Chapter 13 Female Genital System and Breast
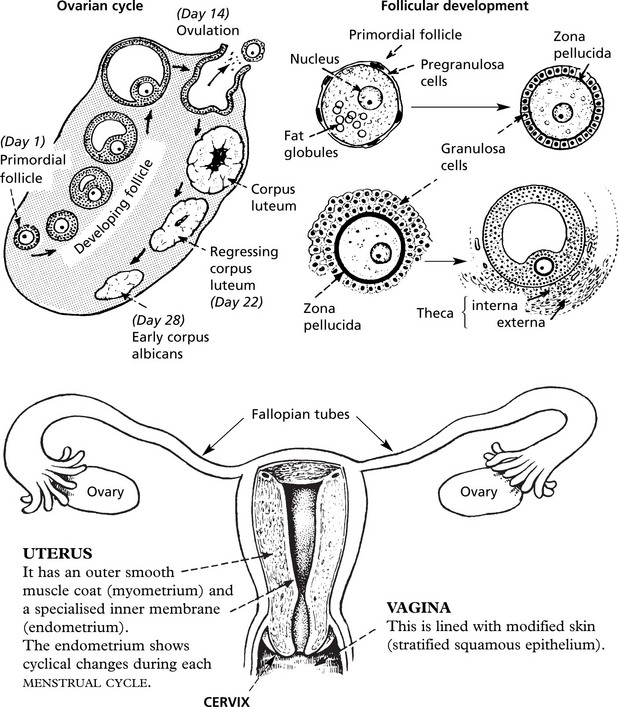
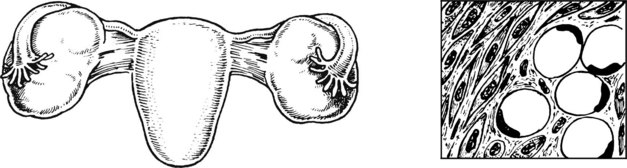
Female Genital Tract – Anatomy and Physiology
The following diagrams summarise normal anatomy and physiology:
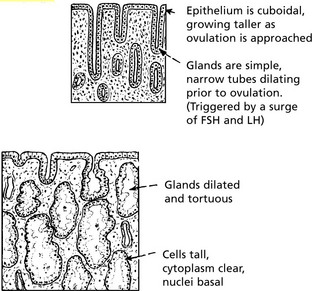
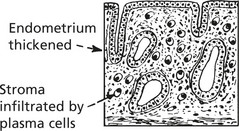
Cyclical Endometrial Changes
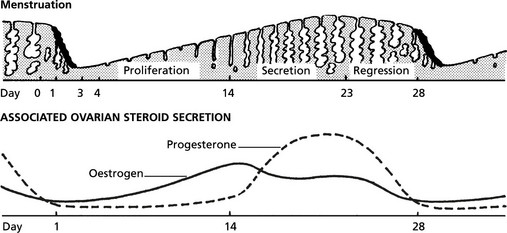
Diseases of the Endometrium
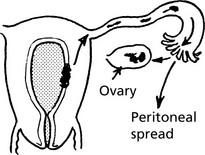
Endometriosis
This consists of deposits of endometrium outside the uterine cavity.
In most cases, the disease is confined to the pelvis and the genital tract.
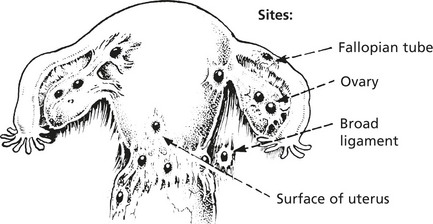
Other sites: Caecum and appendix, bladder, rectum, umbilicus laparotomy scar.

