[level-membership-for-orthopaedics-category]3
Flexibility and Stretching
1. Describe viscoelasticity and the properties associated with collagen.
2. Explain the stress-strain curve and factors that influence change.
3. Discuss Golgi tendon organs (GTOs) and muscle spindles.
4. Discuss how temperature affects connective tissue.
5. Define and discuss range of motion, flexibility, and stretching.
6. Outline various methods used to measure flexibility.
7. Identify and describe various stretching techniques.
8. Discuss precautions and essential components of stretching program development.
9. Discuss at least two proposed benefits of stretching.
10. Explain how stretching might negatively impact activity performance.
11. Describe the clinical applications for stretching soft-tissue contractures.
12. Describe and contrast the differences and similarities between scar tissue and adhesions.
Enhancing flexibility is an important component of a fitness program7 and is useful, not only for sport-specific activities, but also for activities of daily living (ADLs). The need for flexibility is particularly necessary if mobility has been impaired, resulting in compromised range of motion (ROM). ROM is the amount of movement available to a joint moving within its anatomic range. Muscular imbalances due to shortened muscles may lead to faulty postural alignment that may lead to injury and joint dysfunction. The ability to restore ROM is crucial when implementing or following a rehabilitation program; consequently, being able to incorporate stretching exercises to restore flexibility as well as normal ROM and function becomes a primary goal for the physical therapist assistant (PTA).
Many clinicians emphasize that having a more flexible body is more efficient, improves muscle balance, and more easily undergoes strength and endurance training. Overall purported benefits of flexibility due to stretching include injury prevention, quicker recovery from workouts, a reduction in post exercise soreness, and facilitation of relaxation.2,129 However, the effects of stretching on performance is somewhat more controversial. Some literature shows that it may potentially help improve performance,48 whereas other literature and research reveal potential detrimental effects on maximal performance activities after stretching.66,113,124,131 Research into flexibility and stretching is ongoing in an attempt to determine the effects of stretching on the body. Consequently, some of the long-held beliefs about stretching, especially regarding performance, are being challenged.
PROPERTIES OF CONNECTIVE TISSUE
Just as amino acids are the building blocks of protein, tropocollagen is the building block of collagen (Fig. 3-1). Collagen fibers are made of short subunits (fibrils) and are found in varying amounts within the different connective tissues: bone, tendon, muscle, skin, hyaline cartilage, and joint capsule.20,41,119 Collagen is a protein building block of connective tissue and it provides the strength needed to withstand high levels of tension and force during movement and exercise. There are more than 20 types of collagen, but the majority of the collagen in the body consists of types I, II, and III.38 Of these, type I collagen is the most abundant in the body.
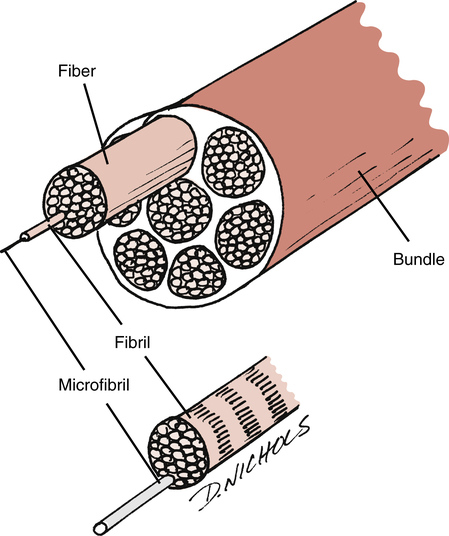
Type I collagen fibers are thick fibers gathered into bundles and display very little elongation when placed under tension (they have an ability to resist pulling). Type II collagen fibers, on the other hand, are thinner and possess slightly less tensile strength. These fibers are observed primarily in tissues such as articular cartilage and the nucleus pulposus. Type III collagen serves mainly in a structural support capacity and is found in expansible organs (e.g., arteries, liver, lungs).58 It is also common in fast growing or healing tissue and is often seen at the early stages (phase 1) of wound repair. It is later replaced by the tougher type I collagen.90
Elastin is a structural protein present in tendons in amounts of less than 1%.35,136 Tissues with greater amounts of elastin usually demonstrate greater degrees of flexibility. Elastin assists collagen in the recovery of tissues after stress.
Stress and Strain
Stress or load is given in units of force/area, where the units may be pounds per square inch or Newtons per square centimeter.96 Therefore stress is directly related to the magnitude of force and inversely related to the unit area, but is independent of the amount of a material.97 The complementary measure related to stress is strain or deformation. Strain is usually dimensionless, since the units of measure cancel each other out, but units are often provided (e.g., inches/inch) to give a perspective of scale applied to the loads.96
The relation of stress and strain is dependent on several factors. These include the material properties used, the magnitude of the stresses, and the rate of stress application. Subsequently, the graphical representation of stress and strain is different for each type of material discussed. This representation is known as the stress-strain or load-deformation curve.92 Figure 3-2 demonstrates the various regions within the stress-strain curve, with each region demonstrating a biomechanical property of a tissue.
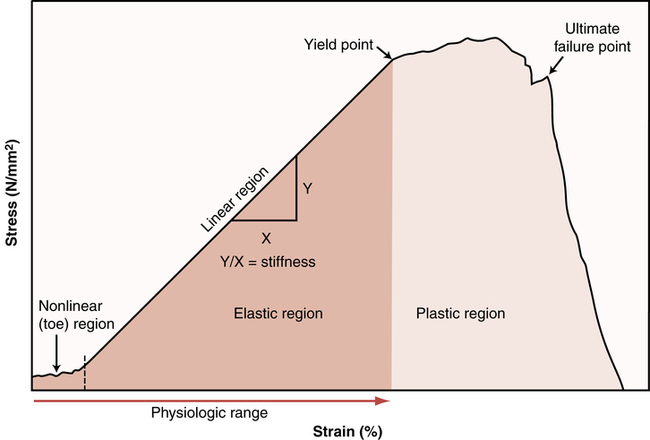
The toe region represents how a slightly pulled tissue (i.e., a ligament) produces only a small amount of tension within the tissue; it indicates that the collagen fibers within the tissue must first be pulled tight before a stretch can be induced. This minimal amount of tension simply results in the slack of the tissue being taken up with no stretch being encountered. The elastic region represents a linear change in strain, which occurs if the tissue continues to be pulled at higher stress levels. A good example of this linear relation is similar to the model of a stretched rubber band. The greater the load on the rubber band, the more the rubber band stretches. So, as the tension on the rubber band is removed, the band shortens, nearing its original length. Given this behavior, it is referred to as the elastic zone. The amount of stretch (strain) applied to the tissue in this zone is generally experienced during many body movements. Note that the slope (the angle of the curve) in this zone is indicative of the relative stiffness of the tissue. Stiffness is defined as the change in force per unit change in length.41 As such, the stiffer the tissue, the steeper the slope. So tissues such as ligaments will only change length at higher levels of stress compared with tissues of less stiffness, such as loose connective tissue.
The upper level of the elastic region marks a transition from the linear slope to one where the slope begins to flatten. This is called the plastic region and is a point where an increasing level of stress on the tissue results in proportionately increased changes in tissue length, probably due to microscopic failure of the tissue. This is termed the plastic zone because of the tissue damage resulting in permanent deformation (plastic deformation). Unlike the elastic region, the plastic energy is not recoverable in its entirety when the load is removed; additionally, there is a change in its resting length. Continued stretch in the plastic region would result in additional deformation of the tissue and would occur until it reached its initial point of failure. The toe region can include strains up to 3%; the elastic region, from 6% to 10%; and the plastic region, from 10% to 15%.41,112
Viscoelasticity
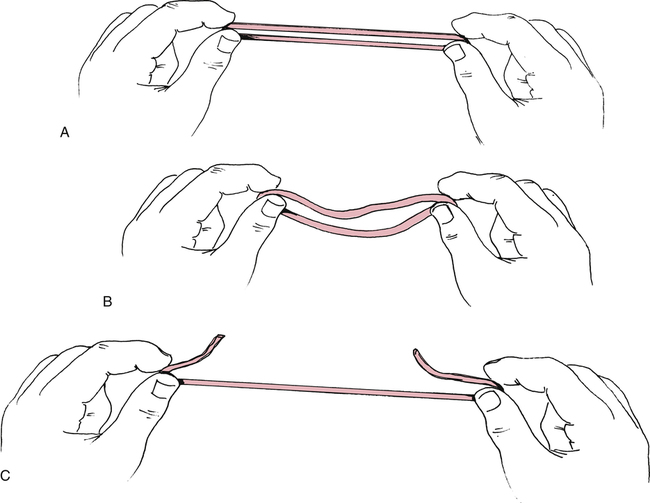
All connective tissue exhibits the property of viscoelasticity, which is simply a combination of the behavior of the properties of elasticity and viscosity.73,76 Elasticity refers to a material’s ability to return to its original state following strain or deformation (i.e., change in length or shape) after a removal of the stress or load. This mutable change is termed elastic deformation and is similar to the changes that occur in a rubber band under high rates of strain. The rubber band rapidly conforms to a new length and is able to return to its original resting length when the stress is removed. However, the rubber band breaks if the degree of stress exceeds the strain capabilities (Fig. 3-3). Viscosity refers to a material’s ability to resist a change in form or to dampen shearing forces. Tissues exhibiting viscosity have time-dependent and rate-dependent properties when forces are applied to them.
The rate at which tissues are stretched has a profound effect on the degree or percent of strain. As mentioned, tensile (distractive) or compressive forces will produce deformation on viscoelastic materials, but will allow return to their original state after removal of the force. Given normal conditions, however, viscoelastic materials do not immediately return to their original state. Viscoelastic materials, unlike pure elastic materials, have time-dependent properties. Slower rates of stress produce greater amounts of strain or elongation, whereas faster rates of stretch produce much smaller amounts of elongation.29,35,119 As such, they are sensitive to the applied force duration. Tissues gradually lengthen when they are subjected to constant or repeated stress of long duration.
