Problem 15 Flank pain in a 60-year-old man
Now that the patient’s condition has stabilized some further investigations can be considered.
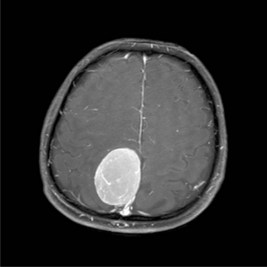
A non-contrast CT scan is performed and two representative slices are shown in Figure 15.1A, B.


He is readmitted 2 weeks later for a ureteroscopy after his urine is confirmed to be sterile.

Answers
• Further details about the pain are required. What is the location, is it colicky in nature, what is the severity, does it radiate anywhere and are there any aggravating or relieving factors?
• Are there any other associated symptoms, in particular symptoms of the gastrointestinal (vomiting, diarrhoea) and urinary tracts (dysuria and haematuria)?
• It is important to ascertain relevant medical history, including diabetes, gout, previous surgery and any history of renal stones or gastrointestinal disease. Current medications and allergies should be noted.
A.8 A combination of anti-inflammatories and opioids is effective for renal colic.
• Size – smaller stones are more likely to pass. Approximately 75% of stones with diameter < 4 mm pass spontaneously, and only 35% with diameter > 7 mm.
• Location – there are three anatomical locations where the ureter tends to narrow: at the pelviureteric junction (PUJ), where the ureter crosses the iliac artery, and at the vesicoureteric junction (VUJ). A more distal location of the stone predicts a higher rate of spontaneous passage.
• Duration and grade of obstruction – prolonged symptoms and signs of high-grade obstruction (hydronephrosis, perinephric stranding, extravasation of urine) make spontaneous passage very unlikely.
• Fever, urinary infection, deteriorating renal function and pain that is difficult to control are indications to intervene early to relieve the obstruction. This can be performed by a ureteric stent or percutaneous nephrostomy tube.
• All these indications relate to the medical condition of the patient, and are not related to stone size or position.
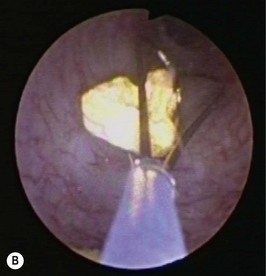
A.11 These are ureteroscopic photographs demonstrating Figure 15.1A after (1) the ureteric stone during LASER lithotripsy, and Figure 15.1B basket extraction of stone fragments.
Revision Points