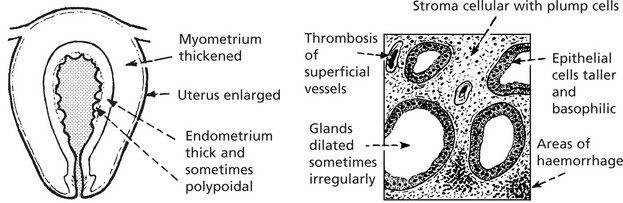
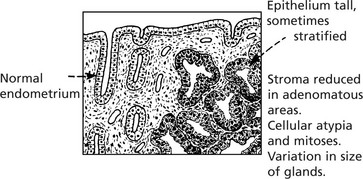
Endometrial Hyperplasia
Endometrial hyperplasia occurs in 3 forms: Simple hyperplasia, complex hyperplasia and atypical hyperplasia. Of these, atypical hyperplasia is most important as it is associated with an increased risk of malignancy. Progressive molecular genetic alterations occur on the pathway to cancer.
Endometrial Carcinoma
This common gynaecological cancer particularly affects postmenopausal patients, who typically present with vaginal bleeding.
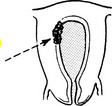
Carcinoma
This growth may form a localised plaque or polyp.

Most growths are well-differentiated adenocarcinomas (endometrioid). These are graded from I – III
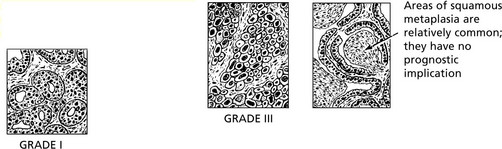
The endometrium possesses no lymphatics and invasion of the myometrium takes place slowly.
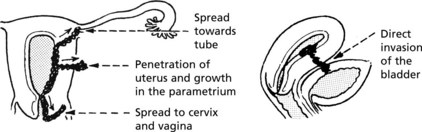
Local extension: this may take place in several directions.
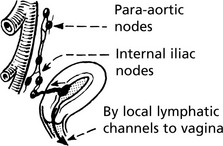
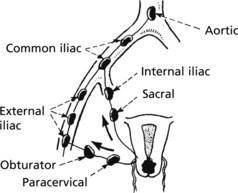
Metastases
Diseases of the Myometrium
Tumours of the myometrium are extremely common.
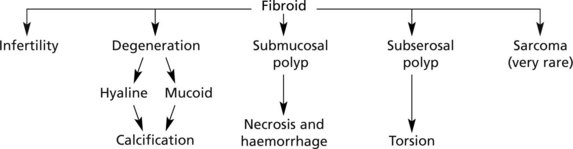
Leiomyoma (Fibroid)
This is a circumscribed growth derived from uterine muscle.
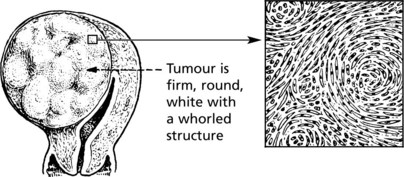
The cells are typical long spindle muscle cells, arranged in interlacing bundles
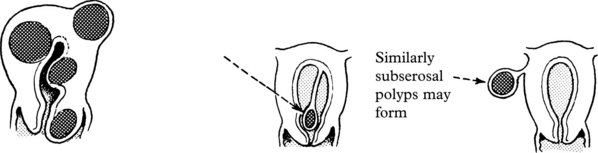
They vary in size from tiny (mm) growths to several cm in diameter and are frequently multiple.
Fibroids may be found in any part of the uterus.
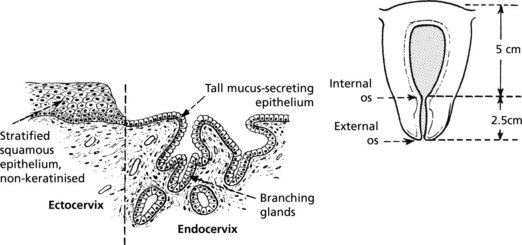
Diseases of the Cervix
The cervix constitutes the lower one third of the uterine body.
It is in two parts: endocervical and ectocervical with different lining epithelium.
