CHAPTER 2 Extracorporeal Membrane Oxygenation Cannulation
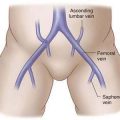
Step 1: Surgical Anatomy
Step 2: Preoperative Considerations—Patient Management before Extracorporeal Life Support
Type of Support






Cannula Considerations
Selection of Technique
Step 3: Operative Steps—Cannula Insertion for Neonatal ECLS
VV/VA Cannulation: Open Technique
Preoperative
Operation
Position of Patient
Exposure of the Carotid Sheath
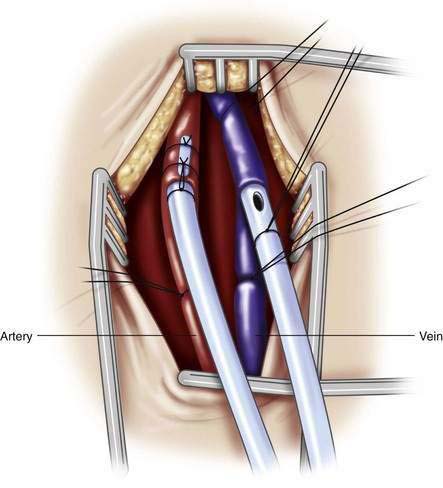
Dissection of the Vessels
Arteriotomy/Venotomy
Cannula Placement (Fig. 2-1)
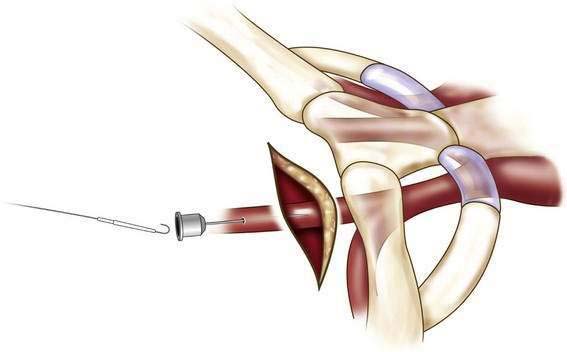
VV Cannulation: Semi-open Technique
Incision and Vein Exposure
Guidewire Placement (Fig. 2-2)
Cannula Placement (Fig. 2-3)
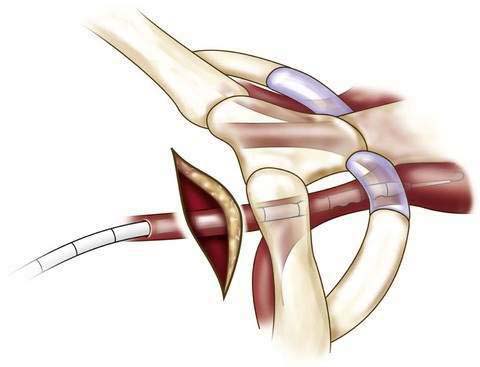
Wound Closure and Cannula Fixation
Cannula Insertion for Pediatric ECLS
Venovenous Bypass
Cannula Insertion for Adolescent ECLS
Venovenous Bypass
Venoarterial Bypass
 Jugular vein to carotid artery bypass as used in infants has been used successfully and works well, especially for combined cardiac and pulmonary support. It provides very good perfusion to all branches of the aortic arch and distal aorta, but it increases afterload by increasing aortic pressure. Ligation of the cerebral artery may cause cerebral edema.
Jugular vein to carotid artery bypass as used in infants has been used successfully and works well, especially for combined cardiac and pulmonary support. It provides very good perfusion to all branches of the aortic arch and distal aorta, but it increases afterload by increasing aortic pressure. Ligation of the cerebral artery may cause cerebral edema.




Transthoracic Cannulation
Step 4: Postoperative Care
Step 5: Pearls and Pitfalls
Difficulty Threading the Venous Cannula
Vein Division
Proximal Vein Lost in Mediastinum
Foley DS, Swaniker F, Pranikoff T, Bartlett RH, Hirschl R. Percutaneous cannulation for venovenous extracorporeal life support (ECLS). J Pediatr Surg. 2000;35:943-947.
Lazar EL, Abramson SJ, Weinstein S, et al. Neuroimaging of brain injury in neonates treated with extracorporeal membrane oxygenation: Lessons learned from serial examinations. J Pediatr Surg. 1994;29:186-191.
Miskulin J, Annich G, Grams R, et al. Venous-arteriovenous cannulation for adult ECMO patients with cardiogenic shock. 14th Annual ELSO Conference, September 10-12, 2004, Chicago, IL.
Montoya JP, Merz SI, Bartlett RH. A standardized system for describing flow/pressure relationships in vascular access devices. Trans Am Soc Artif Intern Organs. 1991;37:4-8.
Peek GJ, Firmin RK, Moore HM, et al. Cannulation of neonates for venovenous extracorporeal life support. Ann Thoracic Surg. 1996;61:1291-1292.
Pranikoff T, Hirschl RB. Neonatal extracorporeal membrane oxygenation. In Carter DC, Russell RCG, editors: Rob and Smith’s operative surgery, 6th ed, London: Butterworth-Heinemann, 2005.
Pranikoff T, Hirschl RB, Remenapp R, Swaniker F, Bartlett RH. Venovenous extracorporeal life support via percutaneous cannulation in 94 patients. Chest. 1999;115:818-822.
Pranikoff T, Hirschl RB. Neonatal extracorporeal membrane oxygenation. In Carter DC, Russell RCG, editors: Rob and Smith’s operative surgery, 5th ed, London: Butterworth-Heinemann, 1995.
Rich PB, Awad SS, Crotti S, Hirschl RB, Bartlett RH, Schreiner RJ. A prospective comparison of atrio-femoral and femoro-atrial flow in adult venovenous extracorporeal life support. J Thorac Cardiovasc Surg. 1998;116:628-632.
Schumacher RE, Barks JD, Johnston MV, et al. Right-sided brain lesions in infants following extracorporeal membrane oxygenation. Pediatrics. 1988;82:155-161.
Sinard JM, Merz SI, Hatcher MD, et al. Evaluation of extracorporeal perfusion catheters using a standardized measurement technique—the M-number. Trans Am Soc Artif Intern Organs. 1991;37:60-64.
Streltz LJ, Bej MD, Graziani LJ, et al. Utility of serial EEGs in neonates during extracorporeal membrane oxygenation. Pediatr Neurol. 1992;8:190-196.
1996 UK collaborative randomized trial of neonatal extracorporeal membrane oxygenation. UK Collaborative ECMO Trial Group. Lancet. 1996;348:75-82.
Walker LK, Short BL, Traystman RJ. Impairment of cerebral autoregulation during venovenous extracorporeal membrane oxygenation in the newborn lamb. Crit Care Med. 1996;24:2001-2006.