FEELING OF COLD, FEELING OF HEAT AND FEVER
FEELING OF COLD, FEELING OF HEAT AND FEVER
Feeling of cold in interior conditions
Feeling of cold in exterior conditions
How to distinguish between external and internal causes of feeling of cold
SIMULTANEOUS FEELING OF COLD AND FEVER IN EXTERIOR CONDITIONS
ALTERNATING FEELING OF COLD AND FEELING OF HEAT
FEELING OF HEAT FROM INTERNAL CAUSES
CONTRADICTORY FEELINGS OF COLD AND HEAT IN INTERNAL CONDITIONS
WHEN WE ASK
In internal conditions, questions about a patient’s feeling cold or hot are often asked towards the end of the consultation to confirm the existence of a Cold or Hot pattern. Often questions about feelings of cold or heat also help us to detect the constitutional tendency of a patient to Cold or Hot conditions. For example, patients may not have significant symptoms of Yang deficiency and Cold but, on asking, may say that they always feel cold, need to wear more clothes than other people, etc.; this symptom should never be discounted because it indicates an underlying tendency to Yang deficiency and Cold patterns.
HOW WE ASK
Terminology
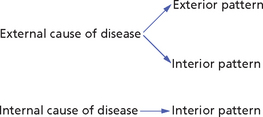
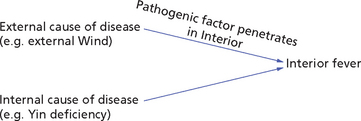
The pattern (or syndrome) refers to the location of the pathogenic factor, which may be on the Interior or Exterior: this is decided not according to the origin of the pathogenic factor but on the basis of the clinical manifestations. In other words, an external cause of disease (e.g. external Wind) may cause both an exterior pattern and an interior pattern (Fig 43.1).
FEELING OF COLD
Symptoms and Signs, Chapter 82
Aversion to wind means that the patient has goose pimples, dislikes going out in the wind and wants to stay indoors.
Feeling of cold in interior conditions
Box 43.1 summarizes the clinical manifestations of Full-Cold.
A deficiency of Yang of the Lungs or Heart, or both, will manifest especially with cold hands (Fig 43.2), a deficiency of Spleen-Yang with cold limbs and abdomen (Fig 43.3) and that of Kidney-Yang especially with cold legs, knees, feet and back (Fig 43.4). A deficiency of Stomach-Yang will manifest with cold epigastrium and cold limbs in a similar way to Spleen-Yang deficiency (Fig 43.3).
Fig. 43.2 Lung- and Heart-Yang deficiency

Fig. 43.3 Spleen-Yang deficiency
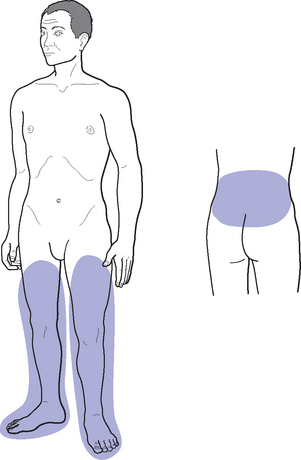
Fig. 43.4 Kidney-Yang deficiency
Box 43.2 summarizes the clinical manifestations of Empty-Cold.
There are however, other causes of cold limbs (as opposed to a general cold feeling). One is Qi stagnation: when Qi stagnates it may fail to reach the hands and feet and these become cold (Fig 43.5). This is called the ‘Four Rebellious Syndrome’, in which the ‘Four Rebellious’ indicate cold hands and feet; the famous formula Si Ni San Four Rebellious Powder is used for this pattern. An important difference between cold in the limbs due to Yang deficiency and that due to Qi stagnation is that in the former case the whole limb will be cold whereas in the latter case only the hands and feet, and especially the fingers, are cold.
