40 Femoral Nerve Block
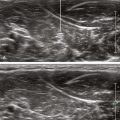
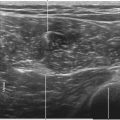
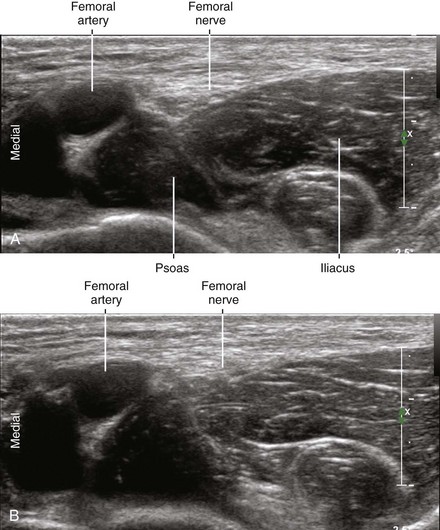
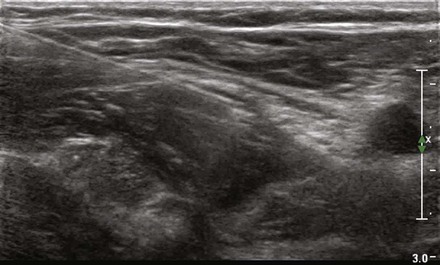
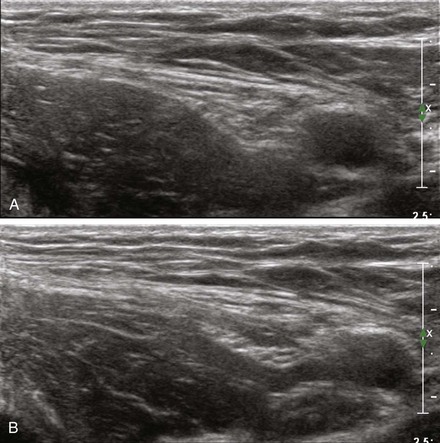
The normal femoral nerve is oval or triangular in cross section, with dimensions of about 3 mm in anteroposterior diameter and 10 mm in mediolateral diameter in the inguinal region.1 The femoral nerve usually lies lateral to the femoral artery but can contact or lie underneath the femoral artery in 15% of cases. In about one third of individuals, the femoral nerve is triangular in the suprainguinal region on short-axis scans.
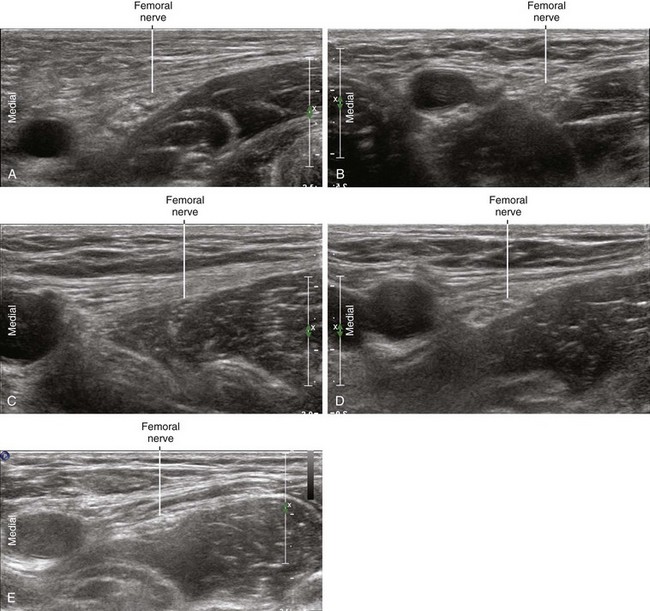
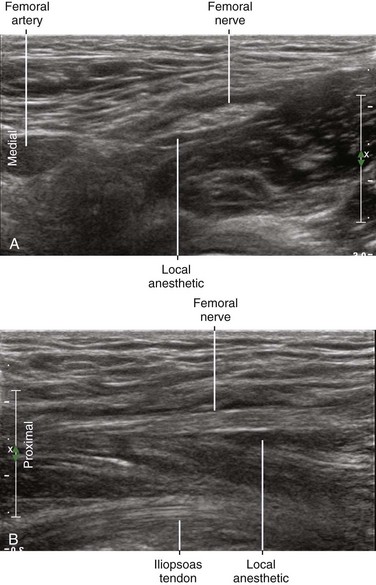
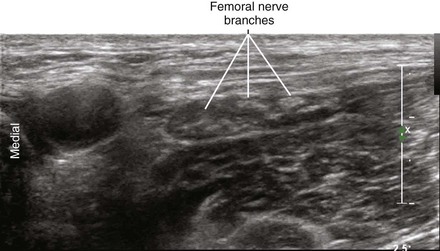
The femoral nerve is covered by echogenic subcutaneous tissue and fascia. The nerve lies on the hypoechoic iliopsoas muscle, which has a characteristic mediolateral inclination. This incline positions the lateral side of the nerve slightly closer to the skin surface. At this interface of bright fascia and dark muscle, the nerve can be difficult to visualize. The best nerve visibility is proximal to the inguinal crease before the