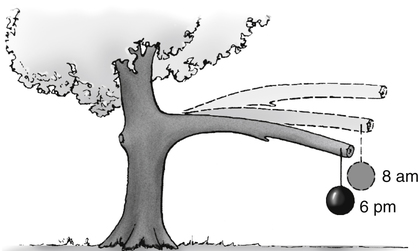
So a viscoelastic material subjected to either a constant compressive or tensile load will initially respond by rapidly deforming; it continues to deform over a finite length of time even if the load remains constant. This deformation of the tissue will continue until a state of equilibrium is reached when the load is balanced. This is called the creep phenomenon (Fig. 3-4),76 which simply means the gradual increase in tissue length that occurs when maintaining a constant stress (or force). For example, if one uses a constant force against the muscle with slow and passive stretching, the muscle will eventually elongate. However, the tissue does not return to its original length immediately when unloaded because of the collagen’s viscous property.73 Essentially, the longer the duration of the applied force, the greater the deformation or stretching of the tissue.
The loading and unloading of tissue is influenced by its viscoelastic properties. This loading and unloading is quantified by measuring the hysteresis area (Fig. 3-5). The loading (solid line) and unloading (dashed line) phases represent a measurement of the stress and strain that is applied to a tissue and then released. The hysteresis area lies between the two lines and represents the amount of energy dissipated in the loading and unloading process.41,73

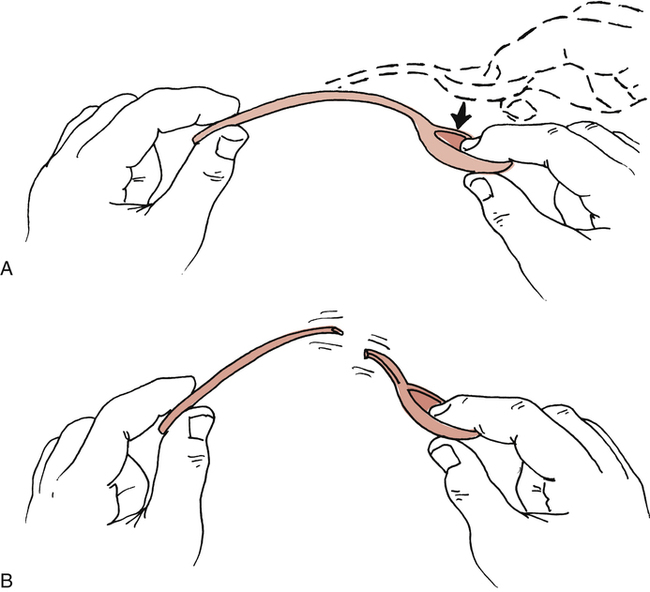
The ability of tissues to recover after stress is extremely important in relation to flexibility. Woo and colleagues136 have shown that increasing the levels of stress produces an increase in collagen within ligaments and tendons, whereas reducing the levels of stress causes weakening in connective tissues. Recovery is the ability of tissues to return to their previous resting state. However, it does not imply that permanent elongation or microscopic damage has not occurred. Plastic deformation is force dependent under slow rates of stress and is used to describe permanent change in a tissue. For example, when a low degree of stress is applied to a plastic spoon, the spoon slowly deforms to a new shape. The spoon breaks if the stress is applied too fast (Fig. 3-6). Lehman and colleagues74 and Warren and co-workers126 have demonstrated that recovery of the tissue’s resting length had occurred after microscopic failure had begun.
Along with stress and the rate of stress applied to tissues, temperature also affects connective tissue extensibility as well as the rate of creep. High temperatures in the range of 37° C (98.6° F) to 40° C (104° F) affect the viscoelastic properties of connective tissue and increase the rate of creep.29,73 The higher the temperature (approximately 45° C [113° F] is the therapeutic upper limit), the greater the degree of elongation with stress before tissue failure.108 Because connective tissue’s viscoelastic and plastic changes occur at higher temperatures, there is less microscopic damage under stress at these temperatures. Studies by Warren and colleagues127 have demonstrated that a temperature of 45° C is needed to reduce tissue damage during strains of 2.6% or less. So to stretch out a connective tissue structure, one should heat it and use a large load over a long period of time to produce creep.96 Low temperatures decrease the rate of creep.
Muscle or contractile tissue responds to stretch by elastic and plastic deformation properties in ways similar to connective tissue. Obviously the contractile properties of muscle allow for the greatest degree of freedom of movement around a joint. Although connective tissue is considered a passive resistant to joint motion, muscle tissue is considered an active restraint to joint motion by virtue of its elastic and contractile elements. Active exercise (muscular contractions) affects intramuscular temperature. Increases to approximately 39° C are observed in exercised muscle.6 Commonly used passive thermal agents that increase tissue temperature are moist heat and ultrasound. The judicious use of active exercise and passive thermal agents before and during stretching programs enhances the effectiveness of the prescribed program.
FLEXIBILITY
Kisner and Colby64 define flexibility as the ability of a muscle to relax and yield to a stretch force. Others have defined flexibility as the ability to move muscles and joints through a full ROM.12,102 In essence, flexibility refers to the degree of normal ROM available. Therefore, flexibility can refer to various measurable components of joint motion. Muscles, tendons, ligaments, skin, joint capsule, and bone geometry all influence the degree of movement in joints. For example, a muscle can stretch or elongate, creating a measurable effect on the joint or joints upon which it acts. If a muscle becomes damaged by trauma or disease or becomes shortened because of immobilization, its ability to stretch and allow freedom of joint motion is affected. Flexibility will diminish over time if tissues are not stretched or exercised using regular and proper stretching regimens.2 As such, the goal of any flexibility program would be to improve or maintain ROM at all joints.
Different classifications of flexibility currently exist, depending on how the tissue is stretched. For example, static flexibility occurs as a result of static stretching, whereas dynamic flexibility relates to moving through a ROM with normal or rapid velocity.2 However, evidence does not support the existence of flexibility as a single general characteristic of the body. Instead, it is specific to particular joints, joint actions, or movements and is highly variable among different individuals.53 An understanding of the properties and components of various connective tissues is fundamental in delivering various stretching and flexibility regimens.
Measuring Flexibility
It is important to assess overall flexibility by measuring ROM at specific joints, because no one composite test provides an index of an individual’s flexibility characteristics.53,54 Subsequently, some measurements of overall flexibility are somewhat difficult, since they involve a complexity of movements over several joints (e.g., sit and reach test).
Measuring joint ROM is accomplished by using standard goniometric instruments. The measuring device most commonly used to measure ROM is the universal goniometer (Fig. 3-7), which is a protractor with degree measurements. The goniometer arms are placed along the proximal and distal components of a joint with the axis centered over the joint, which are then moved in accordance with the body part being measured. The goniometer can be used to measure joint position and ROM at almost all joints of the body.95 Other types of goniometers used less frequently in the clinical setting are the inclinometer, the pendulum goniometer, and the fluid goniometer.

Consistency in measurement is crucial; therefore it is important to use the same type of goniometer for a specific patient each time that patient is measured. Because different goniometers may provide slightly different results, they should not be interchangeable in their use in the clinical setting. For example, when using an inclinometer as the measuring device, it should be used for all future measurements for that patient to ensure consistency.96 For documentation purposes, most authorities recommend using goniometry rather than visual estimates because of its increased accuracy and reliability of measurement.128,137
Joint stability differs from joint ROM in that the ligaments and surface geometry of joint articulations dictate static joint integrity (stability). A patient may demonstrate limited ROM in knee flexion and extension (by goniometry); however, anterior and posterior joint mobility may be excessive and unstable (Fig. 3-8). On the other hand, a patient may demonstrate normal joint ROM, yet when tested statically the joint may be very stable, tight, and unyielding to pressure.

The sit and reach test (Fig. 3-9, A-B), standing toe touch for back and hamstring flexibility (Fig. 3-9, C), seated hip external rotation test (Fig. 3-9, D), and standing knee recurvatum test generally are less specific flexibility tests. These tests and others are used to provide very general assessment of multijoint flexibility. Such tests also can be used as stretching techniques to improve limitations in movement. However, objective clinical documentation of joint ROM is made by joint goniometry.

Factors Affecting Flexibility
In addition to muscles, tendons, and their surrounding fascia, other structures, such as bone, fat, connective tissue lesions, skin, and postural problems, may all lead to flexibility and joint ROM limitations.5 Other factors that may affect flexibility are age and gender.14,25
STRETCHING
Stretching involves elongating the muscles and tendons to the end of the available ROM. As such, applying a tensile force to a muscle results in a transient deformation, which elongates the musculotendinous unit, resulting in a stretch.2,40 Given that the mechanical behavior of connective tissue is primarily influenced by the amount of collagen available,73,119 the amount of stretching that takes place is dependent on the type of connective tissue present (i.e., skin, fascia, ligaments, tendons, joint capsules, and muscle fascia).
Although gradually increasing flexibility to increase ROM is the main goal, other adaptations occur from a regular stretching program. For example, research has shown that as a result of training, the stretch reflex may be reset to a different level.133,134 Several types of stretching exercises have been detailed in the literature and will be described in this section.
Stretching Principles
Stretching is effective primarily because of its mechanical and neurophysiologic effects.69,119 As mentioned, the muscle-tendon unit responds viscoelastically during stretching. However, some stretching exercises are based on the neural inhibition of the muscle undergoing stretch as well. In this case, a decreased reflex activity would result in reduced resistance to stretch, resulting in further gains of joint ROM. Most likely, both mechanisms are responsible.
It is important to note that stiffness relates to a tissue’s ability to resist stretch and indicates the amount of deformation proportional to the load applied.81 So, the stiffer the tissue, the less compliance it has and the less likely it is to stretch; conversely, less stiffness means greater compliance. It stands to reason then that flexibility training is designed to decrease the stiffness of the muscle-tendon unit.69,119 Furthermore, a rapidly applied stretch results in a greater resistance to that stretch.
