guidance specific to the nursing care of older patients with hip fracture.
Care of the older adult is complex and best achieved by an interdisciplinary team approach. The concept of orthogeriatrics is well established in the medical and surgical care of this patient – care led by a collaborative orthopaedic and geriatric approach – but the concept has not yet become widely established in nursing care of this patient group. Even so, both skilled orthopaedic and elderly care nursing are vital in order to provide effective and appropriate care. Nurses are an integral contributor to the orthogeriatric team or, as described by NICE (2011) ‘the hip fracture programme’, as they are in an ideal position to co-ordinate care provision. The complex sharing of care between orthopaedic surgeons and orthogeriatricians could become fragmented and less effective if the care is not managed or coordinated effectively. The role of a specialist nurse or coordinator can vary according the size, culture and organisation of each individual unit, but such coordination is currently undertaken by a variety of nurses in different roles including; hip fracture nurse specialists, elderly care nurse specialists, trauma nurse coordinators and nurse practitioners. These advanced practitioners are well placed to ensure that the patient experience is positive, that they are appropriately prepared for surgery, placed early on a scheduled trauma surgery list, have a coordinated care and rehabilitation programme and are discharged to home or to an appropriate care setting.
Practitioners should be mindful of the complications that can occur in older patients and must monitor them closely at the same time as liaising with family and carers in order to promptly detect changes in patient condition. The most significant care issues relate to pain, malnutrition, dehydration, constipation, delirium, pressure ulcers and mobility/function. The quality of care being provided to the patient is reflected in these aspects of care and they are issues that respond to nursing management strategies, hence they can be referred to as nurse sensitive quality indicators. The following evidence-based principles of care following hip fracture have been identified in a set of international guidelines (Maher et al., 2012, Maher et al., 2013).
Pain
Hip fracture is painful and early fracture surgical fixation provides the most effective pain relief. Accurate pain assessment is the foundation for successful pain management because good pain control in the early stages of care will promote comfort and confidence. Later on, if pain is poorly controlled, mobilisation will be delayed – bringing with it the complications of prolonged bed rest and immobility leading to increased dependency and an associated rise in the risk of post-operative delirium.
A formalised analgesia protocol should be followed. Simple analgesics such as paracetamol should be prescribed and administered on a regular basis (unless contraindicated) and additional opioids or nerve blocks used in conjunction with the paracetamol to provide pain relief as required. NICE (2011) suggest that assessment of the patient is made immediately upon presentation at hospital and analgesia should be given routinely at that time. Within 30 minutes of administering initial analgesia, a further assessment of pain should be made, giving additional analgesia if required. Assessment and administration of analgesia should then occur hourly until the patient is settled and then regularly as part of routine care. The aim of analgesia should be to give sufficient pain relief to allow movements necessary for investigations, nursing care and rehabilitation.
Pain in older people is often under-reported by patients and undetected by practitioners. Cognitive impairment places patients at particularly high risk of this. Pain assessment scales alone do not provide the essential elements to guide treatment. It is extremely important to know the onset and duration, location, predisposing factors or influences and the type of pain. The acute pain of the fracture is often in conjunction with chronic pain which may be related to other co-morbid conditions such as osteoarthritis or malignancy. Visual analogue pain scores (VAPS), at rest and on movement, should be recorded before and after the administration of analgesia (RCP/BGS/Pain Society 2007). This form of self-reporting is the single most reliable measurement of pain. Verbal reports of pain are valid and reliable in patients with mild to moderate dementia or delirium. The diagnosis of pain in a patient with cognitive impairment due to dementia or delirium may be particularly difficult and requires familiarity with the patient and will require information from relatives or carers. Many studies have shown that cognitively impaired and acutely confused patients receive less analgesia than their unimpaired counterparts. This is generally because nursing and medical staff rely on self-reporting of pain and rarely consider pointers to the presence of pain such as moaning, sighing or holding a guarded posture, tachycardia and high blood pressure (BOA 2007). The use of a tool to tell staff about the individual needs of a person with dementia such as the ‘This is Me’ form available from the Alzheimer’s Society, encourages relatives and carers to document individual patient information and personal behaviours. Working with families of patients with dementia or delirium to complete this document will support pain assessment. See Chapter 11 for further consideration of general issues related to pain management.