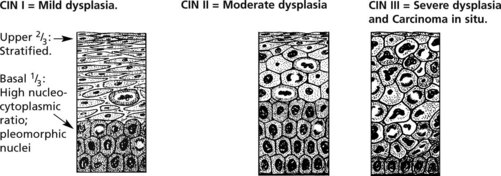
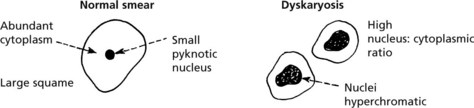
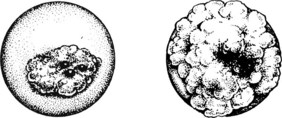
Cervical Intraepithelial Neoplasia (CIN)
The Transformation Zone
From puberty onwards and particularly in pregnancy the squamo-columnar junction presents on the vaginal surface of the external os. This is the area where squamous metaplasia occurs. It is important because cervical squamous carcinoma and its precursor cervical intraepithelial neoplasia (CIN) begin there. Within this metaplastic epithelium, dysplastic changes may develop. They are graded as CIN I, II and III. Later, in some cases, invasive squamous carcinoma develops.

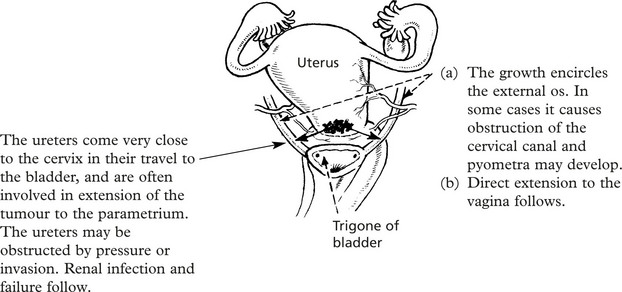
Carcinoma of Cervix
Carcinoma
This is the most common malignant tumour of the female genital tract, even where there is a vigorous screening campaign for early diagnosis and eradication of dysplasia. The tumour is a squamous carcinoma in 90% of cases, and an adenocarcinoma in 10%. Most squamous carcinomas arise at the squamo-columnar junction: most adenocarcinomas arise within the endocervical canal.
The cervix becomes indurated with necrosis and ulceration


Diseases of Vagina and Vulva
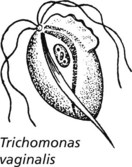
Vaginal discharge is a common complaint especially in parous women. In many cases it is related to chronic cervicitis. There are however a number of inflammatory conditions which arise primarily in the vagina.
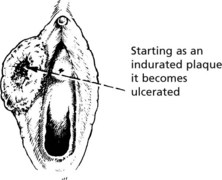
Leukoplakia and Premalignancy
Leukoplakia is a descriptive term meaning white patches. These are common on the vulval and perineal region in almost any chronic inflammatory skin condition due to the local moist conditions, e.g. chronic dermatitis (lichen simplex), fungal infection and lichen sclerosis.
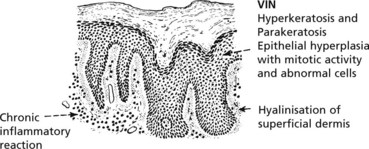
The degree of dysplasia varies, amounting to carcinoma in situ in some cases.
Diseases of the Fallopian Tube
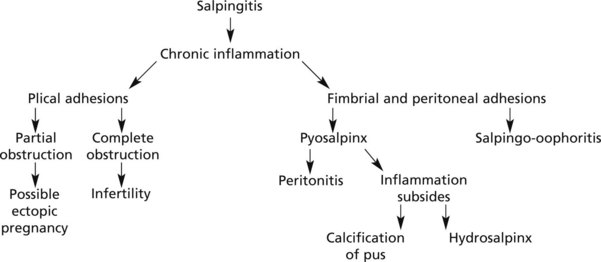
Acute Salpingitis
This is the result of ascending infection from the endometrium: some cases follow abortion and puerperal infection. Chlamydia may cause acute salpingitis.
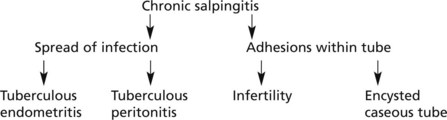
Tuberculous Salpingitis
The complications are those expected of a chronic salpingitis with the added element of caseation.