femoral nerve and femoral artery divide into smaller branches distally. In this proximal location, the femoral nerve puts a small dent in the surface of the iliopsoas muscle. This occurs because the femoral nerve usually lies in the groove between the iliacus (lateral) and psoas (medial) components of the muscle. The tilt of the transducer strongly influences femoral nerve visibility owing to anisotropic effects.2 With ultrasound guidance it may be possible to perform more proximal drug injections and therefore more complete resultant femoral nerve blocks.
Suggested Technique
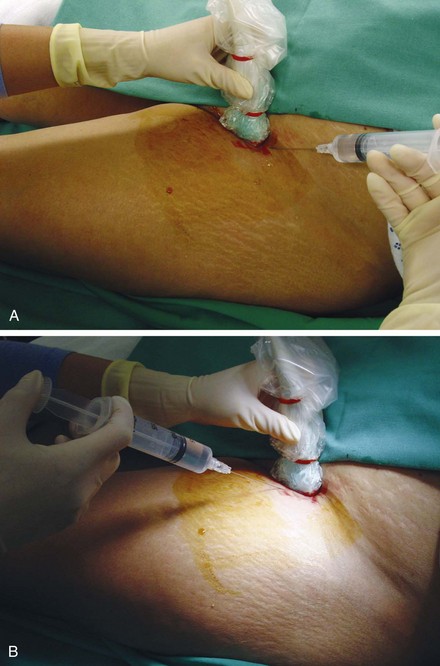
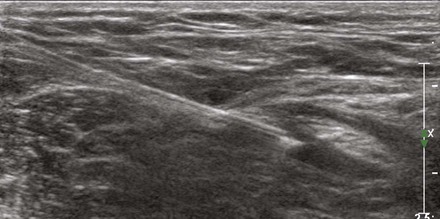
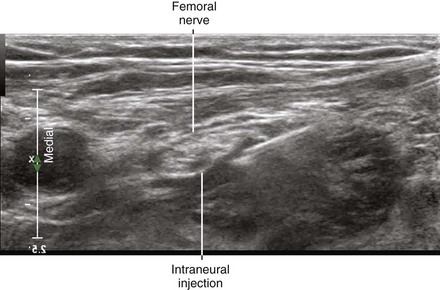
Femoral nerve block is performed in the supine position with the nerve in short-axis view. The lateral corner of the nerve is targeted to avoid the femoral vessels and to make the injection closest to the skin surface. Both out-of-plane (from distal to proximal) and in-plane (from lateral to medial) approaches can be used. It is critical that the needle tip be positioned between the fascia iliaca and iliopsoas muscle.3 It is not important to position the needle tip immediately adjacent to the nerve.