Malnutrition
Malnutrition is often associated with ageing and is characterised by diminished hunger and thirst, along with chronic illness patterns. There are many causes of malnutrition including:
- Reduced intake – poor appetite due to illness, food aversion, nausea or pain when eating, depression, anxiety, side effects of medication or drug addiction.
- Inability to eat – due to being fasted for investigations or surgery, reduced levels of consciousness, confusion, difficulty in feeding oneself due to weakness, arthritis or other conditions such as Parkinson’s disease, dysphagia, vomiting, painful mouth conditions, poor oral hygiene or dentition and restrictions imposed by surgery or investigations.
- Lack of food availability – particularly prior to admission, due to poverty, poor quality diet at home, problems with shopping and cooking as well as issues with food availability in hospital or in care homes.
- Impaired absorption – due to medical and surgical problems affecting digestion; stomach, intestine, pancreas and liver/or absorption.
- Altered metabolism – increased or changed metabolic requirements related to illness or treatment e.g. cancer, surgery, organ dysfunction.
- Excess losses – vomiting, diarrhoea, nutrient fistulae, stomas, losses from nasogastric tube and other drains or skin exudates from wounds.
Up to 60% of hip fracture patients are clinically malnourished on admission to hospital. This can lead to serious consequences such as:
- increased risk of infections including surgical site infection and respiratory and urinary tract infection
- delayed wound healing and increased risk of pressure ulcer development
- impaired respiratory function
- muscle weakness and functional decline
- reduced cognitive function and depression.
Many older people do not eat and drink adequate amounts while in hospital, putting their health and recovery at risk and hospitalised hip fracture inpatients are thought to have only half their recommended daily energy, protein and other nutritional requirements (BOA 2007). Nutrition is an inter-disciplinary concern, which requires effective liaison and communication between all members of the team. A number of approaches to nutritional support have been studied. The strongest evidence for the effectiveness of nutritional supplementation exists for oral protein and energy feeds, multi-nutrient feeds (providing energy, protein, vitamins and minerals), which may reduce the risk of death or complication and possibly the length of stay (BOA 2007; Duncan et al., 2006). Patients’ acceptance of supplement drinks is often poor. It is therefore crucial that all staff dealing with patients recovering from hip fracture understand the importance of adequate nutritional intake and that specific attention is given to helping people to eat at meal times. Simple practical measures such as providing additional carers or volunteers to assist in nutrition can be effective, as well as other strategies such as meal times protected from disturbance and systems that highlight patients at risk of malnutrition such as coloured trays. Routine nursing care must include an assessment of nutritional intake and, where appropriate, referral for dietetic advice. General issues related to nutrition and the orthopaedic patient are considered in more detail in Chapter 10.
Dehydration
Dehydration is highly prevalent among older orthopaedic patients and carries with it significant potential adverse consequences. Older adults admitted to hospital from home or other care facilities often present with dehydration for a variety of reasons. This can include pre-existing restricted fluid intakes which may relate to normal age-related changes, diminished thirst reflex and subsequent diminished fluid intake. Many patients who suffer from incontinence or frequency may self-regulate fluid intake to reduce the risk of incontinence and because of difficulty accessing toilet facilities. Diuretic use can result in altered fluid balance. A long post-fall lie on the floor can also result in reduced fluid intake.
Dehydration decreases circulatory volume, resulting in diminished perfusion to organs and tissues and is implicated in the development of delirium, acute kidney injury, pressure ulcers, falls, venous thromboembolism and urinary tract infections. Optimised perioperative fluid management helps to reduce the incidence of dehydration and therefore reduces morbidity and hospital stay (Price et al., 2004). Every effort must be made to ensure that intravenous fluid is prescribed on admission and that it is administered over the correct time. Strict fluid balance monitoring along with shortest possible periods of pre-operative fasting also prevent or improve dehydration.
Electrolyte imbalances, particularly hyponatraemia and hypokalaemia, are common in the post-operative period and reflect limited renal reserve. The situation may be made worse by diuretics and inappropriate maintenance of intravenous fluids. This limited renal reserve is also reflected in the high risk of acute kidney injury (AKI) in hip fracture patients, which is estimated to be 16% (Bennet, 2010). Older patients admitted to hospital for emergency surgery are at increased risk of acute kidney injury and its associated pre- and post-operative complications. This can be because of pre-existing co-morbid conditions, age and complex polypharmacy, which often includes diuretics and nephrotoxic medication such as angiotensin-converting enzyme inhibitors (ACE inhibitors) used in the management of hypertension and heart failure and non-steroidal anti-inflammatory drugs (NSAIDs) used for pain relief. Baseline renal function is a good predictor for AKI, but establishment of this may be difficult in hip fracture patients as they may be acutely dehydrated on admission with or without the presence of some chronic renal dysfunction. Close monitoring of fluid balance and blood biochemistry is essential to prevent or identify renal injury.