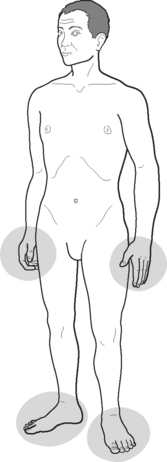
Fig. 43.5 Cold hands and feet from Qi stagnation
Besides this, cold limbs may also derive in women from Blood deficiency; this is due to the deficient Blood not reaching the extremities. In cases of Heart-Blood deficiency only the hands and chest will be cold (Fig 43.6), whereas in cases of Liver-Blood deficiency the feet will be cold (Fig 43.7).

Fig. 43.6 Heart-Blood deficiency
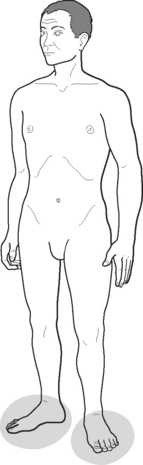
Fig. 43.7 Liver-Blood deficiency
Box 43.3 summarizes the patterns underlying a cold feeling and cold limbs in interior conditions.
Feeling of cold in exterior conditions
External invasions
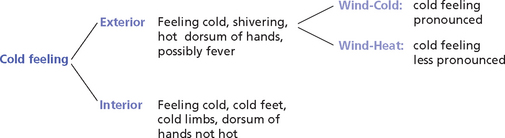
The areas that are usually touched to gauge this are the dorsum of the hands and the forehead. It should be stressed that the feeling of cold and fever (or body feeling hot to the touch) are simultaneous and not alternating: thus, if a patient feels cold in the morning without a fever and without body feeling hot to the touch and has a fever in the evening, this would correspond to the Lesser-Yang syndrome and would not constitute the beginning stage of an invasion of Wind. Figure 43.8 differentiates the manifestations of cold feeling in exterior and interior conditions.
Box 43.4 summarizes the clinical manifestations of interior and exterior pathogenic factors.
How to distinguish between external and internal causes of feeling of cold
When the patient suffers from interior Cold, there are none of the above symptoms. Another distinction between a cold feeling in exterior syndromes and one in interior syndromes is that in the former case the cold feeling is not alleviated by covering oneself, while in the latter case it is. In fact patients who feel cold and shiver from an invasion of exterior Wind will want to go to bed and cover up with blankets, but this will not alleviate the cold feeling and shivering. If a patient suffers from internal Cold, this will be alleviated by covering oneself. Table 43.1 summarizes the differentiation between external and internal Cold.
Table 43.1
Differentiation between external and internal Cold
| External invasion of Cold | Internal Cold |
| Feels cold, shivers, dislikes going out, fever, sneezing, cough, sore throat, nasal discharge | Feels cold, none of the symptoms associated with an external invasion is present |
| Cold feeling not alleviated by wrapping up in clothes and blankets | Cold feeling is alleviated by wrapping up warm |
SIMULTANEOUS FEELING OF COLD AND FEVER IN EXTERIOR CONDITIONS
A simultaneous feeling of cold and fever indicates the invasion of an exterior pathogenic factor and that this factor is still on the Exterior. The simultaneous presence of a cold feeling or shivers with a fever, or both, usually indicates an acute invasion of Wind and it denotes that the pathogenic factor is still on the Exterior: as long as there is a feeling of cold the pathogenic factor is on the Exterior. The clinical situations when the pathogenic factor is on the Exterior are described in the Greater-Yang pattern within the Six Stages from the ‘Discussion of Cold-induced Diseases’ (Shang Han Lun) and the Defensive-Qi level within the Four Levels described by the School of Warm Diseases (Wen Bing) of the Qing dynasty (see Part 6). As mentioned above, it is important to stress that the feeling of cold and fever (or body feeling hot to the touch) are simultaneous and not alternating (Fig 43.9).

Fig. 43.9 Simultaneous feeling of cold and fever
The pathogenic factors discussed are:
Cold feeling (‘aversion to cold’) in exterior patterns
As mentioned above, there are four different degrees of ‘cold feeling’ in Exterior conditions: ‘aversion to wind’, ‘fear of cold’, ‘aversion to cold’ and ‘shivers’. The clinical significance of these four degrees of feeling of cold in the context of exterior invasions is listed in Box 43.5.