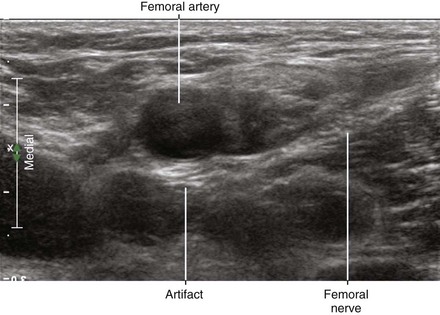
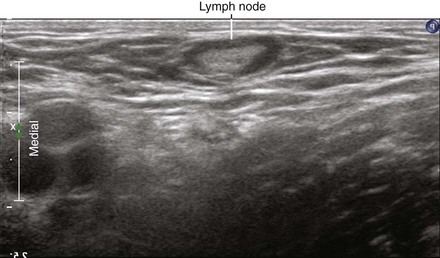
Posterior acoustic enhancement occurs deep to the femoral artery.4 This artifact should not be confused with the femoral nerve. The femoral nerve and iliopsoas tendon can be distinguished because the iliopsoas tendon normally lies deep within the iliopsoas muscle.
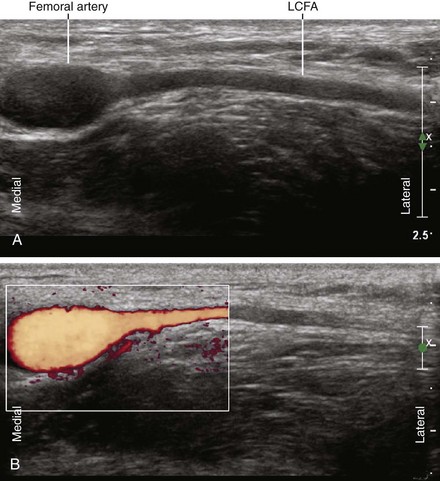
Many institutions have found the out-of-plane approach to be very safe and effective.5 However, the operator must be cognizant of the unimaged needle path. Branches of the femoral artery may lie within the unimaged needle path short of the scan plane.6 Scanning before needle placement can be advantageous.
The incidence of vascular puncture rates with nerve stimulation–guided femoral nerve catheters is about 6%.7 Ultrasound guidance likely reduces that incidence. Puncture of the inguinal vessels can result in blood tracking into the retroperitoneum, even if the puncture occurs distal to the inguinal ligament.8
Key Points
| Femoral Nerve Block | The Essentials |
|---|---|
| Anatomy | The FN lies lateral to the FA on the surface of the iliopsoas muscle. |
| The FN lies in the groove between the iliacus and psoas muscles. | |
| The LCFA can lie over the FN. | |
| The FN is about 3 by 10 mm in diameter. | |
| Image orientation | The iliopsoas muscle has an inclined surface from lateral to medial. |
| Positioning | Supine with leg slightly abducted |
| Some pannus retraction may be necessary | |
| Operator | Standing on the side of the patient |
| Display | Across the table |
| Transducer | High-frequency linear, 38- to 50-mm footprint |
| Initial depth setting | 25 to 30 mm |
| Needle | 20 to 21 gauge, 70 mm in length |
| Anatomic location | Begin by scanning with the probe along the inguinal crease. |
| Slide proximally until the common FA and FN are seen in SAX view. | |
| Best FN imaging is usually 1 to 2 cm proximal to the inguinal crease. | |
| Approach | SAX view of the FN, in-plane from the lateral side |
| Place the needle tip through the fascia iliaca at lateral corner of FN. | |
| Inject underneath the FN (between the FN and iliopsoas muscle). | |
| Sonographic assessment | The injection should track along the FN branches (SAX slide). |
| Anatomic variation | Distance of FN from FA is variable |
| Different nerve morphologies (commonly oval or triangular shape) |
FA, Femoral artery; FN, femoral nerve; LCFA, lateral circumflex femoral artery; SAX, short axis.