Both mechanical and neurophysiologic components are inherent within muscular flexibility.43,50,105,118,119 However, some researchers believe that the ability of stretching to produce greater flexibility is primarily a result of the viscoelastic nature of muscle and connective tissue.84,119 As such, the most resistance to stretching probably is due to the connective tissue framework and sheathing from within and around the muscle and not the muscle itself (since the muscle itself can be stretched to 150% of its resting length); this includes the epimysium, perimysium, and endomysium and may even include the sarcolemma.107,109,116,117
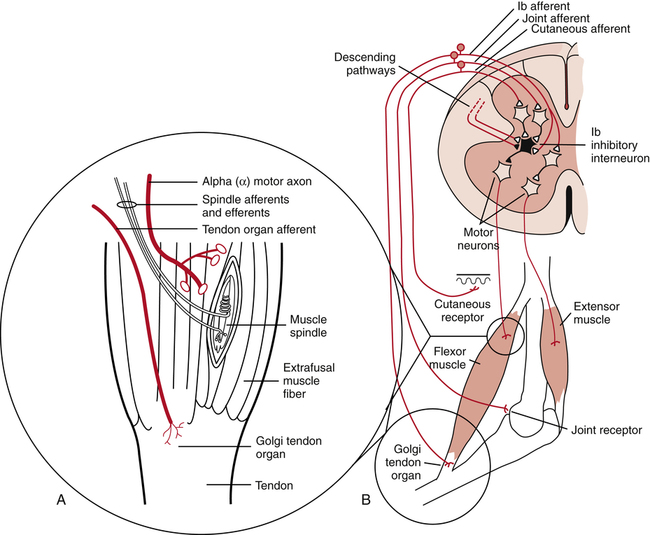
On the other hand, many researchers suggest that the immediate result of stretching is attributed to neurophysiologic phenomena.69 They categorize these phenomena as either a stretch tolerance or active contractile responses and claim that the limiting factor during stretching is the muscular resistance secondary to reflex activity. A stretch tolerance simply means an accommodation to the discomfort of stretching over time. With this philosophy, the aim of stretching is to inhibit the reflex activity, subsequently decreasing the resistance and improving ROM. Several other researchers agree and recommend certain types of stretching for its reduction in reflex activity.3,43,50 Muscle spindles and Golgi tendon organs are the mechanoreceptors responsible for the contractile responses (Fig 3-10).
Warm-up
Warm-up is necessary to help prepare the tissue for activity. Stretching alone before exercise is not recommended by most researchers and health professionals.65,66,111,124 As such, the purpose of warm-up exercises, including stretching, is to prepare the body for the stresses it will encounter during an activity or sport and is necessary for increasing the core body temperature. Heat is produced with muscle contraction, thereby increasing the intramuscular temperature.23 ROM increases as a result of warmed tissue.107 A warmed muscle will be able to contract more forcefully and relax more quickly,15 thereby enhancing work production for those muscles used.16 In training, a general body warm-up is needed first. The beneficial effects of a warm-up before strenuous activities include the following:
 Blood flow to working muscles is increased.
Blood flow to working muscles is increased.
 Temperature in working muscles is increased.
Temperature in working muscles is increased.
 Cardiovascular response to sudden, dynamic exercise is improved.
Cardiovascular response to sudden, dynamic exercise is improved.
 Breakdown of oxyhemoglobin for the delivery of oxygen to the working muscles is increased.
Breakdown of oxyhemoglobin for the delivery of oxygen to the working muscles is increased.
With warm-up, the risk of connective tissue and contractile tissue damage is reduced. Warm-up protocols usually last from 10 to 25 minutes or more and may vary somewhat, depending on the nature of the activity or event.8 The warm-up should be intense enough to cause an increase in body temperature, but not so intense as to cause fatigue. So one should taper the warm-up 5 to 10 minutes before the actual event.3 It is clinically assumed, of course, that a more compliant muscle can be stretched further and is therefore less susceptible to injury.48
However, some think that the warm-up period may not be the best time to stretch for increasing ROM, primarily because of increased tissue stiffness. Since the concept of stretching to prevent injury has come under question, benefits of stretching before activity may be incorrect. Activity of gradually increasing intensity (dynamic stretching) may be more appropriate than static stretching as a warm-up activity.96 Some researchers have examined the combination of stretching and active warm-up and have shown that the decrease in stiffness mainly results from increased muscle temperature and not stretching.85,104
Increasing intramuscular temperature to help increase ROM may also be achieved through external means.110 Henricson and colleagues57 reported on results that followed the application of heat to the hip. Although heat alone did not improve hip ROM, stretching without heat did increase hip ROM, and stretching with heat combined gave the greatest increase in ROM, maintaining it for 30 minutes. These results are consistent with others,62,74,127 who report that collagen extensibility increases and musculotendinous stiffness decreases with heat. Bear in mind, however, that most authors recommend using exercise as the primary way of increasing intramuscular temperature.96 It has not been definitively shown whether a general warm-up serves to improve sports performance.17,18,21,46
Stretching Techniques
In discussion of flexibility and associated stretching programs, the stretching of nonpathologic muscle must be separated from stretching noncontractile connective tissue. Improving muscle extensibility in nonpathologic conditions and in adaptive muscle shortening after injury or immobilization requires a complement of active exercise techniques and thermal agents. Types of stretching exercises are static stretching (active and passive), ballistic stretching, dynamic stretching, and proprioceptive neuromuscular facilitation (PNF) techniques (contract-relax, contract-relax with agonist contraction, and hold-relax). Research has shown that all four techniques have been shown to increase flexibility.31,56,61,80,82,105 Essential to a successful stretching program for improving flexibility is the proper execution of the exercises.
Static stretching
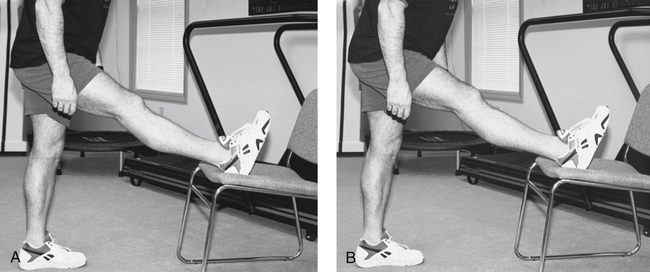
The most common form of stretching exercise that is used to safely increase the ROM in a joint is static stretching. This form of stretching allows one to sustain a controlled stretch by placing a muscle in a fully elongated position and holding that position for a period of time (Fig. 3-11). A passive static stretch implies that the force is applied externally (i.e., with a partner or gravity-assisted) (Fig. 3-12). If an opposing muscle action is used to aid the stretch, then the stretch is called an active static stretch. However, to obtain optimal passive stretching, all voluntary and reflex muscular resistance must be eliminated.

Research supports that slow passive stretching through the ROM will not produce muscle activity in normal relaxed subjects.13,107 As such, the muscle should be slowly and passively stretched to a new length, so that the stretch reflex is not elicited. Additionally, the stretch should not elicit pain.3,105 As is described later, the stretch is maintained for an extended period of time before being returned to its starting position. Subsequently, a lengthening of the muscle is accomplished.
Athletes use static stretching before sports activities as part of a warm-up before a workout and as part of a cooldown after a workout. Because intramuscular temperature rises to approximately 39° C during exercise,6 active general body movements can improve muscle temperature before stretching is done. Most warm-up programs use primarily active static stretches, using gravity to assist the stretch.
Studies on rat tail tendons74 demonstrated that ruptures occurred with 31% of normal loads when temperatures were at 25° C, whereas increasing temperatures to 45° C delayed tendon rupture until 102% of normal load. This demonstrates that stretching at normal body temperatures may damage tissue,127 but elevating tissue temperature before and during prolonged stretch is less damaging.126,127
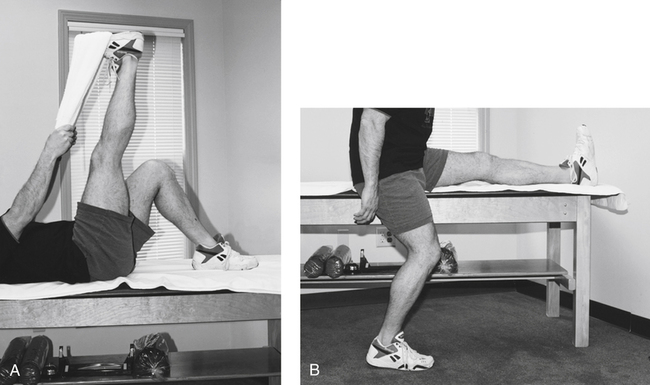
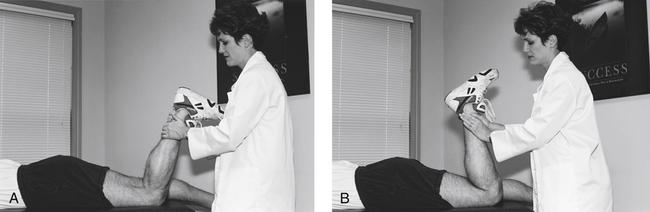
Static stretching has distinct advantages, such as reduced chance of exceeding strain limits of tissues, reduced energy requirements compared with other forms of stretching, and reduced potential for muscle soreness.29,108,136 The ease and practicality of teaching patients to perform static stretching is another advantage. For example, hamstring stretches can be taught with the patient in various positions (Fig. 3-13). The general goals of static stretching are to prevent or minimize the risk of soft-tissue injury from participation in sports or physical activities, improve movement and increase flexibility, and prevent contracture.8,64
Ballistic stretching
Another technique used quite often by athletes is ballistic stretching (Fig. 3-14). Many believe that this is the least desirable technique, because it potentially places the tissue at risk secondary to the use of jerking or bouncing movements at the end of the ROM to stretch the muscles.71 Athletes use dynamic, high-velocity, and even violent motions during sporting events and require extraordinary flexibility to prevent or reduce the risk of potential musculoskeletal injury. Relatively high-velocity or quick bouncing may not be appropriate for many patients. The potential for tissue damage exists in all forms of exercise, but ballistic stretching may increase the risk of connective tissue and contractile tissue trauma, although a narrow segment of patients may benefit.

The reason ballistic stretches are considered undesirable is that they stimulate the muscle spindles during the stretch. This results in a continuous resistance to further stretch, which then causes a high rate of tension strong enough to potentially injure the musculotendinous unit.65,107,123 Ballistic stretching does not imply aggressive, violent, high-velocity stretches throughout the ROM; instead it involves a slight but progressively greater bounce at the end of the range achieved through static stretching.