Thus, generally speaking, there are three aspects to the ‘cold feeling’ in invasions of exterior Wind: the patient feels cold, has ‘waves’ of shivers and is reluctant to go out and wants to stay indoors near sources of heat. Except in mild cases, the cold feeling is not relieved by covering oneself.
Fever in exterior patterns
In fact, it is a characteristic of Fa Shao (so-called ‘fever’) in the exterior stage of invasions of Wind that the dorsum of the hands feels hot compared with the palms and the upper back feels hot compared with the chest.1 This objective hot feeling of the patient’s body may or may not be accompanied by an actual fever. Indeed, in fevers of internal origin, there may even be cases when the patient has an actual low-grade fever and the body feels cold to the touch.
Wind-Cold and Wind-Heat
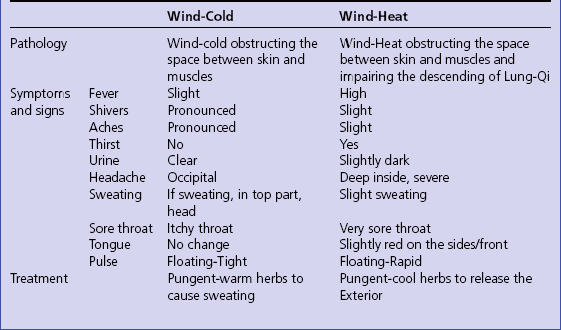
Clinical manifestations of Wind-Heat and Wind-Cold
Although a fever is more likely to occur in invasions of Wind-Heat, the differentiation between Wind-Heat and Wind-Cold is not made on the basis of the intensity of aversion to cold and fever (or a hot feeling of the body). Other factors such as the tongue and other symptoms help us to differentiate between Wind-Cold and Wind-Heat. These are listed in Table 43.2.
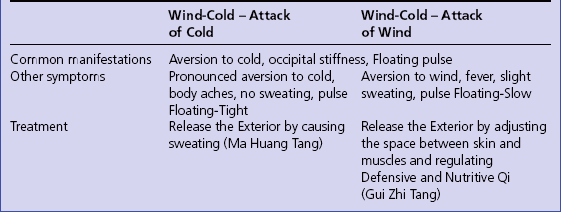
Wind-Cold: differentiation between ‘Attack of Wind’ and ‘Attack of Cold’
So far we have talked about Wind-Cold in general but the ‘Discussion of Cold-induced Diseases’ differentiates between two types of Wind-Cold invasions: one with prevalence of Wind, called ‘Attack of Wind’, and the other with prevalence of Cold, called ‘Attack of Cold’. The Attack of Wind is described in Clause 2 of the ‘Discussion of Cold-induced Diseases’: ‘The Greater-Yang pattern with fever, sweating, aversion to wind and a Floating and Slowed-down pulse is called Attack of Wind’.2 It may seem strange that the pulse is Slowed-down in this pattern as Wind is a Yang pathogenic factor that moves and opens. However, it is also true that Wind may cause stiffness (as in occipital stiffness in Wind-Cold invasions), rigidity and paralysis; thus it is quite possible for the Attack of Wind of external Wind-Cold to cause a Slowed-down pulse (which is less slow than the Slow pulse). The commentary to Clause 2 confirms that Huan in this case means a ‘moderate and slow (Chi) pulse’.3
Clause 3 describes the Attack of Cold: ‘The Greater-Yang pattern with fever or no fever, aversion to cold, body aches, retching and Tight pulse on both Yin and Yang, is called Attack of Cold’.4
In Attack of Wind, the patient’s Nutritive Qi is more deficient than in the Attack of Cold and this causes a slight sweating. Other symptoms are tabulated in Table 43.3.
