Chapter 13 Fever
9 What is “fever phobia”?
Corneli HM. Beyond the fear of fever. Clin Ped Emerg Med 1:94–101, 2000.
Schmitt BD: Fever phobia: Misconceptions of parents about fevers. Am J Dis Child 134:176–181, 1980.
10 What are the normal increases in heart rate and respiratory rate with each degree rise in body temperature?
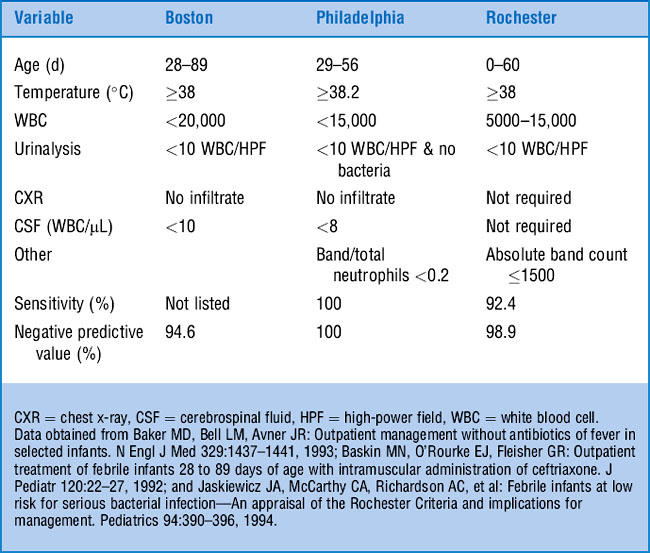
26 What are low-risk criteria for the management of febrile infants?
In an attempt to avoid routine hospitalization of all febrile young infants, many investigators have sought to devise clinical and laboratory criteria that would identify a subset of febrile infants at “low risk” of having bacterial disease as a cause of their fever. Three major prospective studies have established somewhat different low-risk criteria (Table 13-1).
28 Do all febrile infants need a sepsis workup and admission?
Although there is no absolute consensus, most agree that febrile infants less than 1 month of age require an evaluation for sepsis. Many also feel that the same evaluation applies to infants 1–2 months old. However, some clinicians withhold a lumbar puncture in well-appearing febrile infants. Infants younger than 1 month and those infants at high risk should be hospitalized pending culture results. Infants 1–2 months old who are at low risk (see Table 13-1) for serious bacterial illness may be managed as outpatients if follow-up is assured.
29 Do young febrile infants with respiratory syncytial virus (RSV) bronchiolitis need a sepsis workup?
KEY POINTS: THE FEBRILE INFANT
1 In febrile infants less than 28 days old, the risk of serious bacterial illness is substantial (about 10%) and is not altered by the presence of RSV infection.
2 Urinary tract infection is the most common bacterial infection in febrile infants less than 2 months old.
3 For well-appearing febrile infants 4–8 weeks old, a variety of testing and management strategies are available.
35 Is the peripheral white blood cell count a helpful screen for bacteremia in otherwise healthy febrile children?
36 Should the decision on whether to perform a lumbar puncture on a febrile child be guided by the height of the fever or the peripheral white blood cell count?
41 What is the difference among intermittent fever, spiking fever, remittent fever, sustained fever, and relapsing fever?
43 How often does FUO have no diagnosis or resolve spontaneously?
Almost 25% of children with FUO are either undiagnosed or have spontaneous resolution.
45 How do you decrease body temperature in children with heatstroke?
Management of heatstroke begins with aggressive attempts at cooling, such as ice packs, fanning, ice water immersions, and, occasionally, cool IV fluids, until the core temperature drops below 39°C. Avoid antipyretics and alcohol sponge baths (see question 15). Further management includes airway and cardiovascular support, IV rehydration, and pressor support if necessary.
46 What kind of fever is associated with bizarre movements in response to disco music?
1 eMedicine Health http://www.emedicinehealth.com/articles/10035-1.asp
2 eMedicine Health http://www.emedicine.com/emerg/topic377.htm
3 University of Chicago Priztker School of Medicine, Pediatrics Clerkship http://pedclerk.bsd.uchicago.edu/evaluationoffever.html
4 National Guideline Clearinghouse http://www.guideline.gov/summary/summary.aspx?ss=15&doc_id=4620&nbr=3401