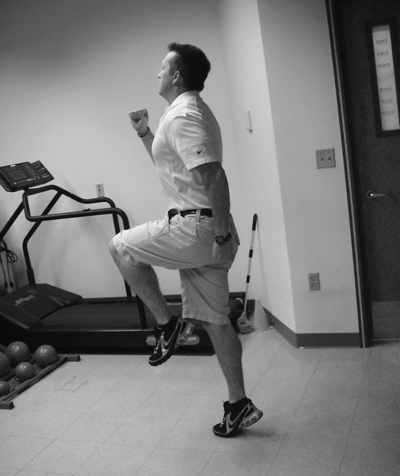
Dynamic stretching
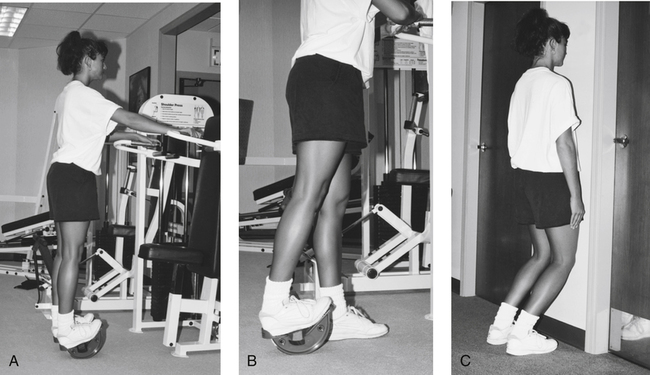
A type of stretching technique that has become increasingly popular is dynamic stretching. With dynamic stretching, muscular contraction is used to stretch a muscle; the effect is to increase or decrease the joint angle where the muscle crosses, thereby elongating the musculotendinous unit as the end ROM is obtained.10 What sets dynamic stretching apart is that it uses activity-specific movements, thereby preparing the muscles by taking them through the movements used in a particular sport. An example of this would be a sprinter who would walk using exaggerated long strides, thus emphasizing hip flexion and extension (Fig. 3-15). This subsequently actively contracts and stretches the muscles used by the sprinter, namely the hip flexors and extensors.60 Dynamic stretching does not incorporate end range ballistic movements that are bouncy or jerky in nature. Rather, all movements are under control.96
Proprioceptive neuromuscular facilitation
Another technique used to facilitate ROM increases via stretching is called proprioceptive neuromuscular facilitation (PNF). PNF is a system of therapy that uses different techniques designed to promote neuromuscular responses via stimulation of the proprioceptive system.122 These techniques use volitional contractions to increase ROM by decreasing the resistance caused by the spinal reflex pathways.24 PNF stretching uses movements in diagonal patterns along with an isometric contraction before the stretch; this allows greater gains in ROM than stretching alone. However, depending on the clinical setting, many clinicians have modified the various PNF patterns, deviating from the proposed diagonal patterns originally described by Knott and Voss64a to straight plane patterns. As a result, it is difficult to determine if the effects of PNF treatment are consistent among practitioners and in the research literature.
PNF stretching techniques, which are based on the stretch reflex, appear to increase ROM through the stimulation of the proprioceptors2 and have been found to produce greater increases in ROM than static stretching.91,101 Two neurophysiologic sensory receptors involved with the stretch reflex are the Golgi tendon organs (GTOs) and the muscle spindle. The GTOs are inhibitory sensory receptors located within the musculotendinous junction that signal tension in a muscle (see Fig. 3-10, B). Stimulation of the GTO results in self-inhibition of that muscle, termed autogenic inhibition. They also signal minute changes in muscle tension, thereby providing information about muscle contraction.63
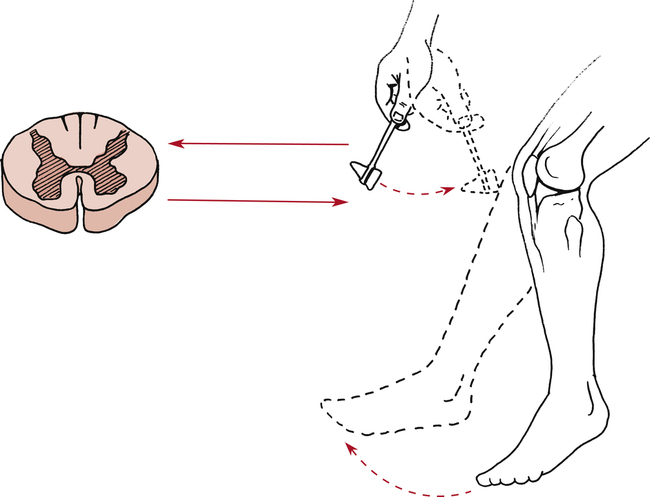
Muscle spindles are excitatory specialized fibers within the muscle (see Fig. 3-10, A) that are sensitive to changes in muscle length as well as maintenance of that length. When a muscle is stretched, the spindles send messages to the spinal cord, which in turn signals the muscle to contract. The classic clinical demonstration of the stretch reflex is produced by tapping the relaxed patellar tendon, which causes the reflexive contraction of the quadriceps. The muscle spindles within the quadriceps are activated by the quick stretch of the patellar tendon, causing the quadriceps to contract reflexively (Fig. 3-16).63
Despite the advantages, PNF stretching has some disadvantages as well. For example, it is more time consuming than other methods, requires skillful application by trained professionals to be effective, and may lead to mild complaints of patient discomfort.108 Some of the more commonly used techniques are contract-relax, contract-relax with agonist contraction, and hold-relax.
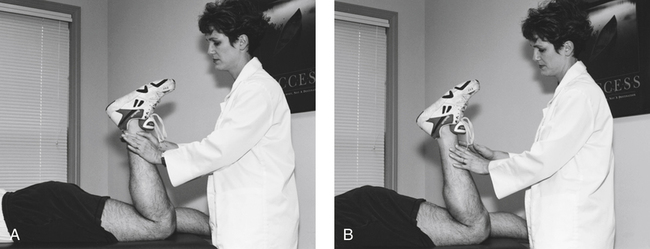
The contract-relax technique involves instructing the patient to relax the affected muscle while the therapist passively moves the limb to the limit of motion (until the person feels a stretch). The patient is instructed to actively contract the restricted muscle (antagonist) against the manually applied resistance of the therapist for 5 to 8 seconds.1 The patient is then instructed to relax while the therapist passively moves the limb to the new limits of motion, at which point the clinician holds the stretch for 10 seconds (Fig. 3-17). This relaxation of the antagonist muscle during contraction is an example of autogenic inhibition. The process is repeated by continuing from the new limit of pain-free motion until the required number of repetitions is performed or until no more range is gained.1
In the contract-relax with agonist contraction technique, there is a contraction of the opposite (agonist) muscles instead of the shortened or restricted muscles.1 In this case, the limb is taken to the point of stretch while the clinician applies manual resistance against the muscle being stretched for 5 to 8 seconds (as in the contract-relax method). The muscle is then relaxed while the agonist muscle concentrically contracts; this facilitates the stretch using the principle of reciprocal inhibition (Fig. 3-18). In reciprocal inhibition, voluntary isometric contraction of the agonist muscle group results in a subsequent reflex inhibition on the muscle groups being stretched (reciprocal inhibition). The clinician again takes up any slack and holds the new position for 10 seconds before continuing.
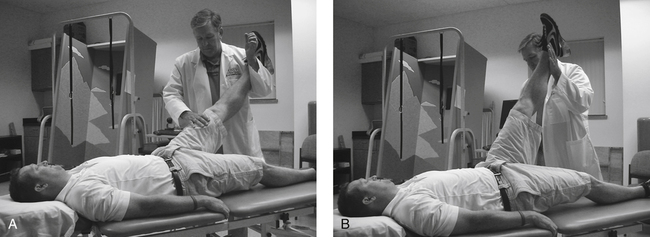
The hold-relax technique is similar to contract-relax. However, with this technique, the patient actively moves the limb to the end of pain-free motion. The patient isometrically contracts against the force applied by the therapist at the end of the ROM for 5 to 8 seconds as resistance is slowly increased. After holding the contraction for the requisite amount of time, the patient is instructed to relax. The patient then actively stretches the limb to the new limits of motion (Fig. 3-19).1
Duration, Frequency, and Intensity of Stretching
The specific duration, frequency, intensity, and number of stretching repetitions varies in the literature. Stretch duration depends upon the joint targeted, the flexibility goal, and the type of stretching technique used. Generally, static stretches may be held in a fully elongated position for anywhere from 10 to 60 seconds, with most research recommending that stretches be held between 15 and 30 seconds.8–10,81,103,122 An attempt is then made to extend the stretched position farther within tolerable limits (Fig. 3-20). However, because of the structural diversity of tissue, predicting the duration of stretch for each tissue becomes very difficult.73 Current American College of Sports Medicine (ACSM) guidelines recommend 3 to 5 repetitions for each stretching exercise.98
The limits of motion achieved during a stretching program depend on the patient’s tolerance, age, pathologic condition (if any), motivation, and commitment. The muscle’s ability to adapt is a prolonged process. Patients must be cautioned not to exceed their pain limits and must receive counseling about the fact that many sessions of stretching are needed to produce change and lasting improvement. Approximately 6 weeks of stretching are necessary to demonstrate significant increases in muscular flexibility.37 An individual must stretch at least three times per week to improve flexibility. An individual must stretch at least 1 day per week to maintain the flexibility gained during the program.108
Intensity
Increases in ROM can be significantly affected by the intensity of the stretch.107,125 Structural damage subsequent to stretching could result with increased levels of force and may result in structural weakening of the muscle-tendon unit, thereby increasing the risk of injury.94,120 The appropriate intensity for static stretching is to stretch slowly and hold the position at low force levels. This is most often communicated to the individual as pain-free or mild discomfort.
How long does it last?