ALTERNATING FEELING OF COLD AND FEELING OF HEAT
An alternating feeling of cold and feeling of heat (or fever) should not be confused with the simultaneous feeling of cold and fever which characterizes invasions of external Wind. There are two main differences. First, in alternating feeling of cold and feeling of heat, the feeling of heat is a subjective feeling of the patient, whereas in the simultaneous aversion to cold and fever of external invasions the feeling of heat is an objective feeling of heat on palpation of the patient’s forehead and hands. Secondly, in alternating feeling of cold and feeling of heat, the cold and hot sensations alternate whereas in aversion to cold and fever, they are simultaneous.
Alternating feeling of cold and feeling of heat occurs also in external invasions, but only those affecting the Lesser-Yang channels (whereas aversion to cold and fever occurs in external patterns affecting the Greater-Yang channels). This symptom is a chief symptom of the Lesser-Yang pattern within the Six Stages (Chapter 105) or of the Gall-Bladder Heat pattern within the Four Levels (Chapter 104). The latter is also a Lesser-Yang-type of pattern but with the prevalence of heat rather than cold. This is reflected in the patient’s sensations in that the feeling of heat is predominant over the feeling of cold.
Case history 43.1 illustrates a pattern causing alternating feeling of heat and feeling of cold.
FEELING OF HEAT FROM INTERNAL CAUSES
A subjective feeling of heat may be caused by Full-Heat or Empty-Heat of any organ. In Full-Heat, the feeling of heat is somewhat more intense than in Empty-Heat; another difference is that in Empty-Heat, the feeling of heat tends to be more marked in the afternoon or evening. Also, Empty-Heat is characterized by a feeling of heat especially in the Yin areas of the body, and particularly in the chest, palms and soles. Of course, the differentiation between Full-Heat and Empty-Heat is done on the basis of other manifestations such as thirst, complexion and most of all the tongue, which will be Red with a coating in Full-Heat and Red without coating in Empty-Heat. The main differentiating manifestations of Full-Heat and Empty-Heat are shown in Box 43.7.
We should bear in mind that, in some cases, a person may feel hot in general but simultaneously experience cold feet, for example. Therefore, when a patient replies affirmatively to the question ‘Do you have a tendency to feel hot in general?’, our questioning should not stop there; rather it should continue in order to ascertain whether there is any cold feeling in any particular parts of the body. For a discussion on the clinical significance of simultaneous (and contradictory) hot and cold feelings in internal conditions, see below.
INTERIOR FEVER
Symptoms and Signs, Chapter 82
By ‘fever’ is meant the situation when the patient has a fever but no simultaneous cold feeling or shivers; thus, we are now discussing interior fevers, which, it should be remembered, may be of external or internal origin. An interior fever of external origin is one caused by an exterior pathogenic factor (such as Wind-Heat, Wind-Cold or Damp-Heat) which has penetrated into the Interior and caused a fever; an interior fever of internal origin stems from an internal disharmony such as interior Heat, Yin deficiency, Qi or Blood deficiency and Blood stasis (Figs 43.10 and 43.11).

There are three degrees of interior fever (or hot body sensation); these are listed in Box 43.8.
Acute fever
When discussing fevers of internal origin, it is important to differentiate between acute and chronic fever. Acute interior fevers usually develop from the acute stage of an invasion of external Wind: both Wind-Cold and Wind-Heat may lead to an interior fever. Thus, the fever discussed here is primarily an acute fever deriving from external causes but at the interior stage. In such acute fevers the identification of patterns according to the Four Levels provides the best framework of interpretation and is clinically more relevant than the identification of patterns according to the Six Stages. However, there may be other acute interior fevers that are of internal origin, for example from Damp-Heat in the Liver and Gall-Bladder (febrile episode of cholecystitis) , or Damp-Heat in the Bladder (cystitis with fever) (Fig 43.12).