Diseases of the Ovaries
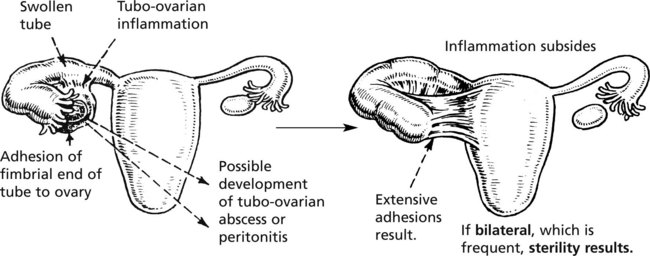
Oophoritis
Inflammation of the ovaries is always secondary to disease of the fallopian tubes or peritoneum. The inflamed fimbrial end of the tube becomes adherent to the ovary and direct spread of infection occurs. Tubo-ovarian inflammation is also associated with the presence of an intra-uterine contraceptive device (see p.496). Important local complications may follow.
The ovary may be similarly involved in tuberculous salpingitis, and caseating lesions can occur.
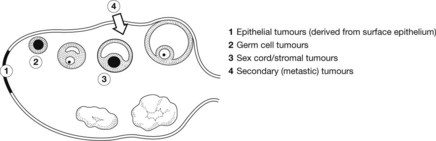
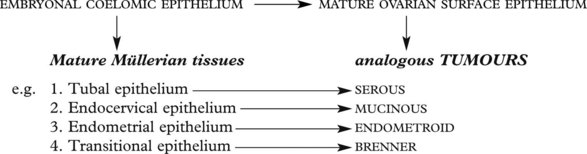
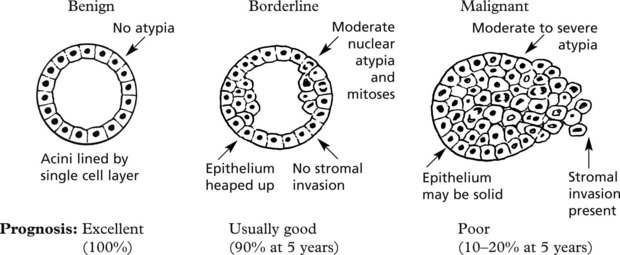
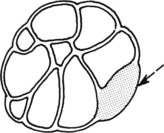
Common Epithelial Ovarian Tumours
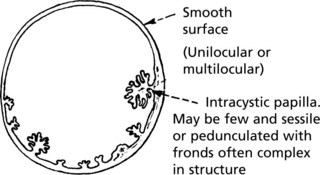
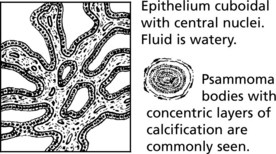
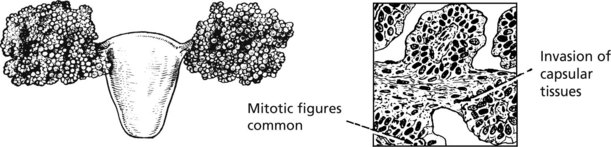
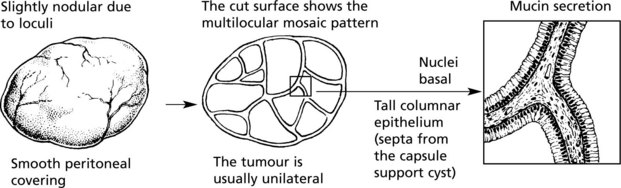
Carcinoma of the Ovary
Complications
Congestion, often infarction due to interruption of blood flow
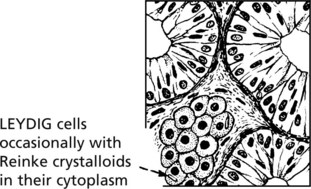
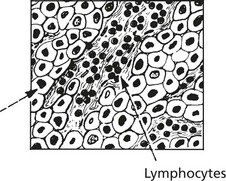
Tumours of the Ovary – Sex Cord Stromal
These may be divided into two broad groups:
Tumours of the Ovary – Germ Cell
Germ Cell Tumours
These arise from primitive germ cells capable of differentiating in many ways. The following diagram indicates the main varieties of tumour produced.

Mature cystic teratoma (dermoid cyst)
This is one of the commonest ovarian tumours and it occurs at all ages.


Very occasionally the squamous epithelium may undergo malignant change.