There is little reported on the long-lasting effects of stretching. Some researchers have reported that stretching techniques using cyclic and sustained stretching for 15 minutes on 5 consecutive days increased hamstring muscle length with a significant percentage of the increased length being retained 1 week posttreatment.115 Others reported that the knee ROM was able to be maintained for 3 minutes, but had returned to prestretched levels in 6 minutes36; whereas other researchers have reported that increased ROM from stretching remained for up to 90 minutes.45,89 These differences have been explained by variations in warm-up, stretching position, stretching force, and stretching duration.138 Some research has shown that stretching at least once a week after a 30-day training program will maintain the gained flexibility.123
Comparisons of Different Stretching Techniques
All stretching techniques previously discussed have been shown to increase flexibility and ROM.47,49,79 However, it has not been adequately defined in the literature as to the appropriate stretching frequency and duration for long-lasting changes in flexibility.100 It is also not completely evident which stretching technique increases flexibility most effectively. Ballistic stretching and static stretching appear to be similar in their effects on flexibility,56,61,105 yet existing research indicates that dynamic stretching may produce about the same flexibility gains as static and ballistic stretching.10
Although many studies have revealed that PNF may be the preferred method for increasing flexibility over static and ballistic stretching,27,42,52,101,118 direct comparison between methods is very difficult to determine because of the differences in methodology, experimental design, procedures, and measurement instruments and the use of inadequate control groups.96 Additionally, some studies found no significant differences between techniques.56,79,86,91 Some authors have reviewed stretching studies and reported conflicting evidence as to the efficacy of these methods44,52; they reported that most of the differences between studies were probably due to variations in training methods, measuring instruments, and confounding variables.
Proposed Stretching Benefits
Enhanced Flexibility
Research has shown that a long-term, routine stretching program can result in increased long-term flexibility, whereas an acute stretching program does not.10,66 Wiktorsson-Moller and colleagues130 reported that stretching significantly increased hip ROM for flexion/extension, hip abduction, knee flexion, and ankle dorsiflexion. The effect was significantly greater than that obtained by massage and warming up separately or combined. Similarly, Williford and associates132 showed that increases in flexibility could occur as a result of a static stretching training program.
Relief of Muscular Soreness
Previous research has indicated that slow stretching exercises were able to reduce postexercise muscular soreness,30,32 but other research, examining the effect of static stretching on soreness, revealed no significant effect on perceived pain compared with a control group.83 Later research showed that stretching had no effects on decreasing exercise soreness over the postexercise period or immediately after an acute bout of stretching.22,51 In fact, some research has demonstrated that stretching may actually cause muscle soreness. In a study investigating the effects of static and ballistic stretching on delayed onset muscle soreness (DOMS), researchers found that similar bouts of static and ballistic stretching induced significant increases in DOMS in subjects unaccustomed to such exercise.114
Muscle Relaxation
The literature has shown that chronic increased muscular tension can result in negative side effects, such as high blood pressure, headaches, ulcers, and muscle and joint pain.72 Subsequently, many individuals use certain types of stretching as a way to facilitate muscle relaxation. An example of this type of flexibility training is used in yoga.2 The belief here is that chronic tension affects muscles so that they become less strong, less supple, and not as capable of absorbing the shock and stress of various types of movements. As such, stretching may be implemented to facilitate muscular relaxation, thereby decreasing stress and muscular tension.33,34 A possible explanation may be that, with stretching, the muscle spindles may adapt to the stretch, or while held at a constant length, force relaxation may occur, which would decrease the tension on the muscle. In examining electromyograms (EMGs) before and after warm-up, Mohr and colleagues88 found that muscle activity during static stretching of the gastrocnemius muscle for about 30 seconds was significantly lower and therefore sufficient to attain muscle relaxation.
Injury Prevention
Evidence is not clear as to whether stretching before or after exercise actually decreases the chance of injury. Some research has shown that stretching may decrease the rate of injury.28,55,87,106 Researchers also stated that stretching, as part of a warm-up or a rehabilitation program, decreased the percentage or recurrence of injuries.39 On the other hand, research has also shown that stretching is not effective in preventing injury.121 A 12-week training study of 1538 male army recruits revealed that stretching had little influence on injuries associated with weight-bearing physical training such as running, marching, and walking.99
Performance Enhancement
Many assume that performance is enhanced by preactivity stretching and usually point to sports that require extreme ROM at particular joints (e.g., gymnastics and pitching). However, no conclusive data support a correlation between flexibility and/or stretching and performance. It is generally agreed that a warm-up is necessary before exercising in order to perform an activity safely and successfully.65 Of course, stretching is widely accepted as an important part of the warm-up. Furthermore, many have traditionally believed that performing stretching immediately before physical activity will improve performance.48 Though it is plausible that increased flexibility may potentially improve performance in many activities where ROM is necessary to perform certain skills, whether preperformance stretching can actually improve performance is questionable.66,113,131 Some studies have reported that preperformance stretching neither helps nor inhibits performance,49,67 whereas other studies have revealed negative performance effects.45,68,124
The reason for these negative effects, according to some researchers, is probably that the muscle-tendon unit becomes weaker after acute stretching and is thereby less able to produce high intensity force. Consequently, there is a period of time during which the muscle-tendon unit stays stretched (lag period), in which it may need to “take up the slack” before peak tension is reached. Therefore stretching immediately before a performance task may cause a strength deficit, resulting in impeded performance.124 Because of this, it has been suggested that low intensity muscle contractions should be performed immediately before sport performance (i.e., dynamic stretching).19
When to Stretch
Very little literature is available to determine when stretching should take place in an exercise program. Some believe that stretching should be part of the warm-up to enhance musculotendinous extensibility, but should not constitute the entire warm-up.70 Wiktorsson-Moller and associates130 showed that warm-up before stretching resulted in significant changes in joint ROM. Some think that stretching should not be performed at the beginning of a warm-up routine.70,107 They believe that the tissue temperatures may be too low for optimal muscle-tendon function, subsequently leading to a less compliant tissue, which may not adequately prepare the tissue for activity. As such, many authors recommend at least 5 minutes of light progressive exercise before stretching.107 Conversely, some discourage exercise before stretching, stating that warmed up muscle tissue does not necessarily stretch better nor is it less likely to be injured.93
Some researchers found that stretching should be performed after an exercise session because of the improved joint ROM.85 However, Cornelius and colleagues26 revealed that performing static stretching before, after, and both before and after each workout in a 6-week program did not make a difference in increasing ROM. All produced significant increases in ROM.
Stretching of Soft-Tissue Contractures
The stretching of soft-tissue contractures involves muscle, capsule, tendon, ligament, bursa, and skin. Many options exist for the therapist when prescribing stretching exercises for patients after immobilization or injury, which differ from static, ballistic, or PNF stretching. Long-duration, low-load static stretching has been an effective technique that produces long-lasting connective tissue changes.29,74,126,127 The PTA must recognize adaptive changes that occur in various soft tissues after injury or immobility.
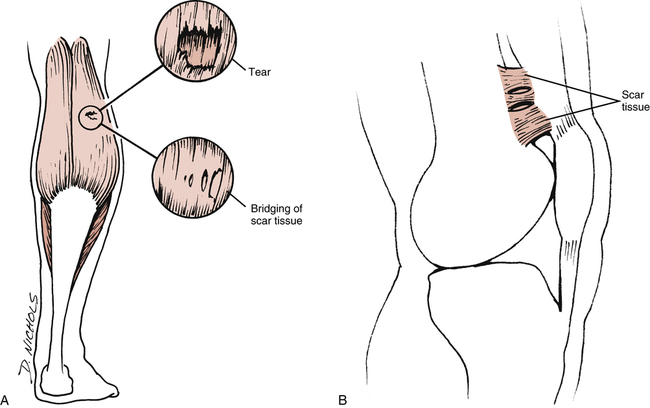
Initially, scar tissue is formed, which may result in the development of a scar contracture if the tissue is not adequately mobilized. A contracture, in this case, is defined as a permanent or transient limitation of movement or shortening of muscle or other soft tissues; in other words, a contracture is the result of healed tissue that forms a fixed, rigid scar and causes cosmetic deformity or functional deficits.58 Scar tissue formation may be the result of adhesions and other tissue damage (Fig. 3-21, A). An adhesion involves a limitation of function resulting from scar tissue that forms between structures. For example, when scar tissue forms after knee surgery, it can bind down and cross-link collagen tissue, resulting in adhesions around the patella, suprapatellar pouch, and quadriceps tendon (Fig. 3-21, B).
Generally, immature scar is defined as adaptable for up to 8 weeks and becomes progressively less changeable for up to 14 weeks. Scar becomes quite inextensible at 14 weeks and is termed inadaptable, or mature scar.4 Adaptable scar is highly vascular, with many cells (including myofibrocytes) that give the scar the ability to contract. Immature scar tissue also has a high rate of remodeling,4 which is the process of tissue restructuring in response to stress or immobilization.29
As new scar tissue is formed, the collagen fibers become highly unorganized and arranged randomly, creating an immobile structure.78 Adaptable or immature scar tissue becomes increasingly organized and oriented, with specific directional lines of stress. The formation of collagen fibers are in response to stress imposed from mechanical loads.58 Where stretching is concerned, the PTA must be attentive to the following critical components:
 The nature of scar tissue is time dependent and stress reactive.
The nature of scar tissue is time dependent and stress reactive.
 Immature, adaptable scar tissue is fragile.
Immature, adaptable scar tissue is fragile.
 At 5 days, new scar is only 10% of its maximum potential strength.
At 5 days, new scar is only 10% of its maximum potential strength.
 At 40 days, new scar is 40% of its maximum strength.
At 40 days, new scar is 40% of its maximum strength.
 At 60 days, new scar is 70% of its maximum strength.
At 60 days, new scar is 70% of its maximum strength.
 At 12 months, new scar is approximately 100% of its maximum strength.
At 12 months, new scar is approximately 100% of its maximum strength.

 Low-load, long-duration stretching of joint contractures in combination with thermal agents to preheat extensible connective tissue has proved effective in the treatment of soft-tissue contracture.59,75,77 Long-duration stretching means stretching over a period of 20 to 60 minutes.
Low-load, long-duration stretching of joint contractures in combination with thermal agents to preheat extensible connective tissue has proved effective in the treatment of soft-tissue contracture.59,75,77 Long-duration stretching means stretching over a period of 20 to 60 minutes.
Clinically, the following areas are involved in a low-load, prolonged stretch technique:
1. Preheat the involved structures with moist heat or ultrasound.29
2. Place the involved structures in a position of comfort, not maximum stretch. This is an extremely important point. To elicit relaxation, the involved structures must be placed in a supported and comfortable gravity-assisted position.