Constipation
Constipation is a significant risk for patients following hip fracture and prevention should be considered early in the care pathway. Use of opioid analgesics including codeine (even in low doses), dehydration, altered diet (particularly decreased fibre in the diet) and lack of mobility can all increase this risk (SIGN 2009). This is considered in more detail in Chapter 9.
Delirium
Delirium (sometimes called ‘acute confusional state’) is a clinical syndrome characterised by disturbed consciousness and altered cognitive function or perception. It has an acute onset and a fluctuating course (NICE 2010). It is a common, but serious and complex clinical syndrome associated with poor outcomes. As many as 65% of patients who have sustained a hip fracture may develop delirium. It is commonly categorised as being hypoactive or hyperactive, reflecting the nature of the behaviour seen in patients.
Delirium is independently associated with a variety of adverse outcomes including pressure ulcers, functional decline, longer hospital stay and institutionalisation. Prompt detection coupled with ongoing assessment and targeted nursing interventions have been proven to reduce the incidence and severity of symptoms of those suffering from delirium (NICE, 2010; Mak et al., 2008). Assessment and the establishment of baseline cognition is a critical and often challenging first step in delirium detection and close communication between the nursing team and family or carers is essential. In addition to information from family members, undertaking an initial Abbreviated Mental Test Score is essential. Although this is not an assessment tool for delirium, it will provide baseline information relating to cognitive function. If there is any suspicion of delirium, tools such as the Short Confusion Assessment Method (shortCAM) are recommended by NICE (2010) for more comprehensive assessment, although training is required in order to undertake the assessment as it is often difficult to distinguish between delirium and dementia.
It is suggested that prevention of delirium is possible in up to 30% of cases (Inouye et al., 1999, Marcantonio et al., 2001). Early attention to risk factors, particularly in patients with underlying dementia, should be addressed early and good communication with patients, family and carers can help practitioners to recognise subtle changes. If delirium is evident it is important to identify and manage any possible underlying cause or combination of causes (BGS 2005) by:
- Seeking early comprehensive orthogeriatric review.
- Withdrawing or reducing culprit drugs such as opiates, where appropriate.
- Effective management of pain.
- Monitoring and screening for infection, while using universal precautions to prevent infection.
- Avoid use of devices that increase the risk of infection such as urinary catheters.
- Alcohol withdrawal increases the likelihood of patients developing delirium so management of withdrawal is key to avoiding delirium. Use of a protocol to manage chemical dependency withdrawal such as the Clinical Institute Withdrawal Assessment (CIWA) score can help ensure symptoms of withdrawal are identified and addressed early.
- Provide effective reassuring communication and reorientation (for example explaining where the person is, who you are and what your role is).
- Invite/encourage family, friends and carers to participate in care.
- If a person with delirium is distressed or considered a risk to themselves or others and verbal and non-verbal de-escalation techniques are ineffective or inappropriate, consider medication and other methods to maintain safety such as low beds and higher levels of supervision.
Pressure ulcers
Development of pressure ulcers is a frequent complication of hip fracture and surgery and up to one third of patients will develop a pressure ulcer (BOA 2007). Patients with pressure ulcers following hip fractures require significantly more nursing care, longer hospital stay, increased hospital costs and use more health care resources following discharge compared to patients without pressure ulcers (Chaves et al., 2010). Given the very high risk, prevention and management of pressure ulcers in this group of patients is, therefore, central to effective, high quality care. Chapter 12 provides detailed evidence-based advice for both prevention and management of pressure ulcers which is equally applicable to a patient with a hip fracture.
Rehabilitation of the older person following fractures
Although a section of this book (Chapter 6) has considered rehabilitation for patients as a result of orthopaedic conditions, orthopaedic surgery or injury, it is important to consider rehabilitation specifically for patients following all types of fragility fracture, but particularly those following hip fracture. This group of patients is older and more likely to have co-morbid conditions which will adversely affect rehabilitation abilities and outcomes if not managed appropriately. The evidence available in the literature mainly considers rehabilitation following hip fracture, but these programmes can easily be transferred to any type of fragility fracture.
