29 Fatigue
It’s like my legs weigh 100 pounds…1
You think about it, dwell on it and it makes it worse. So, part of it is mental and part of it is physical fatigue. You are not your normal self and you are just tired of everything that has happened.1
It’s like being wiped out …my body is just too tired for me to care.2
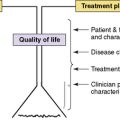
The direct effects of disease, side effects of treatment3 and medications prescribed to manage these contribute to fatigue in children with life-threatening illnesses. Infection, electrolyte imbalance, anemia, dehydration, malnutrition, endocrine dysfunction, and organ impairment are all factors. Psychological states including anxiety, fear, depression, and feelings of isolation and loneliness also influence the frequency and intensity of fatigue.4 Sleep disruption and poor sleep quality contribute to fatigue in children, particularly at the end of life. Sleep deprivation may worsen pain that exacerbates their tiredness. Children with cancer identify the hospital environment as a major contributing factor to fatigue because of the frequent disruptions in their sleep5 (Tables 29-1 and 29-2).
TABLE 29-1 Fatigue: Contributing Factors in Children with a Life-Threatening Illness
| Factor | Possible causes |
|---|---|
| Physical |
TABLE 29-2 Signs and Symptoms of Fatigue in Children
| Domain | Clinical findings |
|---|---|
| Cognitive | |
| Physical | |
| Emotional |
Children’s Descriptions of Fatigue
Researchers exploring fatigue in seriously ill children confirm that perceptions of fatigue differ by developmental age.6–8 Younger children tend to emphasize the physical sensation of fatigue more than emotional aspects, and describe, for example, how watching television or reading comprise their main activities.
Adolescents tend to be more cognitively aware of the impact of fatigue on their lives, and often describe the symptom in terms of its effect on their lifestyle. They also highlight mental tiredness that alternates and at times merges with the physical sensation of fatigue.3,7–10 Teens describe activities that they can no longer perform and their inability to be with peers as significant changes brought on by fatigue. They are more aware of the relationship of the symptom to their overall illness or treatment. For example, adolescents can define when fatigue occurs in relation to their chemotherapy cycle.
Research on Fatigue in Children
Research on fatigue in children has focused primarily on children with rheumatologic disorders and cancer. Fatigue is characterized as a distressing, pervasive symptom with physical, mental, and emotional components characterized by a lack of energy.9,10
Children with juvenile rheumatoid arthritis and systemic lupus erythematous (SLE) describe fatigue as a common symptom.11,12 In a study of 51 children with juvenile polyarticular arthritis, researchers found fatigue present along with pain and joint stiffness on more than 70% of days with significant variability in symptom levels.13 Researchers found a positive relationship between stress and mood and same-day variations in fatigue. A study of 15 children with SLE found fatigue to be a significant symptom in 67% of the children.14 These children also had reduced aerobic fitness compared to age and sex-matched reference norms. Fatigue was a significant symptom in a group of 52 children with Crohn’s disease.15 They had lower quality of life scores and significantly more fatigue compared with healthy controls.
Fatigue is the most frequent symptom experienced by children with cancer.9,10,16–20 In a survey of parents of children with cancer and their treating clinicians, 57% in each group reported fatigue as a frequent symptom.19 In a qualitative study of children receiving treatment for cancer, researchers generated a detailed description of fatigue: a core concept or energy, a core process or managing dwindling energy, and a typology of three types of fatigue: typical tiredness, treatment fatigue, and shutdown fatigue.18 Children with leukemia described fatigue, both disease and treatment-related, as having the greatest impact on their quality of life by altering participation in school, sports, and family activities. In a pilot study of nine school-age children with leukemia, diaries revealed evening fatigue and sleep disturbances21 during the maintenance phase of treatment. Fatigue was also the most frequently reported symptom in a group of 161 acute lymphocytic leukemia survivors,22 even many years after treatment.
Studies have specifically addressed fatigue at the end of life within the childhood cancer population.23 A landmark study of symptoms and suffering at the end of life found that all 103 families surveyed report that their child had experienced fatigue during the last month of life.4 In a Swedish nationwide survey of 449 parents of children with cancer, 86% reported physical fatigue as the most frequently reported symptom that had moderate or high impact on their child’s well-being.24 A study of 65 parents of children who had died of cancer within the previous 6 to 10 months revealed that fatigue was one of the most frequently reported symptoms, along with pain, and changes in behavior, appearance, and breathing.25 Similar findings were found in 32 parents whose child had died within the past 3 years. They reported that the symptom burden was high during the palliative phase, with pain, poor appetite, and fatigue as the most frequently reported physical symptoms. Emotional symptoms included sadness, difficulty talking about feelings, and fear of being alone.26 Fatigue was a prevalent symptom in a group of 28 Japanese children at the end of life.27 In interviews with 30 parents whose children had received pediatric home hospice services, fatigue was one of the most frequently identified symptoms during the last week of their child’s life28 (Fig. 29-1).