3. Maintain moist heat application during the entire course of treatment (20 to 60 min).
4. Apply stress or load gradually and minimally. With new immature scar, gravity alone may be enough to clinically effect change. With mature scar, only slightly greater loads should be used. This is a critical point. Lentell and colleagues75 found that the magnitude of force used in their study (0.5% of body weight) to create a significant long-lasting change in motion fostered such relaxation that many subjects were not even aware of stretching taking place during the procedure. In an effort to gain knee extension after surgery, for example, it would behoove one to use this technique to avoid reflexive splinting or muscle guarding (Fig. 3-22).
5. Allow the patient to rest or recover for a few minutes during the course of treatment if the sensation of stretch becomes too uncomfortable.
6. Maintain heat application for 5 to 10 minutes after removal of the loads. Some researchers107 have advocated the use of ice packs after stretch in this protocol. Lentell and colleagues75 did not find cooling to be effective in their study. However, cooling the involved structures after stress may be effective in selected cases where pain and an inflammatory response are present.
7. Initiate isometric contractions after the application of heat and passive stretching to enhance strength gains at the new end of ROM.
Lentell and colleagues75 demonstrated the effectiveness of applying heat before and during low-load, prolonged stretching and external rotation of nonpathologically involved shoulders. Heat application before and during such stretching was clinically superior to bouts of stretching alone, stretching plus ice, and a heat-stretch-ice protocol. Clinically, few contraindications exist when attempting to gain motion after specific surgical procedures.
The clinical application of low-load, prolonged stretch can be modified to varying degrees depending on the surgical procedure, time constraints of healing, and goals of the rehabilitation program. For example, supine wall slides are a modified technique that uses some of the points of low-load, prolonged stretch (Fig. 3-23). When attempting to gain knee flexion range, it is wise to preheat the quadriceps muscles and suprapatellar pouch before stretching. Next, the patient is placed in a supine position and the foot of the involved limb put on a towel against a wall. To reduce friction against the wall, the contact surface of the towel is lightly coated with baby powder so it will slide more easily against the wall. As the patient relaxes, gravity assists in knee flexion and the foot slides down the wall.

This concept can be modified further. In keeping with the example of gaining knee flexion range, the use of isotonic exercise equipment can be helpful. With the patient in a seated position on a knee extension machine, moist heat or ultrasound can be used before and during the stretch (Fig. 3-24). Many knee extension machines are manufactured with an adjustable range-limiting device that allows the patient to adjust the starting and stopping angle of the exercise. Before the stretch is begun, the patient’s hips are secured with straps to keep them from rising during the treatment. An angle is selected that is comfortable to the patient. As the tissues are continually heated, a very gradual increase in the flexion angle is initiated. The angle does not have to be excessive to be effective. Thus the protocol remains essentially the same, but the equipment and the position of the patient are changed.
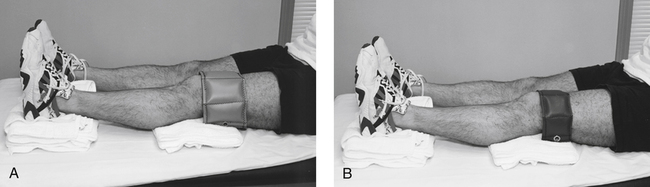
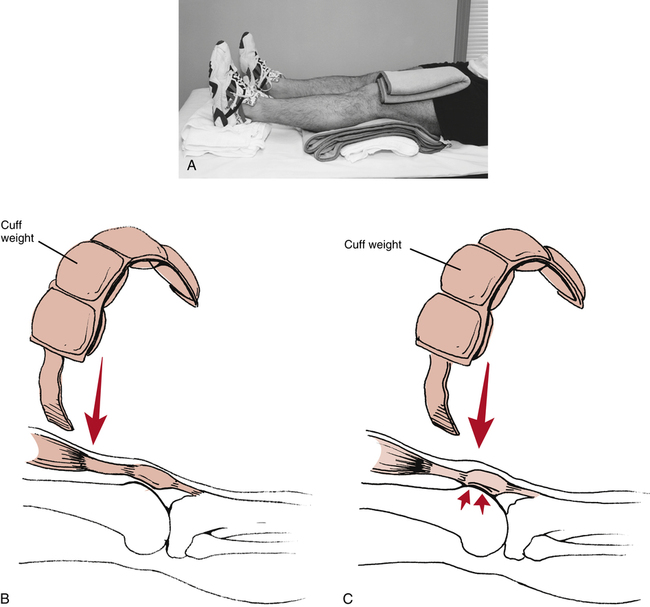
The knee serves as an excellent example to further describe and clarify methods to improve ROM by prolonged static stretching. To gain knee extension range, the patient can be supine with moist heat applied behind the knee (popliteal fossa) and on the hamstring and quadriceps. The heel of the involved limb is placed on a small folded towel (Fig. 3-25, A). If the knee is contracted to −20°, for example, towels are added under the hot packs under the knee to ensure a very comfortable starting position. During the course of treatment, small layers of towel can be removed gradually to allow for improved range of knee extension. As a progression to this technique, a small vertical force can be applied on the knee. Care should be taken to ensure that this force is sufficiently small (1 to 2 lb or lighter) and that it is applied superior to the patella to avoid compressive forces between the patella and femur (Fig. 3-25, B-C).
The patient is brought to a sitting position to enhance this stretch further. A towel is used to dorsiflex the involved foot, and the patient is instructed to slowly lean forward to stretch the hamstrings (Fig. 3-26, A). Simultaneous isometric quadriceps sets also are used to improve strength at the new limits of knee extension.
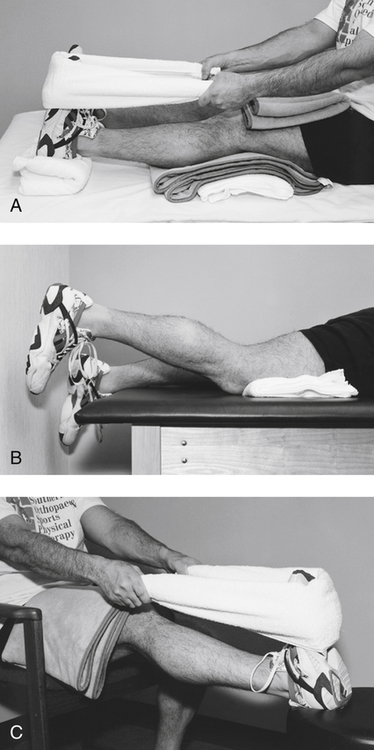
Gaining knee extension can be achieved in a prone position as well (Fig. 3-26, B). However, care must be taken to elevate the patella off the table and thereby prevent excessive patellofemoral compression. This is done by placing a small folded towel superior to the patella. This position works well when only slight degrees of motion are needed (5° to 10° of knee extension). This procedure also can be done on an isotonic exercise apparatus following the same process as described with gaining knee flexion on an isotonic exercise machine. Knee extension range also can be improved in a sitting position, with or without the aid of isotonic exercise equipment (Fig. 3-26, C).
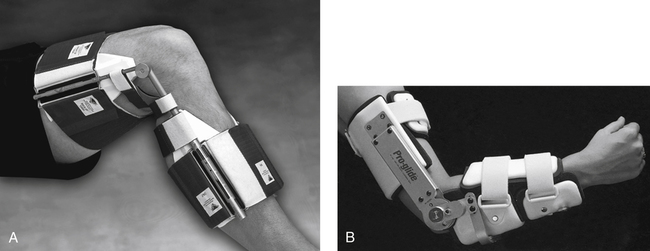
There are many commercially available tools that use the concept of low-load, prolonged stretch. Dynasplint (Dynasplint Systems, Inc.) and Pro-glide (LMB) are two examples of dynamic splints used to progressively load selected joints to gain motion (Fig. 3-27). An arrangement of pivot points and incrementally adjustable degrees of tension provides the levels of stress needed to effect change in joint motion. The selection of patients for use of one of these splints must be made carefully. Skin integrity is an issue that must be addressed in the elderly population. Metal hinges and spring-loaded tension flanges may not be appropriate for this population because of the weight of the devices and the patient’s potential for skin breakdown.
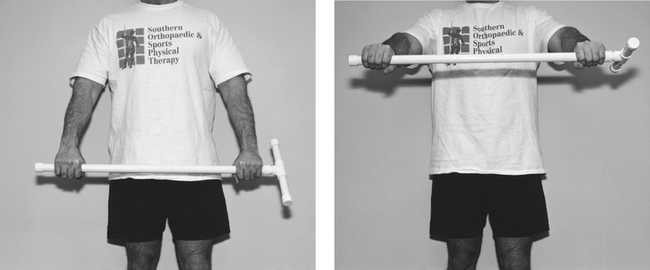
Simple tools for dynamic stretching can be used at home. A wand, cane, or shortened broomstick can be used for general shoulder flexibility (Fig. 3-28, A). Increased mobility can be gained by using the unaffected arm to assist the affected extremity (Fig. 3-28, B).
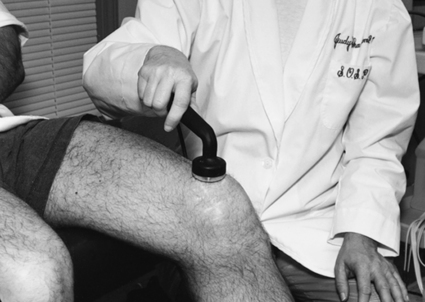
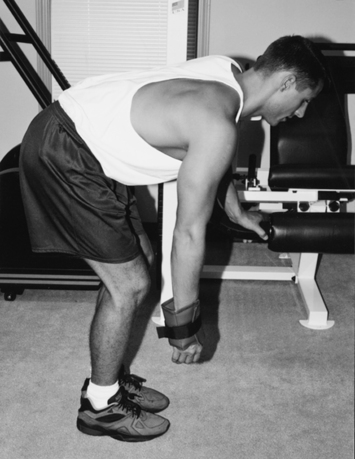
Codman’s pendulum exercises are effective for gaining relaxation and small degrees of motion in the shoulder. Relaxation is paramount to the effectiveness of this exercise. In one exercise technique, the patient is placed prone on a treatment table and a very light weight is held in the hand of the affected extremity. This light distraction force is used in conjunction with gradual, light oscillations in various directions (Fig. 3-29). Relaxation is enhanced by applying moist heat followed by ultrasound to the affected joint before pendulum exercise. When one is teaching the oscillation component of this exercise, it must be made clear that muscular contractions must not be used to initiate and maintain the prescribed motions. The oscillation movements can be initiated by gently swinging the upper body or torso.
[/level-membership-for-orthopaedics-category][not-level-membership-for-orthopaedics-category]3
Flexibility and Stretching
1. Describe viscoelasticity and the properties associated with collagen.
2. Explain the stress-strain curve and factors that influence change.
3. Discuss Golgi tendon organs (GTOs) and muscle spindles.
4. Discuss how temperature affects connective tissue.
5. Define and discuss range of motion, flexibility, and stretching.
6. Outline various methods used to measure flexibility.
7. Identify and describe various stretching techniques.
8. Discuss precautions and essential components of stretching program development.
9. Discuss at least two proposed benefits of stretching.
10. Explain how stretching might negatively impact activity performance.
11. Describe the clinical applications for stretching soft-tissue contractures.
12. Describe and contrast the differences and similarities between scar tissue and adhesions.
Enhancing flexibility is an important component of a fitness program7 and is useful, not only for sport-specific activities, but also for activities of daily living (ADLs). The need for flexibility is particularly necessary if mobility has been impaired, resulting in compromised range of motion (ROM). ROM is the amount of movement available to a joint moving within its anatomic range. Muscular imbalances due to shortened muscles may lead to faulty postural alignment that may lead to injury and joint dysfunction. The ability to restore ROM is crucial when implementing or following a rehabilitation program; consequently, being able to incorporate stretching exercises to restore flexibility as well as normal ROM and function becomes a primary goal for the physical therapist assistant (PTA).
Many clinicians emphasize that having a more flexible body is more efficient, improves muscle balance, and more easily undergoes strength and endurance training. Overall purported benefits of flexibility due to stretching include injury prevention, quicker recovery from workouts, a reduction in post exercise soreness, and facilitation of relaxation.2,129 However, the effects of stretching on performance is somewhat more controversial. Some literature shows that it may potentially help improve performance,48 whereas other literature and research reveal potential detrimental effects on maximal performance activities after stretching.66,113,124,131 Research into flexibility and stretching is ongoing in an attempt to determine the effects of stretching on the body. Consequently, some of the long-held beliefs about stretching, especially regarding performance, are being challenged.
PROPERTIES OF CONNECTIVE TISSUE
Just as amino acids are the building blocks of protein, tropocollagen is the building block of collagen (Fig. 3-1). Collagen fibers are made of short subunits (fibrils) and are found in varying amounts within the different connective tissues: bone, tendon, muscle, skin, hyaline cartilage, and joint capsule.20,41,119 Collagen is a protein building block of connective tissue and it provides the strength needed to withstand high levels of tension and force during movement and exercise. There are more than 20 types of collagen, but the majority of the collagen in the body consists of types I, II, and III.38 Of these, type I collagen is the most abundant in the body.
Type I collagen fibers are thick fibers gathered into bundles and display very little elongation when placed under tension (they have an ability to resist pulling). Type II collagen fibers, on the other hand, are thinner and possess slightly less tensile strength. These fibers are observed primarily in tissues such as articular cartilage and the nucleus pulposus. Type III collagen serves mainly in a structural support capacity and is found in expansible organs (e.g., arteries, liver, lungs).58 It is also common in fast growing or healing tissue and is often seen at the early stages (phase 1) of wound repair. It is later replaced by the tougher type I collagen.90
Elastin is a structural protein present in tendons in amounts of less than 1%.35,136 Tissues with greater amounts of elastin usually demonstrate greater degrees of flexibility. Elastin assists collagen in the recovery of tissues after stress.
Stress and Strain
Stress or load is given in units of force/area, where the units may be pounds per square inch or Newtons per square centimeter.96 Therefore stress is directly related to the magnitude of force and inversely related to the unit area, but is independent of the amount of a material.97 The complementary measure related to stress is strain or deformation. Strain is usually dimensionless, since the units of measure cancel each other out, but units are often provided (e.g., inches/inch) to give a perspective of scale applied to the loads.96
The relation of stress and strain is dependent on several factors. These include the material properties used, the magnitude of the stresses, and the rate of stress application. Subsequently, the graphical representation of stress and strain is different for each type of material discussed. This representation is known as the stress-strain or load-deformation curve.92 Figure 3-2 demonstrates the various regions within the stress-strain curve, with each region demonstrating a biomechanical property of a tissue.
The toe region represents how a slightly pulled tissue (i.e., a ligament) produces only a small amount of tension within the tissue; it indicates that the collagen fibers within the tissue must first be pulled tight before a stretch can be induced. This minimal amount of tension simply results in the slack of the tissue being taken up with no stretch being encountered. The elastic region represents a linear change in strain, which occurs if the tissue continues to be pulled at higher stress levels. A good example of this linear relation is similar to the model of a stretched rubber band. The greater the load on the rubber band, the more the rubber band stretches. So, as the tension on the rubber band is removed, the band shortens, nearing its original length. Given this behavior, it is referred to as the elastic zone. The amount of stretch (strain) applied to the tissue in this zone is generally experienced during many body movements. Note that the slope (the angle of the curve) in this zone is indicative of the relative stiffness of the tissue. Stiffness is defined as the change in force per unit change in length.41 As such, the stiffer the tissue, the steeper the slope. So tissues such as ligaments will only change length at higher levels of stress compared with tissues of less stiffness, such as loose connective tissue.
The upper level of the elastic region marks a transition from the linear slope to one where the slope begins to flatten. This is called the plastic region and is a point where an increasing level of stress on the tissue results in proportionately increased changes in tissue length, probably due to microscopic failure of the tissue. This is termed the plastic zone because of the tissue damage resulting in permanent deformation (plastic deformation). Unlike the elastic region, the plastic energy is not recoverable in its entirety when the load is removed; additionally, there is a change in its resting length. Continued stretch in the plastic region would result in additional deformation of the tissue and would occur until it reached its initial point of failure. The toe region can include strains up to 3%; the elastic region, from 6% to 10%; and the plastic region, from 10% to 15%.41,112
Viscoelasticity
All connective tissue exhibits the property of viscoelasticity, which is simply a combination of the behavior of the properties of elasticity and viscosity.73,76 Elasticity refers to a material’s ability to return to its original state following strain or deformation (i.e., change in length or shape) after a removal of the stress or load. This mutable change is termed elastic deformation and is similar to the changes that occur in a rubber band under high rates of strain. The rubber band rapidly conforms to a new length and is able to return to its original resting length when the stress is removed. However, the rubber band breaks if the degree of stress exceeds the strain capabilities (Fig. 3-3). Viscosity refers to a material’s ability to resist a change in form or to dampen shearing forces. Tissues exhibiting viscosity have time-dependent and rate-dependent properties when forces are applied to them.
The rate at which tissues are stretched has a profound effect on the degree or percent of strain. As mentioned, tensile (distractive) or compressive forces will produce deformation on viscoelastic materials, but will allow return to their original state after removal of the force. Given normal conditions, however, viscoelastic materials do not immediately return to their original state. Viscoelastic materials, unlike pure elastic materials, have time-dependent properties. Slower rates of stress produce greater amounts of strain or elongation, whereas faster rates of stretch produce much smaller amounts of elongation.29,35,119 As such, they are sensitive to the applied force duration. Tissues gradually lengthen when they are subjected to constant or repeated stress of long duration.
So a viscoelastic material subjected to either a constant compressive or tensile load will initially respond by rapidly deforming; it continues to deform over a finite length of time even if the load remains constant. This deformation of the tissue will continue until a state of equilibrium is reached when the load is balanced. This is called the creep phenomenon (Fig. 3-4),76 which simply means the gradual increase in tissue length that occurs when maintaining a constant stress (or force). For example, if one uses a constant force against the muscle with slow and passive stretching, the muscle will eventually elongate. However, the tissue does not return to its original length immediately when unloaded because of the collagen’s viscous property.73 Essentially, the longer the duration of the applied force, the greater the deformation or stretching of the tissue.
The loading and unloading of tissue is influenced by its viscoelastic properties. This loading and unloading is quantified by measuring the hysteresis area (Fig. 3-5). The loading (solid line) and unloading (dashed line) phases represent a measurement of the stress and strain that is applied to a tissue and then released. The hysteresis area lies between the two lines and represents the amount of energy dissipated in the loading and unloading process.41,73
The ability of tissues to recover after stress is extremely important in relation to flexibility. Woo and colleagues136 have shown that increasing the levels of stress produces an increase in collagen within ligaments and tendons, whereas reducing the levels of stress causes weakening in connective tissues. Recovery is the ability of tissues to return to their previous resting state. However, it does not imply that permanent elongation or microscopic damage has not occurred. Plastic deformation is force dependent under slow rates of stress and is used to describe permanent change in a tissue. For example, when a low degree of stress is applied to a plastic spoon, the spoon slowly deforms to a new shape. The spoon breaks if the stress is applied too fast (Fig. 3-6). Lehman and colleagues74 and Warren and co-workers126 have demonstrated that recovery of the tissue’s resting length had occurred after microscopic failure had begun.
Along with stress and the rate of stress applied to tissues, temperature also affects connective tissue extensibility as well as the rate of creep. High temperatures in the range of 37° C (98.6° F) to 40° C (104° F) affect the viscoelastic properties of connective tissue and increase the rate of creep.29,73 The higher the temperature (approximately 45° C [113° F] is the therapeutic upper limit), the greater the degree of elongation with stress before tissue failure.108 Because connective tissue’s viscoelastic and plastic changes occur at higher temperatures, there is less microscopic damage under stress at these temperatures. Studies by Warren and colleagues127 have demonstrated that a temperature of 45° C is needed to reduce tissue damage during strains of 2.6% or less. So to stretch out a connective tissue structure, one should heat it and use a large load over a long period of time to produce creep.96 Low temperatures decrease the rate of creep.