Currently orthopaedic rehabilitation models are fragmented and have not been well evaluated in terms of functional outcome when compared to length of hospital stay. There are, however, three main pathways for patients following hip fracture which are described by NICE (2011):
- The traditional pathway of care is that a patient with hip fracture is admitted to a trauma ward where the orthopaedic surgical team lead both surgical care and subsequent rehabilitation. Geriatrician input to such wards is limited with referrals and medical queries being dealt with on a consultative basis by the on-call medical registrar or on occasional geriatrician visits, but without a proactive geriatrician lead to the multidisciplinary team.
- A more collaborative model of care through formal ‘orthogeriatric’ care, with older trauma patients admitted to a trauma ward or specialised unit under the joint care of both geriatricians and orthopaedic surgeons.
- Hip fracture programmes (HFP), with the orthogeriatric medical team contributing to joint preoperative patient assessment and increasingly taking the lead for post-operative medical care, multidisciplinary rehabilitation (MDR) and discharge planning, with ongoing governance for rehabilitation in hospital or as part of a community rehabilitation scheme as described below.
After initial surgical care and mobilisation in the first two models of care, early post-operative transfer to an orthogeriatric rehabilitation unit or mixed rehabilitation unit for ongoing treatment is another option. This may be additionally supported by community rehabilitation as early supported discharge (ESD) or intermediate care at home. Patients are discharged home from the acute trauma ward or, in some cases, a rehabilitation ward within the hospital supported with a 4–6 week rehabilitation package. This service may include patients living in care homes, but may be limited to patients returning to live independently in their own homes.
The evidence strongly supports the orthogeriatric approach to hip fracture management, and NICE (2011) recommend the development of hip fracture programmes. In this model management and care is undertaken by collaborative working between orthopaedic surgeons, orthogeriatricians, nurses and allied health professionals who have expertise in the care of older patients in surgical environments and associated specific needs. This represents a considerable change in the organisation of medical and surgical management of hip fracture patients. It requires a change in philosophy that needs to be embedded into trauma care as a whole and reflected in pre- and post-qualifying nurse education programmes for health professionals.
The ethos of effective hip fracture programmes is that the care should be provided by professionals interested in high quality care and achievement of best functional outcomes for this group of patients, wherever rehabilitation occurs. This includes discharge from the hip fracture programme when optimal physical, medical and functional ability have been achieved and means that patients are not discharged prematurely without achieving their potential. Programmes must be based on the premise that cost and quality are not in conflict. A review of the available literature and a cost-based analysis of such a programme confirmed that looking after hip fracture patients well (in terms of preventing complications, achieving better functional outcomes, preventing further falls, preventing readmission) was cheaper than looking after them badly (BOA 2007). NICE (2011) clearly outline how such a programme may encompass all types of rehabilitation settings (e.g. acute hospital rehabilitation, geriatric orthopaedic unit rehabilitation or ESD programmes) as long as patients are selected appropriately for ESD and the hip fracture programme team retain governance for care. This approach needs to ensure the minimum number of transfers between care settings to ensure that consistency and continuity are maintained. Transfers between care settings not only lengthen stay, but also reduce the likelihood of final discharge home.
Nurses working in acute hospital trauma wards are central to the care of patients following hip fracture. They need to embrace the principles of excellent trauma nursing practice, but need to provide this in a manner that is focused clearly on the specific needs of older people. This involves consideration of the surgical post-operative complications of pain, dislocation and wound infection and the complications specific to older people such as delirium, dementia, malnutrition and pressure ulcer development. This must include working with patients, carers, therapists, community health or social care teams to promote safe and appropriate discharge home or to the care setting that best meets the patient’s needs.
Consideration of palliative care for patients following hip fracture
Studies have shown that an estimated 18 to 28% of older hip fracture patients die within one year of fracture. Of those who survive, it is estimated that between 24 and 75% will not return to their pre-fracture level of independence (Koval et al., 1994, Mak et al., 2010). Although palliative care originally focused on patients with cancer, it is now well documented that consideration for a palliative care approach should be made for people at the end of their lives for non-malignant as well as malignant disease. Palliative care is defined by the World Health Organization (2011) as:
…an approach that improves the quality of life of patients and their families facing the problem associated with life threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual. Palliative care affirms life and regards dying as a normal process, and intends neither to hasten nor to prolong death. Using a team approach palliative care addresses the needs of patients and their families, including bereavement counselling if necessary.