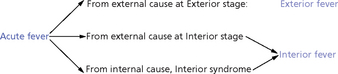
Fig. 43.12 Origin of acute fevers
The Four Levels
The Four Levels patterns are discussed in Chapter 104. Within the Four Levels, the Defensive-Qi level is the only Exterior one and therefore there is simultaneous fever and shivering with a cold feeling. At the other three levels (Qi, Nutritive Qi and Blood), Heat is in the Interior and the fever is interior. The identification of patterns according to the Four Levels describes the symptomatology of invasions of Wind-Heat. However, fever, to a lesser degree, may be present also in invasions of Wind-Cold, for which the identification of patterns according to the Six Stages is used.
The clinical manifestation of the Four Levels in fever is summarized in Box 43.9.
Damp-Heat in the Stomach and Intestines
This is Damp-Heat in the Stomach and Intestines level within the Four Levels.
Chronic fever
Empty-Heat from Yin deficiency
These are the general symptoms of Empty-Heat deriving from Yin deficiency; they may arise from the Lungs, Heart, Stomach, Spleen, Liver and Kidneys. Other accompanying symptoms (or more accentuated symptoms) according to the organ involved are listed in Box 43.10.
Qi deficiency
Clinical manifestations Low-grade fever or feeling of heat that is aggravated by overwork, dizziness, tiredness, depression, muscular weakness, spontaneous sweating, shortness of breath, loose stools, poor appetite, weak voice, Pale tongue and Weak or Empty pulse.
This fever is caused by a severe deficiency of Qi, usually of the Spleen, Stomach and Lungs, and a deficiency of the Original Qi. This situation was described by Li Dong Yuan in the famous classic ‘Discussion on Stomach and Spleen’ (Pi Wei Lun) (see Bibliography). He said that overwork and irregular diet weaken the Qi of the Stomach and Spleen and the Original Qi, which resides in the Lower Field of Elixir (Dan Tian); here it shares a place with the (physiological) Minister Fire. If the Minister Fire is stirred by overwork and emotional problems, it becomes pathological, ‘displaces’ the Original Qi in the Lower Field of Elixir and it rises upwards causing a low-grade fever or a feeling of heat (Fig 43.13).
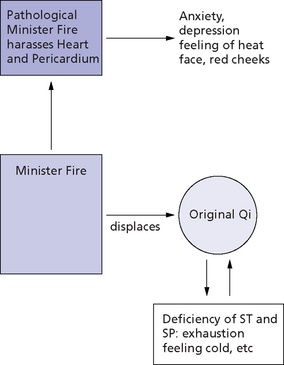
Fig. 43.13 Pathology of Yin Fire
CONTRADICTORY FEELINGS OF COLD AND HEAT IN INTERNAL CONDITIONS
NOTES
1. Tao, Deng Tie. Practical Chinese Diagnosis (Shi Yong Zhong Yi Zhen Duan Xue  ). Shanghai: Shanghai Science Publishing House, 1988; 90.
). Shanghai: Shanghai Science Publishing House, 1988; 90.
2. Shang Han Lun Research Group of the Nanjing College of Chinese Medicine. An Explanation of the ‘Discussion of Cold-induced Diseases’ (Shang Han Lun Yi Shi  ). Shanghai: Shanghai Science Publishing House, 1980; 351.
). Shanghai: Shanghai Science Publishing House, 1980; 351.
3. Shang Han Lun Research Group of the Nanjing College of Chinese Medicine. An Explanation of the ‘Discussion of Cold-induced Diseases’ (Shang Han Lun Yi Shi  ). Shanghai: Shanghai Science Publishing House, 1980; 351.
). Shanghai: Shanghai Science Publishing House, 1980; 351.
4. Shang Han Lun Research Group of the Nanjing College of Chinese Medicine. An Explanation of the ‘Discussion of Cold-induced Diseases’ (Shang Han Lun Yi Shi  ). Shanghai: Shanghai Science Publishing House, 1980; 354.
). Shanghai: Shanghai Science Publishing House, 1980; 354.