Firearm and Arrow Injuries/Fishhook Injury
Firearm Injury
Treatment
1. Follow the basic principles of trauma care and resuscitation concerning airway, breathing, circulation, control of bleeding, immobilization of the spine and fractured extremities, wound care, and stabilization of the patient for transport (see Chapter 12).
2. Remove the weapon from the vicinity where you are giving medical care. Remove the ammunition, and leave open the firing chamber.
3. Perform endotracheal intubation as soon as possible if the patient has a neck wound and expanding hematoma. If endotracheal intubation is not possible and the airway becomes obstructed, perform a cricothyrotomy (see Chapters 10 and 12).
4. Provide immediate relief of a tension pneumothorax with a needle or tube thoracostomy, or occlusion of a sucking chest wound with petrolatum-impregnated gauze (see Chapter 15).
5. Control external bleeding by direct pressure and compression wraps.
a. If bleeding from an extremity cannot be stopped by direct pressure, apply a tourniquet (see Chapter 12).
b. Hemostatic agents are potentially useful products to stop bleeding that cannot be controlled by direct pressure or a tourniquet. When poured or packed into a wound, the granules or gauze combine with blood to induce a robust gel-like clot. Combat Gauze, which is kaolin-impregnated Kerlix gauze (the active agent is aluminum silicate), is the hemostatic dressing issued to the U.S. military for combat use.
6. Treat for shock, and take measures to prevent hypothermia (see Chapter 13).
7. Do not perform wide debridement of normal-appearing tissue.
8. Monitor the neurovascular status of an extremity wound; keep the extremity elevated to minimize swelling.
9. Remember that the path of the bullet cannot reliably be determined by connecting the suspected entrance and exit wounds.
10. Ultimate removal of the bullet or bullet fragments is not necessary unless the bullet is intravascular, intra-articular, or in contact with nervous tissue. It is certainly not necessary in the field.
11. Use forceps to remove from the skin any shotgun pellets that have minimal penetration.
12. For gunpowder burns, remove as much of the powder residue as possible with a scrub brush because gunpowder will tattoo the skin if left in place.
13. Aggressive intravenous (IV) fluid administration to maintain or reach normotension is discouraged in patients with penetrating injury in the field. Allowing the blood pressure to remain in the life-sustaining hypotensive range (systolic blood pressure >100 mmHg) may prevent disruption of clots and dilution of clotting factors. Follow the most recent recommendations for fluid resuscitation for trauma-induced hemorrhage.
14. Administer broad-spectrum antibiotics that provide both aerobic and anaerobic coverage (e.g., cefotetan adult dose 2 g IV q12h or amoxicillin/clavulanate 875 mg/125 mg PO q8h if IV is not available).
Arrow or Spear Injury
Treatment
1. Follow the same treatment principles of trauma care and resuscitation as for a firearm injury.
2. Irrigate lacerations inflicted by arrows or spears, and remove any foreign material. Close the wound primarily following the guidelines in Chapter 20.
3. The piercing arrow or spear lodged in a patient should be physically stabilized so that it remains as motionless as possible, and the object should be left in place during transport. Attempts to remove the weapon by pulling it out or pushing it through the wound may cause further injury. Cut the shaft, and leave about 8 to 10 cm (3 to 4 inches) protruding from the wound to make transport easier, if this can be accomplished with minimal disturbance. A large pair of paramedic-type shears can often cut through an arrow shaft.
4. Bolster and prop the portion of the weapon that remains in the wound with a stack of gauze pads or cloth and tape.
5. Administer broad-spectrum antibiotics that provide both aerobic and anaerobic coverage (e.g., cefotetan adult dose 2 g IV q12h or amoxicillin/clavulanate 875 mg/125 mg PO q8h if IV is not available).
6. Transfer the patient as rapidly as possible to a medical care facility for removal of the arrow or spear under controlled conditions.
Fishhook Injury
Treatment
1. Clean the skin surrounding the entry point with an antiseptic or with soap and water.
2. Remove the hook using one of the following techniques:
a. Pass a string or shoelace through and around the bend of the hook; the hook can then be yanked from the skin while the shank of the hook is pressed toward the skin surface to disengage the barb (Fig. 19-1). Wear eye protection, and be certain that no one is in striking range of a flying hook.
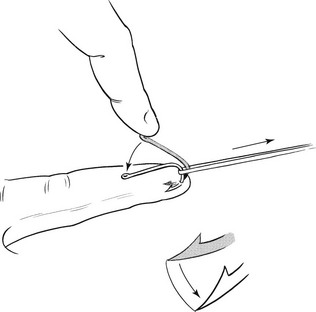
FIGURE 19-1 Fishhook removal.
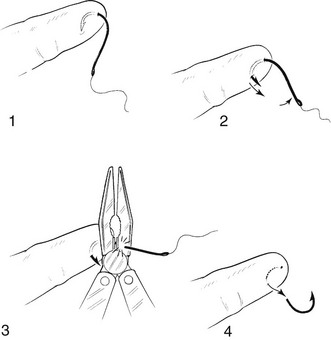
b. With a steady, firm motion, push the hook through the skin so that the barb completely appears. Cut off the barb or the shaft, and pull the remainder of the hook back out of the skin (Fig. 19-2). When cutting off the barb, take care to wear eye protection and look away during cutting.
3. Irrigate the wound with saline solution or water. Inspect the wound daily for signs of infection.
4. For a fishhook embedded in the eye, leave it in place and secure it with tape. Cover the eye with a sufficiently deep eye shield or cup, and transport the patient to an ophthalmologist for definitive care.