This philosophy of care allows for physical, psychological, social and emotional care for patients, their families and carers when the patient with a hip fracture is frail and does not have the physical resilience to survive the trauma of the fracture. Effective models of care for patients with hip fracture actively lend themselves to the inclusion of patient-centred palliative care when appropriate. Typically, palliative care is provided by an interdisciplinary team who focus on the assessment and treatment of pain and other symptoms while ensuring that care is enhanced by patient-centred communication and decision-making across the continuum of care settings, from hospital to home.
Identifying patients for whom a palliative care approach is most appropriate is difficult. Many patients presenting with hip fracture also have multiple co-morbidities; in the 2011/12 NHFD report 67% of patients were graded at American Society of Anaesthesiologists (ASA) GRADE III or above (Chapter 14), identifying those who have severe systematic disease that limits activity or is life threatening. It could be suggested that these are the people for whom palliative care should be considered. However, many such patients recover well post-operatively, leave hospital and have a good functional outcome and ongoing quality of life. Appropriate models of end of life care are currently a matter of considerable discussion. Palliative care has not previously been a natural consideration in orthopaedic care so this is a matter for continuing debate and discussion rather than something that is currently integrated into practice.
It is the responsibility of the orthogeriatric or hip fracture team, through good communication with patients’ families and carers, to identify those people who have been having the typical period of decline pre-fracture and for whom the physical insult of fall, fracture, surgery and hospitalisation leads to the hastening of end of life. It then becomes the responsibility of the team to prepare the patient and family not only physically, financially and emotionally, but also to ensure that ongoing care and treatment is appropriate to the patient’s needs and this may or may not include surgical intervention. If a hip fracture complicates or precipitates a terminal illness, surgery should be considered as part of a palliative care approach in order to minimise pain and other symptoms, not necessarily to regain functional ability (NICE 2011). Surgery provides significant pain relief that will then not only allow nursing interventions to be undertaken more comfortably, but will facilitate transfer from an acute orthopaedic unit to either home or to another care setting in keeping with the patients and/or carers end of life wishes.
Hip fracture audit
Older people who sustain a hip fracture deserve to receive the best healthcare possible every time they present to a hospital, but there often remains a disparity in care that patients receive globally, nationally and locally. This is demonstrated year on year in hip fracture audit reports. Hip fracture care over the last few years has received considerable attention following national initiatives such as the National Hip Fracture Database (NHFD) in the UK. This audits the BOA/BGS (2007) six standards of care, the Royal College of Physicians’ Audit of Falls and Bone Health, the Department of Health’s Commissioning Toolkit and the development of NICE Clinical Guideline 124 on the management of hip fracture. Hip fracture audit was first undertaken in Sweden and similar ventures are in place in many other countries such as Australia, New Zealand, Canada and Ireland. In the UK, those units which provide evidence of high quality care (through NHFD audit) receive additional financial rewards. This provides an unprecedented opportunity for units to improve care and patient services.
Conclusion
The care of patients following hip fracture presents a major challenge for trauma, rehabilitation and community services and particularly to nurses. Increasing evidence for best practice is leading to improvements in care that are demonstrable through audit. The way in which services are organised will continue to have an impact on the outcomes of care and there remains a need for staff to be motivated to care for this vulnerable group of patients and to receive education that ensures they have the right knowledge and skills to do so.
Recommended further reading
- British Orthopaedic Association/British Geriatric Society (BOA/BGS) (2007) Care of Patients with Fragility Fractures. London: BOA. Available at: http://www.bgs.org.uk/pdf_cms/pubs/Blue%20Book%20on%20fragility%20fracture%20care.pdf (accessed 19 November 13).
- Maher, A.B., Meehan, A.J., Hertz, K. et al. (2012) Acute nursing care of the older adult with fragility hip fracture: An international perspective. Part 1. International Journal of Orthopaedic and Trauma Nursing, 16(4), 177–194.
- Maher, A.B., Meehan, A.J., Hertz, K. et al. (2013) Acute nursing care of the older adult with fragility hip fracture: An international perspective. Part 2. International Journal of Orthopaedic and Trauma Nursing, 17(1), 4–18.