Muscle or contractile tissue responds to stretch by elastic and plastic deformation properties in ways similar to connective tissue. Obviously the contractile properties of muscle allow for the greatest degree of freedom of movement around a joint. Although connective tissue is considered a passive resistant to joint motion, muscle tissue is considered an active restraint to joint motion by virtue of its elastic and contractile elements. Active exercise (muscular contractions) affects intramuscular temperature. Increases to approximately 39° C are observed in exercised muscle.6 Commonly used passive thermal agents that increase tissue temperature are moist heat and ultrasound. The judicious use of active exercise and passive thermal agents before and during stretching programs enhances the effectiveness of the prescribed program.
FLEXIBILITY
Kisner and Colby64 define flexibility as the ability of a muscle to relax and yield to a stretch force. Others have defined flexibility as the ability to move muscles and joints through a full ROM.12,102 In essence, flexibility refers to the degree of normal ROM available. Therefore, flexibility can refer to various measurable components of joint motion. Muscles, tendons, ligaments, skin, joint capsule, and bone geometry all influence the degree of movement in joints. For example, a muscle can stretch or elongate, creating a measurable effect on the joint or joints upon which it acts. If a muscle becomes damaged by trauma or disease or becomes shortened because of immobilization, its ability to stretch and allow freedom of joint motion is affected. Flexibility will diminish over time if tissues are not stretched or exercised using regular and proper stretching regimens.2 As such, the goal of any flexibility program would be to improve or maintain ROM at all joints.
Different classifications of flexibility currently exist, depending on how the tissue is stretched. For example, static flexibility occurs as a result of static stretching, whereas dynamic flexibility relates to moving through a ROM with normal or rapid velocity.2 However, evidence does not support the existence of flexibility as a single general characteristic of the body. Instead, it is specific to particular joints, joint actions, or movements and is highly variable among different individuals.53 An understanding of the properties and components of various connective tissues is fundamental in delivering various stretching and flexibility regimens.
Measuring Flexibility
It is important to assess overall flexibility by measuring ROM at specific joints, because no one composite test provides an index of an individual’s flexibility characteristics.53,54 Subsequently, some measurements of overall flexibility are somewhat difficult, since they involve a complexity of movements over several joints (e.g., sit and reach test).
Measuring joint ROM is accomplished by using standard goniometric instruments. The measuring device most commonly used to measure ROM is the universal goniometer (Fig. 3-7), which is a protractor with degree measurements. The goniometer arms are placed along the proximal and distal components of a joint with the axis centered over the joint, which are then moved in accordance with the body part being measured. The goniometer can be used to measure joint position and ROM at almost all joints of the body.95 Other types of goniometers used less frequently in the clinical setting are the inclinometer, the pendulum goniometer, and the fluid goniometer.
Consistency in measurement is crucial; therefore it is important to use the same type of goniometer for a specific patient each time that patient is measured. Because different goniometers may provide slightly different results, they should not be interchangeable in their use in the clinical setting. For example, when using an inclinometer as the measuring device, it should be used for all future measurements for that patient to ensure consistency.96 For documentation purposes, most authorities recommend using goniometry rather than visual estimates because of its increased accuracy and reliability of measurement.128,137
Joint stability differs from joint ROM in that the ligaments and surface geometry of joint articulations dictate static joint integrity (stability). A patient may demonstrate limited ROM in knee flexion and extension (by goniometry); however, anterior and posterior joint mobility may be excessive and unstable (Fig. 3-8). On the other hand, a patient may demonstrate normal joint ROM, yet when tested statically the joint may be very stable, tight, and unyielding to pressure.
The sit and reach test (Fig. 3-9, A-B), standing toe touch for back and hamstring flexibility (Fig. 3-9, C), seated hip external rotation test (Fig. 3-9, D), and standing knee recurvatum test generally are less specific flexibility tests. These tests and others are used to provide very general assessment of multijoint flexibility. Such tests also can be used as stretching techniques to improve limitations in movement. However, objective clinical documentation of joint ROM is made by joint goniometry.
Factors Affecting Flexibility
In addition to muscles, tendons, and their surrounding fascia, other structures, such as bone, fat, connective tissue lesions, skin, and postural problems, may all lead to flexibility and joint ROM limitations.5 Other factors that may affect flexibility are age and gender.14,25
STRETCHING
Stretching involves elongating the muscles and tendons to the end of the available ROM. As such, applying a tensile force to a muscle results in a transient deformation, which elongates the musculotendinous unit, resulting in a stretch.2,40 Given that the mechanical behavior of connective tissue is primarily influenced by the amount of collagen available,73,119 the amount of stretching that takes place is dependent on the type of connective tissue present (i.e., skin, fascia, ligaments, tendons, joint capsules, and muscle fascia).
Although gradually increasing flexibility to increase ROM is the main goal, other adaptations occur from a regular stretching program. For example, research has shown that as a result of training, the stretch reflex may be reset to a different level.133,134 Several types of stretching exercises have been detailed in the literature and will be described in this section.
Stretching Principles
Stretching is effective primarily because of its mechanical and neurophysiologic effects.69,119 As mentioned, the muscle-tendon unit responds viscoelastically during stretching. However, some stretching exercises are based on the neural inhibition of the muscle undergoing stretch as well. In this case, a decreased reflex activity would result in reduced resistance to stretch, resulting in further gains of joint ROM. Most likely, both mechanisms are responsible.
It is important to note that stiffness relates to a tissue’s ability to resist stretch and indicates the amount of deformation proportional to the load applied.81 So, the stiffer the tissue, the less compliance it has and the less likely it is to stretch; conversely, less stiffness means greater compliance. It stands to reason then that flexibility training is designed to decrease the stiffness of the muscle-tendon unit.69,119 Furthermore, a rapidly applied stretch results in a greater resistance to that stretch.
Both mechanical and neurophysiologic components are inherent within muscular flexibility.43,50,105,118,119 However, some researchers believe that the ability of stretching to produce greater flexibility is primarily a result of the viscoelastic nature of muscle and connective tissue.84,119 As such, the most resistance to stretching probably is due to the connective tissue framework and sheathing from within and around the muscle and not the muscle itself (since the muscle itself can be stretched to 150% of its resting length); this includes the epimysium, perimysium, and endomysium and may even include the sarcolemma.107,109,116,117
On the other hand, many researchers suggest that the immediate result of stretching is attributed to neurophysiologic phenomena.69 They categorize these phenomena as either a stretch tolerance or active contractile responses and claim that the limiting factor during stretching is the muscular resistance secondary to reflex activity. A stretch tolerance simply means an accommodation to the discomfort of stretching over time. With this philosophy, the aim of stretching is to inhibit the reflex activity, subsequently decreasing the resistance and improving ROM. Several other researchers agree and recommend certain types of stretching for its reduction in reflex activity.3,43,50 Muscle spindles and Golgi tendon organs are the mechanoreceptors responsible for the contractile responses (Fig 3-10).
Warm-up
Warm-up is necessary to help prepare the tissue for activity. Stretching alone before exercise is not recommended by most researchers and health professionals.65,66,111,124 As such, the purpose of warm-up exercises, including stretching, is to prepare the body for the stresses it will encounter during an activity or sport and is necessary for increasing the core body temperature. Heat is produced with muscle contraction, thereby increasing the intramuscular temperature.23 ROM increases as a result of warmed tissue.107 A warmed muscle will be able to contract more forcefully and relax more quickly,15 thereby enhancing work production for those muscles used.16 In training, a general body warm-up is needed first. The beneficial effects of a warm-up before strenuous activities include the following:
Blood flow to working muscles is increased.
Temperature in working muscles is increased.
Cardiovascular response to sudden, dynamic exercise is improved.
Breakdown of oxyhemoglobin for the delivery of oxygen to the working muscles is increased.
With warm-up, the risk of connective tissue and contractile tissue damage is reduced. Warm-up protocols usually last from 10 to 25 minutes or more and may vary somewhat, depending on the nature of the activity or event.8 The warm-up should be intense enough to cause an increase in body temperature, but not so intense as to cause fatigue. So one should taper the warm-up 5 to 10 minutes before the actual event.3 It is clinically assumed, of course, that a more compliant muscle can be stretched further and is therefore less susceptible to injury.48
However, some think that the warm-up period may not be the best time to stretch for increasing ROM, primarily because of increased tissue stiffness. Since the concept of stretching to prevent injury has come under question, benefits of stretching before activity may be incorrect. Activity of gradually increasing intensity (dynamic stretching) may be more appropriate than static stretching as a warm-up activity.96 Some researchers have examined the combination of stretching and active warm-up and have shown that the decrease in stiffness mainly results from increased muscle temperature and not stretching.85,104
Increasing intramuscular temperature to help increase ROM may also be achieved through external means.110 Henricson and colleagues57 reported on results that followed the application of heat to the hip. Although heat alone did not improve hip ROM, stretching without heat did increase hip ROM, and stretching with heat combined gave the greatest increase in ROM, maintaining it for 30 minutes. These results are consistent with others,62,74,127 who report that collagen extensibility increases and musculotendinous stiffness decreases with heat. Bear in mind, however, that most authors recommend using exercise as the primary way of increasing intramuscular temperature.96 It has not been definitively shown whether a general warm-up serves to improve sports performance.17,18,21,46
Stretching Techniques
In discussion of flexibility and associated stretching programs, the stretching of nonpathologic muscle must be separated from stretching noncontractile connective tissue. Improving muscle extensibility in nonpathologic conditions and in adaptive muscle shortening after injury or immobilization requires a complement of active exercise techniques and thermal agents. Types of stretching exercises are static stretching (active and passive), ballistic stretching, dynamic stretching, and proprioceptive neuromuscular facilitation (PNF) techniques (contract-relax, contract-relax with agonist contraction, and hold-relax). Research has shown that all four techniques have been shown to increase flexibility.31,56,61,80,82,105 Essential to a successful stretching program for improving flexibility is the proper execution of the exercises.
Static stretching
The most common form of stretching exercise that is used to safely increase the ROM in a joint is static stretching. This form of stretching allows one to sustain a controlled stretch by placing a muscle in a fully elongated position and holding that position for a period of time (Fig. 3-11
[/not-level-membership-for-orthopaedics-category]