Clinical Pearls
• Some clinicians advocate an oblique out-of-plane approach to femoral nerve block.9 This approach from the lateral aspect of the thigh allows needle tip placement under the posterior aspect of the nerve. The needle tip punctures the fascia iliaca at the lateral corner of the femoral nerve.
• The iliopsoas tendon lies under the femoral artery and should not be mistaken for the femoral nerve.10
• Transducer location is of paramount importance to femoral nerve visibility. If the transducer is too distal, the femoral nerve and artery will divide.11 This compromises nerve visibility because it is difficult to image small femoral nerve branches, particularly those that branch to the surface, within the echobright subcutaneous tissue (only after injection of anechoic fluid can these branches be seen). If the transducer is too proximal, the nerve and artery will dive away from the transducer on the surface on the iliacus muscle.
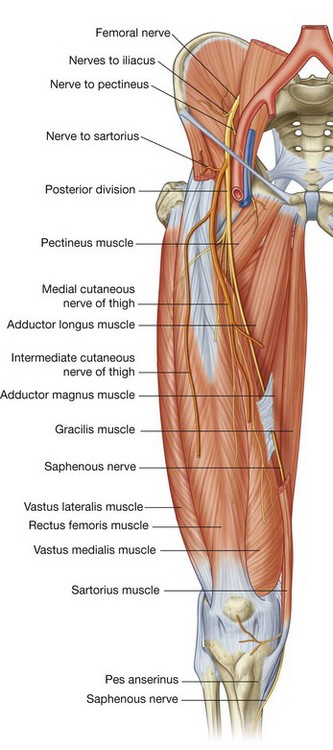
FIGURE 40-1 Course of the femoral nerve.
(From Drake RL, Vogl W, Mitchell AWM. Gray’s anatomy for students. Philadelphia: Churchill Livingstone; 2004.)

1 Gruber H, Peer S, Kovacs P, et al. The ultrasonographic appearance of the femoral nerve and cases of iatrogenic impairment. J Ultrasound Med. 2003;22:163–172.
2 Soong J, Schafhalter-Zoppoth I, Gray AT. The importance of transducer angle to ultrasound visibility of the femoral nerve. Reg Anesth Pain Med. 2005;30:505.
3 Dalens B, Vanneuville G, Tanguy A. Comparison of the fascia iliaca compartment block with the 3-in-1 block in children. Anesth Analg. 1989;69:705–713.
4 Filly RA, Sommer FG, Minton MJ. Characterization of biological fluids by ultrasound and computed tomography. Radiology. 1980;134:167–171.
5 Sites BD, Spence BC, Gallagher JD, et al. Characterizing novice behavior associated with learning ultrasound-guided peripheral regional anesthesia. Reg Anesth Pain Med. 2007;32:107–115.
6 Orebaugh SL. The femoral nerve and its relationship to the lateral circumflex femoral artery. Anesth Analg. 2006;102:1859–1862.
7 Wiegel M, Gottschaldt U, Hennebach R, et al. Complications and adverse effects associated with continuous peripheral nerve blocks in orthopedic patients. Anesth Analg. 2007;104:1578–1582.
8 Spies JB, Berlin L. Complications of femoral artery puncture. AJR Am J Roentgenol. 1998;170:9–11.
9 Fredrickson M. “Oblique” needle-probe alignment to facilitate ultrasound-guided femoral catheter placement. Reg Anesth Pain Med. 2008;33:383–384.
10 Mulroy RD. The iliopsoas muscle complex: iliacus muscle, psoas tendon release. Clin Orthop. 1965;38:81–85.
11 Muhly WT, Orebaugh SL. Ultrasound evaluation of the anatomy of the vessels in relation to the femoral nerve at the femoral crease. Surg Radiol Anat. 2011;33(6):491–494.