- NICE (2011) Hip Fracture: The Management of Hip Fracture in Adults. NICE Clinical Guideline 124. NICE, London.
- NICE (2012) Osteoporosis: Assessing the Risk of Fragility Fracture. NICE Short Guideline. NICE, London.
- Parker, M. and Johansen, A. (2006) Hip fracture. British Medical Journal, 333(7557), 27–30.
References
- Association of Anaesthetists of Great Britain and Ireland (AAGBI) (2011) Management of Proximal Femoral Fractures. Available at:http://www.aagbi.org/sites/default/files/femoral%20fractures%202012_0.pdf (accessed 19 November 2013).
- Bennet, S.J. (2010) Acute renal injury following hip fracture. Injury, 41(4), 335–338.
- Bottle, A. and Aylin, P. (2006) Mortality associated with delay in operation after hip fracture: observational study. British Medical Journal, 332, 947–950.
- British Geriatric Society (2005) Guidelines for the Prevention, Diagnosis and Management of Delirium in Older People in Hospital. Available at: http://www.bgs.org.uk/index.php/clinicalguides/170-clinguidedeliriumtreatment?showall=andlimitstart (accessed 19 November 2013).
- British Orthopaedic Association (BOA) (2007) Standards for Trauma (BOAST). BOAST 1: Hip Fracture in the Older Person. BOA, London. Available at: http://www.boa.ac.uk/LIB/LIBPUB/Documents/BOAST%201%20-%20Hip%20Fracture%20in%20the%20Older%20Person%20Version%201%20-%202008.pdf (accessed 19 November 2013).
- British Orthopaedic Association/British Geriatric Society (BOA/BGS) (2007) Care of Patients with Fragility Fractures. BOA, London. Available at: http://www.bgs.org.uk/pdf_cms/pubs/Blue%20Book%20on%20fragility%20fracture%20care.pdf (accessed 19 November 2013).
- Chaves, L.M. Grypdonck, M. and DeFloor, T. (2010) Protocols for pressure ulcer prevention: are they evidence-based? Journal of Advanced Nursing, 66(3), 562–572.
- Department of Health (2009) Fracture Prevention Services: Economic Evaluation. DOH, London. Available at:http://www.cawt.com/Site/11/Documents/Publications/Population%20Health/Economics%20of%20Health%20Improvement/fractures.pdf (accessed 19 November 2013).
- Duncan, D.G., Beck, S.J., Hood, K. and Johansen, A. (2006) Using dietetic assistants to improve the outcome of hip fracture: a randomised controlled trial of nutritional support in an acute trauma ward. Age and Aging, 35(2), 148–153.
- International Osteoporosis Foundation (2012) Capture the Fracture Report. Available at: http://www.iofbonehealth.org/capture-fracture-report-2012 (accessed 19 November 2013).
- Inouye, S.K., Bogardus, S.T., Charpentier, P.A. et al. (1999) A multicomponent intervention to prevent delirium in hospitalized older people. New England Journal of Medicine, 340(9), 669–676.
- Kanis, J.A., Oden, A., Johnell, O. et al. (2001). The burden of osteoporotic fractures: a method for setting intervention thresholds. Osteoporosis International, 12(5), 417–427.
- Kanis, J.A., Johnell, O., De Laet, C. et al. (2004) A meta-analysis of previous fracture and subsequent fracture risk. Bone 35(2): 375–382.
- Khan, S.K., Kalra, S., Khanna, A., Thiruvengada, M.M. and Parker, M.J. (2009) Timing of surgery for hip fractures: A systematic review of 52 published studies involving 291,413 patients. Injury, 40, 692–697.
- Kanis, J.A., Oden, A., McCloskey, E.V. et al. (2012) A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporosis International, 23(9), 2239–2256.
- Koval, K.J. and Zuckerman J.D. (1994) Hip fractures: overview and evaluation and treatment of femoral neck fractures. Journal of the American Academy of Orthopaedic Surgeons, 2(3), 141–149.
- Leslie, W.D., O’Donnell, S., Jean, S. et al. (2009) Trends in hip fractures in Canada. Journal of the American Medical Association, 302(8), 883–889.