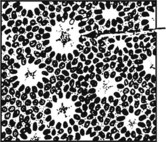
Immature Teratoma
The tumours are predominantly solid and are malignant. They contain immature tissues, typically of primitive nerve tissue and mesenchymal tissue. They may metastasise to the peritoneum where the nerve tissue may differentiate (gliomatosis peritonei).
Chemotherapy has greatly improved the prognosis in these cases.
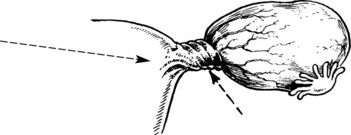
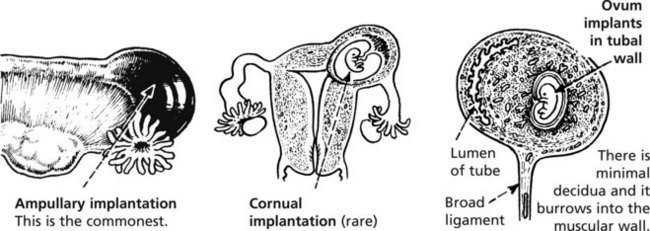
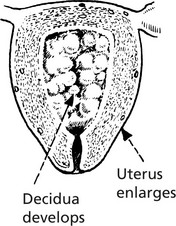
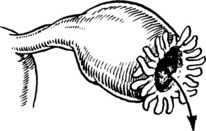
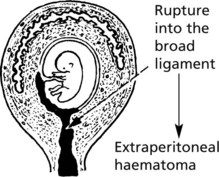
Ectopic Pregnancy
This means implantation of the fertilised ovum outside the uterine cavity usually in the fallopian tube.

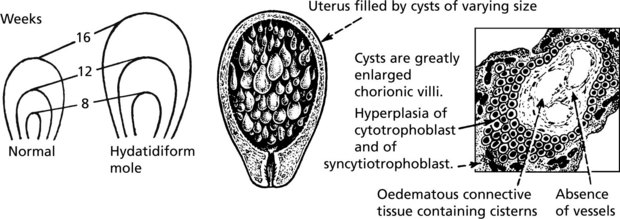
Gestational Trophoblast Disease
This term describes proliferative conditions of placental tissue.
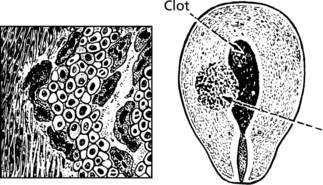
Hydatidiform Mole
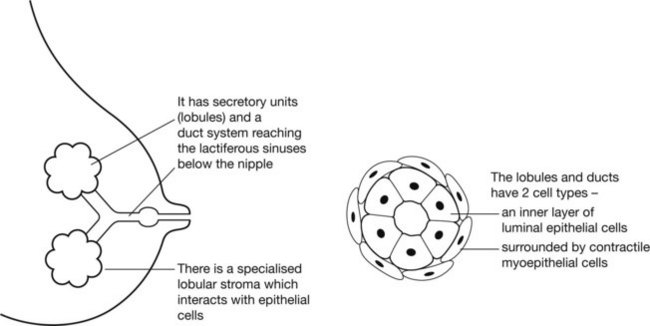
Breast Structure and Function
The breast is a greatly modified sweat gland which has evolved to secrete nourishment to infants.
Benign Diseases of the Breast
Acute infection is an occasional complication of lactation.
Chronic infection e.g. tuberculosis is very uncommon.
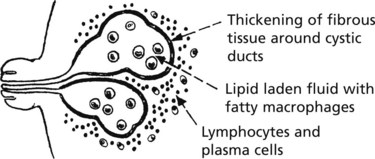
Duct ectasia (plasma cell mastitis)
This chronic inflammatory reaction is associated with ectasia of the ducts (cystic dilatation).
Fibrocystic Change
This change presents as a lump or lumpiness of the breast in pre-menopausal women.
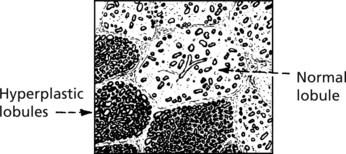

Uniform proliferation of acinar epithelium without acinar expansion.