Fig. 29-1 Parents need help with understanding the significant effects fatigue can have on their child.
A qualitative study exploring factors that influence quality of life in 49 children and adolescents with epilepsy found excessive fatigue as a barrier to academic and social pursuits. Participants described how intermittent or continuous fatigue made it difficult to think clearly and to fully participate in classroom learning.29
Fatigue may provide protection, as a shield from suffering, during the final stages of life; and treatment of fatigue at this stage of palliative care may be detrimental.30 When the death of a child is imminent, fatigue often intensifies and withdrawal from family and friends occurs as a result of diminished energy. Preparing the family for this eventuality may prevent their misinterpretation of tiredness as depression, or, even more painful, as a rejection of them (Fig. 29-2).
Assessment of Fatigue
Many patients and families assume that fatigue is an inevitable and untreatable side effect of disease or treatment and thus often do not report it as a symptom. Furthermore, until recently, standardized assessment of fatigue by clinicians has been oversimplified, as a yes or no checklist,6 or entirely absent.
Guidelines from the National Comprehensive Cancer Network recommend routine screening for fatigue as the sixth vital sign. Those older than 12 years of age should be screened using a simple numeric rating scale such as 0, no fatigue, to 10, worst fatigue. For children 7 to 12 years of age, a 1 to 5 point scale is recommended. For children aged 5 and 6 years the words tired or not tired should be used to determine fatigue. Once screened, patients should be evaluated for the seven treatable contributing factors to fatigue, which is informally referred to as the gang of seven: anemia, pain, sleep difficulties, nutrition issues, changes in activity patterns, emotional distress, and presence of co-morbidities.31–33 The health care team should assess for the onset and type of fatigue, aggravating or alleviating factors, and degree of interference with the child’s functioning.
Several research instruments are available to assess symptom clusters in children, including fatigue, although none was designed specifically for end of life. Once fatigue has been identified as a specific symptom it may be useful to use one of the validated and reliable pediatric fatigue scales, such as the Memorial Symptom Assessment Scale (MSAS), Edmonton Symptom Assessment Scale (ESAS), or the Pediatric Quality of Life (PedsQL) scale.34
The Childhood Fatigue Scale (CFS) is a 14-item (four-point Likert scale) questionnaire that asks children (ages 7 to 12 years) about their tiredness during the previous week. The three subscales are: lack of energy, inability to function, and altered mood.8,35 Parent Fatigue Scale (PFS) is a 17-item inventory of parents’ perception of their child’s fatigue in the previous week. In addition to the three subscales on the children’s version, it also included a scale of altered sleep. The Fatigue Scale-Adolescent (FS-A) is a 14-item questionnaire that asks adolescents (ages 13 to 18 years), to evaluate their fatigue experience during the previous week. The child and parent scales are available in English and Spanish; the adolescent form in English only. The CFS, PFS, and FS-A are validated research instruments, easy to administer, and require limited time to complete in the clinical setting.8,35,36
The PedQL Multidimensional Fatigue Scale is an 18-item research instrument (ages 2 to 18) with three subscales: general fatigue, sleep-rest fatigue, and cognitive fatigue. The scale is self-administered for 8 to 18 year olds, interview-administered in 5 to 7 year olds and done by parent proxy for the youngest children. It is available in 22 languages.37,38 The Pediatric Functional Assessment of Chronic Illness Therapy-Fatigue (Peds FACIT-F) is an 11-item scale for children with cancer that measures fatigue in the past 7 days. It is correlated with the Peds QL Multidimensional Fatigue Scale and is available in English and Spanish.35,39
Interventions for Fatigue
Sixty Turkish children, ages 7 to 12 years, with leukemia or lymphoma, who were receiving their first 7- to 10-day course of chemotherapy, were randomized to an experimental group who received fatigue education or a control group who received standard care. The experimental group received a handbook on fatigue and nutritional counseling. Children and their mothers identified strategies that could decrease fatigue, such as minimizing interruptions at night during hospitalization. Developmentally appropriate activities included reading, art, music, and walking in the hallway for 10 to 15 minutes. After a 7-day period, the children were evaluated using the Child Fatigue Scale (CFS) and Parent Fatigue Scale (PFS). Mean scores for the experimental group was significantly lower than the control group. Methods that helped alleviate fatigue were taking naps, walking, eating well-balanced meals, increasing visitor interaction, and having fun activities to distract from the sense of being tired.40
In another study, 13 children ages 5 to 15 years with leukemia and lymphoma and their parents were interviewed regarding quality of life during therapy.18 One area dealt with ways to replenish, conserve, and preserve energy to alleviate physical, mental, and emotional fatigue. Strategies to replenish energy or promote relaxation included taking hot baths and naps, receiving massage, or engaging in quiet activities. Distractions such as watching television, playing with animals, and doing puzzles were also helpful. Conserving strategies included activities that required minimal energy expenditure such as watching television without the sound, resting the mind, having only familiar people around, sleeping, being read to, and having alone time. Children’s preserving strategies to minimize further energy loss were more inward: withdrawing, ignoring people, and creating a quiet environment. Teenagers reported that the loss of control over their environment and a lack of age-appropriate activities contributed to their fatigue.18
The management of fatigue is most effective when an interdisciplinary team contributes to the plan for an individual child33 (Table 29-3). Strategies to alleviate fatigue should be an intrinsic part of dealing with a complex of associated symptoms, such as anemia, pain, sleep disturbances, and depression (Table 29-4). Children and families should be taught that while fatigue is a normal and expected symptom, there are strategies to mitigate its effects. Suggestions include setting priorities for activities and scheduling them during peak energy times, maintaining a consistent daily routine, limiting naps to 20 to 30 minutes so as not to interfere with nighttime sleep, and using play and distractions.32,33,41
TABLE 29-3 Interdisciplinary Approach to Fatigue Interventions
| Discipline | Interventions |
|---|---|
| Nursing |
TABLE 29-4 Possible Interventions for Fatigue and Contributing Symptoms
| Correct potential factors associated with fatigue | Medical/pharmacologic interventions | Nonpharmacolgic interventions |
|---|---|---|
| Anemia | Educate regarding foods high in iron | |
| Pain | Provide adequate pain management, including adjuvants | |
| Careful consideration of hypnotics | ||
| Inactivity | Incorporate activity, exercise regimen as tolerated | |
| Depression | Antidepressants | |
| Symptomatic fatigue |
* Increasing periods of sleep are normal at the end of life
Sleep
Inquiry and guidance regarding sleep hygiene should be integrated into regular clinic and hospital visits. The need for regular and adequate sleep is particularly important to emphasize when counseling adolescents. Considerations in the hospital include clustering care and creating a restful environment in the room.18 Limiting caffeinated drinks and foods as well as vigorous exercise within 4 hours of bedtime can promote better rest. Maintaining a consistent bedtime routine, quiet environment, and the presence of a security object are effective in promoting sleep.33 Pharmacologic interventions may be used3 and are further discussed in Chapter 30.
Exercise
Randomized controlled trials have demonstrated that exercise decreases fatigue in adults.3 Recommendations for both adults and children include starting with a low-intensity exercise regimen and adjusting as needed based on the patient’s clinical condition.32 Before initiating an exercise program, a referral to physical therapy, occupational therapy, or physical medicine should be considered.
Nutrition
Children with chronic illnesses or debilitating conditions may be at particular risk for nutritional deficits that exacerbate fatigue. Interventions are guided by the assessment of caloric intake, fluid and electrolyte imbalances, and any barriers to intake. Megestrol acetate has been used to increase appetite but there is limited research in children.42 Correcting sodium, potassium, calcium, or magnesium electrolyte imbalances may improve fatigue symptoms as well as providing nutritional supplements. It is well recognized that decreased appetite and oral intake are common at the end of life and that the interventions at this phase of life will be different33 (Chapter 33).
Anemia
Some adult studies indicate correcting anemia with erythropoietin for cancer patients has improved their quality of life.3,33 However, in children with cancer, erythropoietin improved the anemia but it did not significantly improve their quality of life. Correcting anemia alone does not address the multidimensional factors associated with fatigue.43 If anemia is identified as the significant factor in the child’s fatigue, red cell transfusions and erythropoietin may be considered.
Pharmacologic agents
Psycho-stimulants may be considered after careful evaluation of fatigue. Improvement in fatigue in adults has been documented with the use of methylphenidate and modafinil. While there is extensive evidence that methylphenidate is useful in the treatment of attention deficit hyperactivity disorder in children, there are no studies evaluating its use for fatigue.42 Only one case series supports the use of methylphenidate to decrease fatigue in adolescents who were receiving opioids.44 Corticosteroids and adenosine triphosphate infusions are described as pharmacologic therapies for fatigue but there are no data for their use in children.3,33
Complementary and Alternative Medicine
Complementary and alternative medicine (CAM) is a growing field and data suggest that many parents pursue these therapies for their children. Estimates of pediatric CAM use range from 2% to 70%.45 A 2007 National Health Interview survey evaluated CAM use in 9000 children under 17 years and found that 12% had used some form of CAM during the previous 12 months.46 A recent survey of 281 families reported that 52.3% of children had used one or more types of CAM therapies in the previous year. Children with epilepsy and cancer used CAM most frequently.47 In a review of 482 pediatric and adolescent charts, 34.6% were taking 1 to 10 CAM products. A significant predictor of this use was a presenting symptom of poor energy or fatigue.45
When faced with life-threatening illnesses, parents often pursue CAM therapies to ensure that they have left no stone unturned.48 Patients and families tend to seek CAM when symptoms are not adequately treated with conventional approaches.49 The National Center for Complementary and Alternative Medicine has identified four major domains of CAM therapies: mind-body medicine, manipulative body-based practices, energy, and biologic therapies.48 Massage is the CAM most frequently cited for fatigue management. Incorporating cognitive behavior therapy (CBT), stress management, guided imagery, and relaxation also may reduce fatigue.33
Over a 1-year period, 17 parent-child dyads were randomized to receive massage therapy or quiet time and then crossed over to the other treatment option. Pain, nausea, anxiety, fatigue, vital signs, and cortisol levels were assessed. There were no significant changes in fatigue with either the massage or the quiet time. Children reported feeling relaxed but some had a difficult time conceptualizing the difference between fatigue and relaxation.50 A study of 68 mothers who received massage while their children were hospitalized had decreased fatigue and increased vigor. Researchers suggested that decreasing fatigue in mothers caring for their sick children may lead to improved support to their children.51 Healing touch and acupuncture in adults have demonstrated effectiveness in reducing cancer-related fatigue but no studies are available in children.48
l-Carnitine deficiency is observed in pediatric AIDS patients and both adult and pediatric cancer patients presenting with fatigue.48,52 Earlier studies suggest that a week of carnitine supplementation reduced fatigue and improved functioning in adult hospice patients without adverse events. However, a recent double-blind, placebo-controlled study in adults did not support the reversal of cancer-related fatigue even though serum levels improved with l-carnitine supplementation.48,52 In a double-blind randomized controlled trial with 15 adult hospice patients who received transcutaneous electrical nerve stimulation (TENS) for 6 days found that fatigue improved significantly over the sham TENS.53
1 Hockenberry-Eaton M., Hinds P.S., Alcoser P. Fatigue in children and adolescents with cancer. J Pediatr Oncol Nurs. 1998;15(3):172-182.
2 Hicks J., Bartholomew J., Ward-Smith P., et al. Quality of life among childhood leukemia patients. J Pediatr Oncol Nurs. 2003;20(4):192-200.
3 Ullrich C.K., Mayer O.H. Assessment and management of fatigue and dyspnea in pediatric palliative care. Pediatr Clin North Am. 2007;54:735-756.
4 Wolfe J., Grier H.E., Klar N., et al. Symptoms and suffering at the end of life in children with cancer. N Engl J Med. 2000;342:326-333.
5 Hinds P.S., Hockenberry M., Rai S.N., et al. Nocturnal awakenings, sleep environment interruptions, and fatigue in hospitalized children with cancer. Oncol Nurs Forum. 2007;34:393-402.
6 Eddy L., Cruz M. The relationship between fatigue and quality of life in children with chronic health problems: a systematic review. J Spec Pediatr Nurs. 2007;12:105-114.
7 Hockenberry-Eaton M., Hinds P.S. Fatigue in children and adolescents with cancer. In: Winningham M.L., Barton-Burke M., editors. Fatigue in cancer. Boston: Jones and Bartlett Publishers; 2000:71-85.
8 Hockenberry M.J., Hinds P.S., et al. Three instruments to assess fatigue in children with cancer: the child, parent and staff perspectives. J Pain Symptom Manage. 2003;25(4):319-328.
9 Hockenberry-Eaton M., Hinds P.S., Alcoser P. Fatigue in children and adolescents with cancer. J Pediatr Oncol Nurs. 1998;15(3):172-182.
10 Hockenberry-Eaton M., Hinds P., O’Neill J.B., et al. Developing a conceptual model for fatigue in children. Eur J Oncol Nurses. 1999;3(1):5-11.
11 Ward T.M., Brandt P., Archbold K., et al. Polysomnography and self-reported sleep, pain, fatigue, and anxiety in children with active and inactive juvenile rheumatoid arthritis. J Pediatr Psychol. 2008;33:232-241.
12 Sällfors C., Hallberg L.R., Fasth A. Well-being in children with juvenile chronic arthritis. Clin Exp Rheumatol. 2004;22:125-130.
13 Schanberg L.E., Gil K.M., Anthony K.K., et al. Pain, stiffness, and fatigue in juvenile polyarticular arthritis: contemporaneous stressful events and mood as predictors. Arthritis Rheum. 2005;52:1196-1204.
14 Houghton K.M., Tucker L.B., Potts J.E., et al. Fitness, fatigue, disease activity, and quality of life in pediatric lupus. Arthritis Rheum. 2008;59:537-545.
15 Marcus S.B., Strople J.A., Neighbors K., et al. Fatigue and health-related quality of life in pediatric inflammatory bowel disease. Clin Gastroenterol Hepatol. 2009;7:554-561.
16 Perdikaris P., Merkouris A., Patiraki E., et al. Changes in children’s fatigue during the course of treatment for pediatric cancer. Int Nurs Rev. 2008;55:412-419.
17 Whitsett S.F., Gudmundsdottir M., Davies B., et al. Chemotherapy-related fatigue in childhood cancer: correlates, consequences, and coping strategies. J Pediatr Oncol Nurs. 2008;25:86-96.
18 Davies B., Whitsee S., Bruce A., et al. A typology of fatigue in children with cancer. J Pediatr Oncol Nurs. 2002;19(1):12-21.
19 Gibson F., Barnett M., Richardson A., et al. Heavy to carry, a survey of parents’ and healthcare professionals perceptions of cancer-related fatigue in children and young people. Cancer Nurs. 2005;28(1):27-35.
20 Erickson J.M. Fatigue in adolescents with cancer: a review of the literature. Clin J Oncol Nurs. 2004;8:139-145.
21 Gedaly-Duff V., Lee K.A., Nail L.M., et al. Pain, sleep disturbance, and fatigue in children with leukemia and their parents: a pilot study. Oncol Nurs Forum. 2006;33(3):641-646.
22 Meeske K.A., Hicks J., Bartholomew J., Ward-Smith P., et al. Quality of life among childhood leukemia patients. J Pediatr Oncol Nurs. 2003;20(4):192-200.
23 Mooney-Doyle K. An examination of fatigue in advanced childhood cancer. J Pediatr Oncol Nurs. 2006;23:305-310.
24 Jalmsell L., Kreicbergs U., Onelov E., et al. Symptoms affecting children with malignancies during the last month of life: a nationwide follow-up. Pediatrics. 2006;117:1314-1320.
25 Pritchard M., Burghen E., Srivastava D.K., et al. Cancer-related symptoms most concerning to parents during the last week and last day of their child’s life. Pediatrics. 2008;121:e1301-e1309.
26 Theunissen J.M., Hoogerbrugge P.M., van Achterberg T., et al. Symptoms in the palliative phase of children with cancer. Pediatr Blood Cancer. 2007;49(2):160-165.
27 Hongo T., Watanabe C., Okada S., et al. Analysis of the circumstances at the end of life in children with cancer: symptoms, suffering and acceptance. Pediatr Int. 2003;45:60-64.
28 Hendricks-Ferguson V. Physical symptoms of children receiving pediatric hospice care at home during the last week of life. Oncol Nurs Forum. 2008;35(6):E108-115.
29 Elliott I.M., Lach L., Smith M.L. I just want to be normal: a qualitative study exploring how children and adolescents view the impact of intractable epilepsy on their quality of life. Epilepsy Behav. 2005;7:664-678.
30 Radbruch L., Strasser F., Eisner F., et al. Fatigue in palliative care patients-an EAPC approach. Palliat Med. 2008;22:13-32.
31 Piper B.F., Borneman T., Sun V.C., et al. Cancer-related fatigue: role of oncology nurses in translating national comprehensive cancer network assessment guidelines into practice. Clin J Oncol Nurs. 2008;12:37-47.
32 Mock V., Atkinson A., Barsevick A.M., et al. Cancer-related fatigue: clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2007;5:1054-1078.
33 National Comprehensive Cancer Network (NCCN). Available at. July 25, 2009. www.ncc.org/professionals/physician_gls/f_guidelines.asp.. Originally accessed
34 Paice J.A. Assessment of symptom clusters in people with cancer. J Natl Cancer Inst Monogr. 2004;32:98-102.
35 Hockenberry M. Nausea, vomiting, anorexia and fatigue. In: Wiener L.S., Pau M., editors. Quick Reference for Pediatric Oncology Clinicians: The Psychiatric and Psychological Dimensions of Pediatric Cancer Symptom Management. Charlottesville, Va: IPOS Press; 2009:104-107.
36 Hinds P.S., Hockenberry M., Tong X., et al. Validity and reliability of a new instrument to measure cancer-related fatigue in adolescents. J Pain Symptom Manage. 2007;34:607-618.
37 Varni J.W., Burwinkle T.M., Szer I.S. The PedsQL multidimensional fatigue scale in pediatric rheumatology: reliability and validity. J Rheumatol. 2004;31:2494-2500.
38 Varni J.W., Burwinkle T.M., Katz E.R., et al. The PedsQL in pediatric cancer: reliability and validity of the pediatric quality of life inventory generic core scales, multidimensional fatigue scale, and cancer module. Cancer. 2002;94:2090-2106.
39 Lai J.S., Cella D., Kupst M.J., et al. Measuring fatigue for children with cancer: development and validation of the pediatric functional assessment of chronic illness therapy-fatigue (peds FACIT-F). J Pediatr Hematol Oncol. 2007;29:471-479.
40 Genc R.E., Conk Z. Impact of effective nursing interventions to the fatigue syndrome in children who receive chemotherapy. Cancer Nurs. 2008;31:312-317.
41 Radbruch L., Strasser F., Eisner F., et al. Fatigue in palliative care patients-an EAPC approach. Palliat Med. 2008;22:13-32.
42 McCullough R., Comac M., Craig F. Paediatric palliative care: coming of age in oncology? Eur J Cancer. 2008;44:1139-1145.
43 Razzouk B.I., Hord J.D., Hockenberry M., et al. Double-blind, placebo-controlled study of quality of life, hematologic end points, and safety of weekly epoietin alfa in children with cancer receiving myelosuppressive chemotherapy. J Clin Oncol. 2006;27:3583-3589.
44 Yee J.D., Berde C.B. Dextroamphetamine or methylphenidate as adjuvants to opioid analgesia for adolescents with cancer. J Pain Symptom Manage. 1994;9:122-125.
45 Wilson K., Busse J., Gilchrist A., et al. Characteristics of pediatric and adolescent patients attending a naturopathic college clinic in Canada. Pediatrics. 2005;115:e338-343.
46 National Center for Complementary and Alternative Medicine. Complementary and Alternative Medicine use in children. Available at. July 25, 2009. http://nccam.nih.gov/health/children/. (Originally accessed)
47 Post-White J., Fitzgerald M., Hageness S., et al. Complementary and alternative medicine use in children with cancer and general and specialty pediatrics. J Pediatr Oncol Nurs. 2009;26:7-15.
48 Ladas E., Post-White J., Hawks R., et al. Evidence for symptom management in the child with cancer. J Pediatr Hematol Oncol. 2006;28:601-615.
49 Steinhorn D.M., Rogers M. Complementary and alternative medicine. In: Goldman A., Hain R., Liben S., editors. Oxford textbook of palliative care for children. Oxford: Oxford University Press; 2006:484-496.
50 Post-White J., Fitzgerald M., Savik K., et al. Massage therapy for children with cancer. J Pediatr Oncol Nurs. 2009;26:16-28.
51 Iwasaki M. Interventional study on fatigue relief in mothers caring for hospitalized children-effect of massage incorporating techniques from oriental medicine. Kurume Med J. 2005;52:19-27.
52 Cruciani R.A., Dvorkin E., Homel P., et al. L-carnitine supplementation in patients with advanced cancer and carnitine deficiency: a double-blind, placebo-controlled study. J Pain Symptom Manage. 2009;37:622-631.
53 Pan C., Morrison S., Ness J., et al. Complementary and alternative medicine in the management of pain, dyspnea, and nausea and vomiting near the end of life: a systematic review. J Pain Symptom Manage. 2000;20:374-387.