- Maher, A.B., Meehan, A.J., Hertz, K. et al. (2012) Acute nursing care of the older adult with fragility hip fracture: An international perspective. Part 1. International Journal of Orthopaedic and Trauma Nursing, 16(4), 177–194.
- Maher, A.B., Meehan, A.J., Hertz, K. et al. (2013) Acute nursing care of the older adult with fragility hip fracture: An international perspective. Part 2. International Journal of Orthopaedic and Trauma Nursing, 17(1), 4–18.
- Mak, J., Cameron, I. and March, L. (2010) Evidence-based guidelines for the management of hip fractures in older persons: An update. Medical Journal of Australia, 192(1), 37–41.
- Marcantonio, E., Flacker J., Wright, J. and Resnick, N., (2001) Reducing delirium after hip fracture: A randomized trial. Journal of the American Geriatrics Society, 49: 516–522.
- McLellan, A., Reid, D. and Forbes, K. (2004) Effectiveness of Strategies for the Secondary Prevention of Osteoporotic Fractures in Scotland. CEPS 99/03. NHS Quality Improvement Scotland, Edinburgh.
- National Hip Fracture Database (NHFD) (2010) The National Hip Fracture Database National Report 2010. Available at: http://www.rcseng.ac.uk/news/docs/NHFD%20%28final%29.pdf (accessed 21 November 2013).
- National Hip Fracture Database (NHFD) (2012) The National Hip Fracture Database National Report 2012. Available at: http://www.nhfd.co.uk/003/hipfractureR.nsf/0/da44e3a946a14e4180257a6f001eb4db/$FILE/NHFD%20National%20Report%202012%20Summary.pdf (accessed 21 November 2013).
- National Osteoporosis Society http://www.nos.org.uk (accessed 4 April 2014).
- National Institute for Health and Clinical Excellence (NICE) (2010) Understanding NICE Guidance: Delirium (103). NICE, London.
- NICE (2011) Hip Fracture: The Management of Hip Fracture in Adults. NICE Clinical Guideline 124. NICE, London.
- NICE (2012) Osteoporosis: Assessing the Risk of Fragility Fracture. NICE Short Guideline. NICE, London.
- Parker, M. and Anand, J. (1991) What is the true mortality of hip fractures? Public Health, 105(6), 443–446.
- Parker, M. and Johansen, A. (2006) Hip fracture. British Medical Journal, 333(7557), 27–30.
- Pasco, J.A., Brennan, S.L., Henry, M.J. et al. (2011) Changes in hip fracture rates in south-eastern Australia spanning the period 1994–2007. Journal of Bone Mineral Research, 26(7), 1648–1654.
- Price, J.D., Sear, J.J.W. and Venn, R.R.M. (2004) Perioperative fluid volume optimization following proximal femoral fracture. Cochrane Database of Systematic Reviews 1 (Art. No.: CD003004). DOI:10.1002/14651858.CD003004.pub2.
- Royal College of Physicians, British Geriatrics Society and the British Pain Society (2007) The Assessment of Pain in Older People. RCP/BGS/BPS, London. Available at: http://www.bgs.org.uk/Publications/pubdownlds/Sep2007PainAssessment.pdf (accessed 20 November 2013).
- Scottish Intercollegiate Guidelines Network (SIGN) (2009) Management of Hip Fracture in Older People. National Clinical Guideline 111. Available at: http://www.sign.ac.uk/pdf/sign111.pdf (accessed 21 November 2013).
- Shiga T., Wajima Z. and Ohe Y. (2008) Is operative delay associated with increased mortality of hip fracture patients? Systematic review, meta-analysis and meta-regression. Canadian Journal of Anaesthesia, 55(3),146–154.
- World Health Organization (2011) Palliative Care for Older People: Better Practice. WHO, Geneva. Available at: http://www.euro.who.int/__data/assets/pdf_file/0017/143153/e95052.pdf (accessed 22 April 2014).
Related posts:
 Professional development, competence and education
The complications of musculoskeletal conditions and trauma
Professional development, competence and education
The complications of musculoskeletal conditions and trauma
 The team approach and nursing roles in orthopaedic and musculoskeletal trauma care
The team approach and nursing roles in orthopaedic and musculoskeletal trauma care
 Soft tissue, peripheral nerveand brachial plexus injury
Soft tissue, peripheral nerveand brachial plexus injury
 Key musculoskeletal interventions
Key musculoskeletal interventions