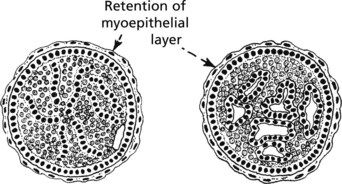
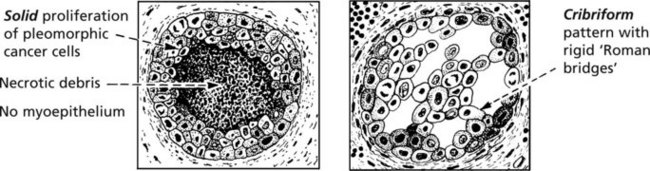
Benign Breast Tumours and in situ Carcinoma
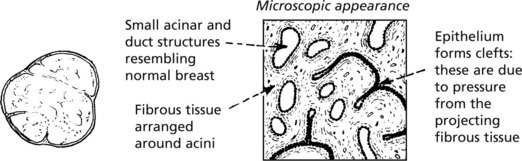
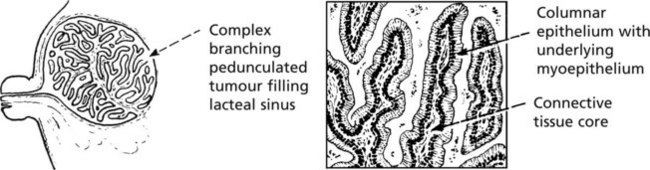
Duct Papilloma
This tumour may develop in any part of the duct system of the breast, but is most common in the lacteal sinuses at the nipple. Two forms exist:
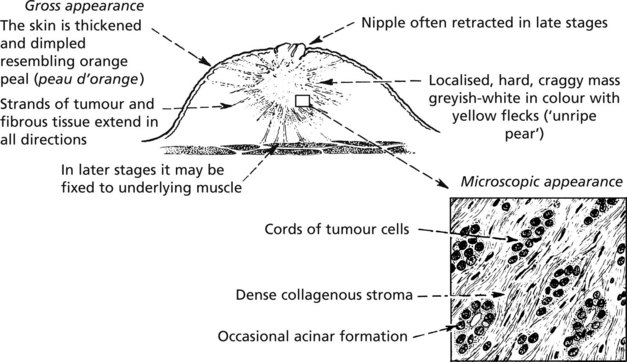
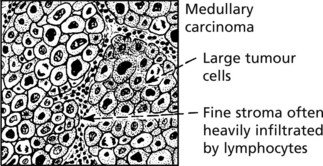
Carcinoma of the Breast
This is the commonest form of malignancy in women and rarely occurs in men. It may be found in any part of the breast but most frequently it is in the upper outer quadrant.
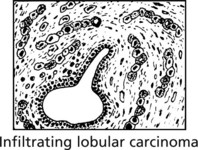
Infiltrating Lobular Carcinoma
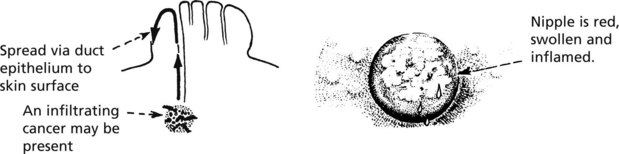
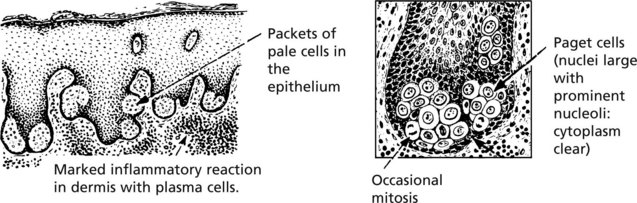
Local Spread: In late stages local infiltration causes skin ulceration and there may be direct penetration of the chest wall. Intra-epithelial spread occurs. The classical example is paget’s disease of the nipple – which may complicate intra-duct carcinoma.
Microscopic examination reveals:
Early (When the tumour is still small) |
via LYMPHATICS |
Prognosis
The most important factors determining prognosis are: