[level-membership-for-dermatology-category]
13 Eyebrow height / shaping
Summary and Key Features
• Eyebrow height and shape play a key role in attractiveness, emotional expression, and perceived youthfulness; the ideal brow for an individual depends on many factors
• Enhancement of brow height and contour following treatment with botulinum toxin is well documented
• The standard injection pattern in the glabella leads to inactivation of the brow depressors and portions of the frontalis; it is likely that the compensatory increase in the resting tone of the frontalis leads to brow elevation
• Brow ptosis and a ‘mephisto’ brow are the most common complications of treatment and an understanding of the relevant anatomy can help to prevent this
• Hyaluronic acid fillers can be a useful adjunct to botulinum toxin if there has been volume loss beneath the brows
• Eyebrow asymmetry is a common problem and symmetric treatment with botulinum toxin may offer a simple, non-surgical, method of correction
Eyebrows and attractiveness
The modern concept of the ideal contour of the female brow was proposed by Westmore in 1974 (Fig. 13.1). This schema applies best to an oval-shaped face, and serves as a good starting point since there is no clear definition of an ‘ideal brow’ that can be applied to all faces (Fig. 13.2). Several authors have suggested that the ideal apex of the brow is actually more lateral than the lateral limbus as Westmore had proposed. If the apex is too medial and overelevated it creates a surprised appearance.
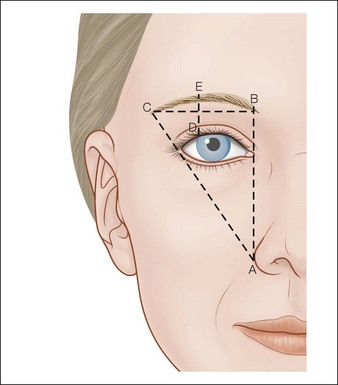
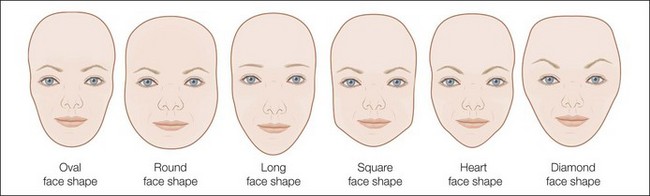
Figure 13.2 Face shapes.
Round face – to make the face appear more oval eyebrow lines should go up. A high arched brow with a lateral apex is ideal.
Long face – horizontal eyebrows draw the eye from side to side, making the face appear more oval.
Square face – angled brows balance the strong jaw line. The apex of the brow should be above the square of the jaw if possible.
Heart-shaped face – a rounded brow adds curves, softens the appearance, and emphasizes the shape.
Diamond face – a rounded brow will soften the angular face. If the face is particularly wide a peaked brow will draw the eyes up and make the face appear more oval.
Variations to Westmore’s ideal brow have been suggested to account for variations in face shape and intercanthal distance. Baker et al confirmed that, in the case of a long face and square face, observers preferred eyebrows planned by a makeup artist who accounted for these factors, rather than the Westmore ideal (see Fig. 13.2, Box 13.1).
Technique
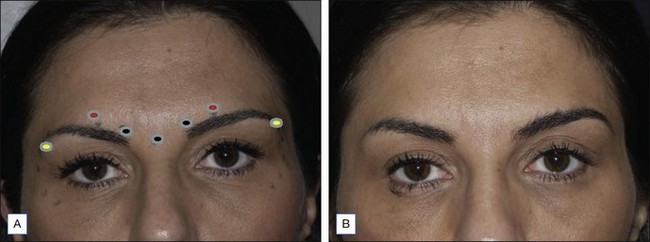
The standard injection pattern for glabella typically has five to seven injection sites and most studies looking at brow height have used this template (Figs 13.3, 13.4). We recommend an initial total dose of 20–30 units for women and 40–60 units for men (Box 13.2), distributed as shown in Figure 13.3. The first injection is typically 5–10 units into the belly of the procerus muscle. The site of the injection can be found at the center of an imaginary X drawn between the top of the medial brow and the contralateral medial canthus. The next injections are 7–10 units (15–20 units in men) bilaterally into the belly of the corrugator supercilii, which overlies the depressor supercilii and medial portion of the orbicularis oculi. The site for this injection is directly above the inner canthus, just above the supraorbital ridge. Although this landmark is typically just superior to the medial brow, the site should be chosen based on the muscular and bony landmarks regardless of the brow position. The supratrochlear artery runs just medial to this injection site so proper landmarking and post-injection pressure are important to avoid excess bruising. Next 4–5 units are injected bilaterally 1 cm above the supraorbital rim in the mid-pupillary line. This injection is the most likely to cause lid ptosis so it is important to measure 1 cm above the supraorbital rim, to inject strictly intradermally in an upwards direction, and to avoid firm massage that may displace the botulinum toxin, since the ptosis is likely caused by diffusion of the botulinum toxin into the levator palpebrae superioris (Fig. 13.5).
Box 13.2
Botulinum units
Botox® is distributed as a vacuum-dried 100 U (Allergan units) vial that is typically reconstituted with 1 mL of preserved saline for a concentration of 100 U/mL. Dysport® comes in a 500 U (Ipsen units) vial and it is recommended that it be reconstituted with 2.5 mL of physiological saline to obtain a concentration of 200 U/mL. As known, Allergan and Dysport® units are not equivalent and not interchangeable, and appropriate conversion ratios must be adopted if switching from one product to the other. Although some sources have used a higher volume of diluents, we recommend these volumes as they allow for more precise low-volume, high-concentration injections. Please refer to Chapter 9, Comparison of botulinum toxins, for a more detailed discussion. For simplicity, we have used Allergan units in this discussion.
In addition to lid ptosis, another possible complication of brow treatment is monolateral or bilateral hyperelevation of the brow’s apex, known as a ‘mephisto brow’ (Figs 13.6, 13.7).


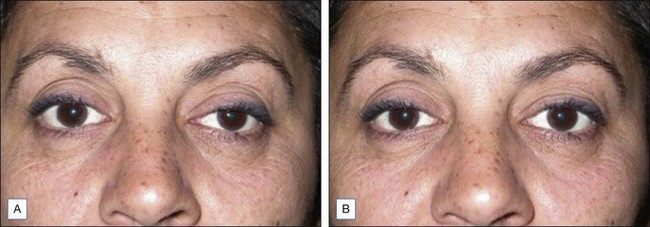
When treating eyebrows, lateral brow elevation is a common goal because it gives a more youthful appearance. In addition to the standard injection pattern previously described, some authors have achieved lateral brow elevation by treating the lateral orbicularis oculi. To achieve this 7–10 units of botulinum toxin A can be injected intradermally just inferior to the lateral brow (see Figs 13.3, 13.4). Concurrent treatment of the crow’s feet will also help to weaken the lateral orbital orbicularis oculi and contribute to brow lift. When performing this procedure it is important not to treat the lateral frontalis since this is the muscle elevating the brow. Risks with this technique include diffusion of the botulinum toxin into the levator palpebrae superioris leading to ptosis and bruising if the injections are too deep.
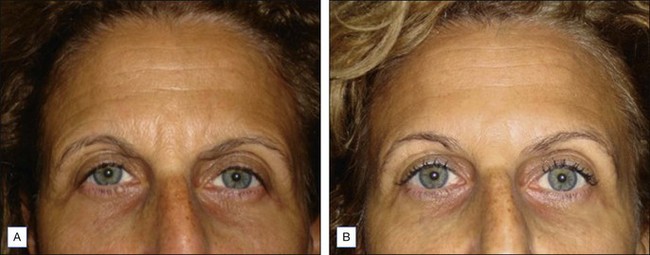
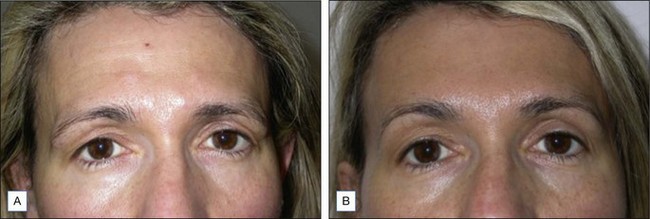
As an adjunct to the brow elevation and contouring achieved with botulinum toxin A, Lambros suggests that adding some volume to the brows with hyaluronic acid can restore a more youthful appearance (Fig. 13.8). This is achieved by adding small amounts in several deep passes beneath the brows, never going below the supraorbital rim. The amount of hyaluronic acid used is very subject specific. The ideal candidates for this procedure are those who have lost volume medially, giving them a worried appearance, and those patients who have lost volume across the entire length of the brow. This is also typically seen in upper blepharoplasty patients, especially when over-resection of fat has been performed. In these cases, the use of botulinum toxin to elevate the brows and of hyaluronic acid to compensate for iatrogenic volume loss is particularly beneficial. Intravascular injections are the most serious complication from this treatment. This risk can be lessened by using lidocaine with epinephrine for vasoconstriction and injecting small amounts at low pressure. The fine blunt-tipped cannulas may also help to minimize this risk.
Eyebrow asymmetry
Eyebrow asymmetry is common in the general population, although minimal data exist regarding the incidence. The minimum asymmetry noticeable to individuals is 2 mm, so many people with mild eyebrow asymmetry may not be aware of it. Box 13.3 lists the many potential causes of eyebrow asymmetry.







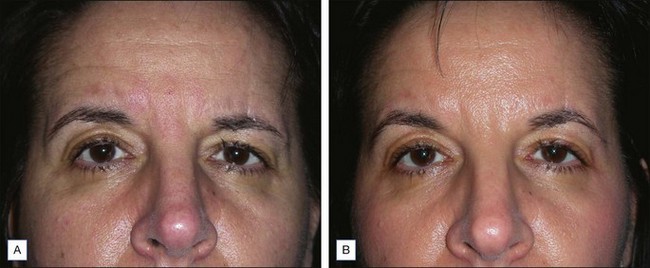
A study by Tiryaki & Ciloglu treated a group of 115 patients with eyebrow asymmetry of at least 2 mm with bilaterally symmetric injections of botulinum toxin A. There was a statistically significant decrease in the discrepancy and in 72.1% of the patients the asymmetry was corrected to less than 2 mm. Given the positive results of this study, it seems reasonable to begin by treating asymmetric brows with symmetric botulinum toxin A injections and make adjustments at future visits if the asymmetry persists (Fig. 13.9).
Ahn MS, Catten M, Maas CS. Temporal brow lift using botulinum toxin A. Plastic and Reconstructive Surgery. 2000;105:1129–1135.
Baker SB, Dayan JH, Crane A, et al. The influence of brow shape on the perception of facial form and brow aesthetics. Plastic and Reconstructive Surgery. 2007;119(7):2240–2247.
Benedetto AV, Lahti JG. Measurement of the anatomic position of the corrugator supercilii. Dermatologic Surgery. 2005;31(8 pt 1):923–927.
Carruthers A, Carruthers J. Botulinum toxin type A: history and current cosmetic use in the upper face. Seminars in Cutaneous Medicine and Surgery. 2001;20:71–84.
Chen AH, Frankel AS. Altering brow contour with botulinum toxin. Facial Plastic Surgery Clinics of North America. 2003;11:457–464.
de Almeida AT, De Boulle K. Diffusion characteristics of botulinum neurotoxin products and their clinical significance in cosmetic applications. Journal of Cosmetic and Laser Therapy. 2007;9(suppl 1):17–22.
Fashion Bomb Daily. Online. Available http://fashionbombdaily.com/2010/06/08/beauty-bomb-how-to-shape-and-care-for-eyebrows/
Frankel AS, Kamer FM. Chemical brow lift. Arch Otolaryngol Head Neck Surg. 1998;124:321–323.
Gunter JP, Antrobus SD. Aesthetic analysis of the eyebrows. Plastic and Reconstructive Surgery. 1997;99:1808–1816.
Huang W, Rogachefsky AS, Foster JA. Brow lift with botulinum toxin. Dermatologic Surgery. 2000;26:55–60.
Kowner R. Facial asymmetry and attractiveness judgment in developmental perspective. Journal of Experimental Psychology. Human Perception and Performance. 1996;22:662–675.
Lambros V. Volumizing the brow with hyaluronic acid fillers. Aesthetic Surgery Journal. 2009;29:177–179.
Matros E, Garcia JA, Yaremchuk MJ. Changes in eyebrow shape and position with aging. Plastic and Reconstructive Surgery. 2009;124:1296–1301.
Muhlbauer W, Holm C. Eyebrow asymmetry: ways of correction. Aesthetic Plastic Surgery. 1998;22:366–371.
Springer IN, Wannicke B, Warneke PH, et al. Facial attractiveness: visual impact of symmetry increases significantly towards the midline. Annals of Plastic Surgery. 2007;59:156–162.
Tiryaki T, Ciloglu NS. Eyebrow asymmetry: definition and symmetrical correction using botulinum toxin A. Aesthetic Surgery Journal. 2007;27:513–517.
Westmore MG, Facial Cosmetics in Conjunction with Surgery (course presented at the Aesthetic Plastic Surgical Society Meeting, Vancouver, British Columbia, May), 1975.
[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
13 Eyebrow height / shaping
Summary and Key Features
• Eyebrow height and shape play a key role in attractiveness, emotional expression, and perceived youthfulness; the ideal brow for an individual depends on many factors
• Enhancement of brow height and contour following treatment with botulinum toxin is well documented
• The standard injection pattern in the glabella leads to inactivation of the brow depressors and portions of the frontalis; it is likely that the compensatory increase in the resting tone of the frontalis leads to brow elevation
• Brow ptosis and a ‘mephisto’ brow are the most common complications of treatment and an understanding of the relevant anatomy can help to prevent this
• Hyaluronic acid fillers can be a useful adjunct to botulinum toxin if there has been volume loss beneath the brows
• Eyebrow asymmetry is a common problem and symmetric treatment with botulinum toxin may offer a simple, non-surgical, method of correction
Eyebrows and attractiveness
The modern concept of the ideal contour of the female brow was proposed by Westmore in 1974 (Fig. 13.1). This schema applies best to an oval-shaped face, and serves as a good starting point since there is no clear definition of an ‘ideal brow’ that can be applied to all faces (Fig. 13.2). Several authors have suggested that the ideal apex of the brow is actually more lateral than the lateral limbus as Westmore had proposed. If the apex is too medial and overelevated it creates a surprised appearance.
Figure 13.2 Face shapes.
Round face – to make the face appear more oval eyebrow lines should go up. A high arched brow with a lateral apex is ideal.
Long face – horizontal eyebrows draw the eye from side to side, making the face appear more oval.
Square face – angled brows balance the strong jaw line. The apex of the brow should be above the square of the jaw if possible.
Heart-shaped face – a rounded brow adds curves, softens the appearance, and emphasizes the shape.
Diamond face – a rounded brow will soften the angular face. If the face is particularly wide a peaked brow will draw the eyes up and make the face appear more oval.
Variations to Westmore’s ideal brow have been suggested to account for variations in face shape and intercanthal distance. Baker et al confirmed that, in the case of a long face and square face, observers preferred eyebrows planned by a makeup artist who accounted for these factors, rather than the Westmore ideal (see Fig. 13.2, Box 13.1).
