Exposure of the Popliteal Artery and Vein

Surgical Principles
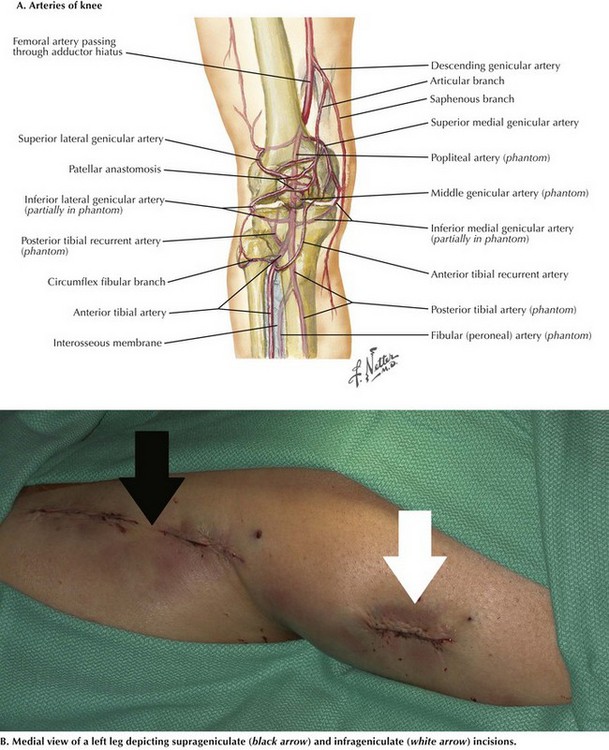
The popliteal artery begins at the adductor canal within the adductor magnus muscle (Hunter’s canal) as it enters the popliteal space behind the knee joint. The popliteal artery ends when it splits in the lower leg to become the anterior tibial artery and tibioperoneal trunk. Several important geniculate collaterals increase in caliber in cases of progressive atherosclerotic occlusion of the distal superficial femoral and popliteal arteries (Fig. 38-1, A). If an acute occlusion is present in this area, however, the collateral vessels are not sufficient and the leg is usually threatened, requiring immediate revascularization. Venous anatomy, on the other hand, is more variable.
Medial Suprageniculate Approach
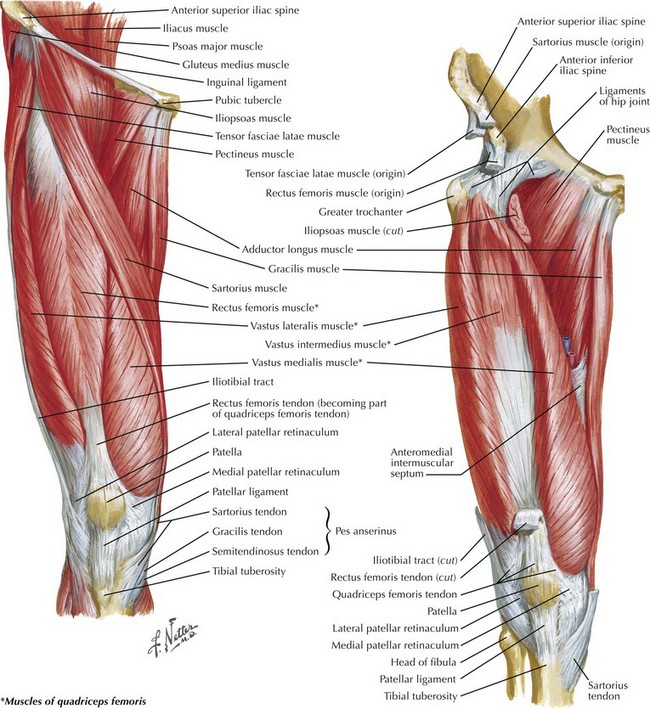
The medial suprageniculate approach is most often used in femoral-to-popliteal artery (femoropopliteal) bypass above the knee. The patient is placed in the supine position with the knee slightly flexed. An incision is made on the distal portion of the medial thigh over the estimated location of the sartorius muscle (Fig. 38-1, B).
After locating the junction between the sartorius (posterior) and vastus medialis (anterior), the surgeon places a self-retaining retractor there (Fig. 38-2).
The popliteal artery should be easily palpable below the fascia tissue between the adductor magnus and semimembranosus muscles (Fig. 38-3, A). It is important to avoid injury to any collateral arteries and veins.

Once this next fascia layer is opened, the vascular sheath containing the proximal popliteal artery and vein is seen as these vessels emerge through the canal. The adjacent popliteal vein is usually encountered first in the authors’ experience, but venous anatomy can be variable (Fig. 38-3, B). Sharp dissection is used to isolate the artery or vein proximally up to the adductor canal. Vessel loops are used to encircle the artery. The surgeon must be careful and look for a bifid popliteal vein with a second vein behind the artery; injury to the vein can lead to significant blood loss.
Medial Infrageniculate Approach
The medial infrageniculate technique is most often used in cases of femoropopliteal bypass below the knee. As for the suprageniculate approach, the patient is placed in the supine position with the knee slightly bent and the hip externally rotated. The incision is started just distal to the medial tibial plateau and runs longitudinally along the posterior border of the tibia approximately 1 fingerbreadth (see Fig. 38-1, B). This incision can be extended distally down the lower leg as needed for adequate exposure. It is important to avoid injury to the greater saphenous vein (GSV) or branches during the initial incision as it lies in the same approximate position. The GSV is often used as the bypass conduit and should be sought out first and protected during the dissection.
Next in the medial infrageniculate approach, the fascia overlying the medial head of the gastrocnemius muscle is incised and the muscle retracted posteriorly using a self-retaining retractor (see Fig. 38-3, A). Again, the vascular bundle is encountered, usually with the popliteal vein first medially. Through sharp dissection, the popliteal artery or vein is isolated, and vascular loops are placed for control. If additional length is needed, the soleus muscle can be divided from its tibial attachments distally. Alternately, the tendons of the pes anserinus (semitendinosus, gracilis, and sartorius muscles) can be temporarily divided proximally, but care must be taken to reattach these tendons after completion of the procedure for knee stability.
Posterior Approach
Best used for treatment of trauma, aneurysms, cystic adventitial disease, and popliteal entrapment syndrome, the posterior approach begins with the patient in the prone position. A lazy S-shaped incision is made to prevent debilitating wound-healing contracture across a mobile joint. Starting at the proximal medial aspect of the lower thigh along the muscle bodies of the semimembranosus and semitendinosus, the surgeon carries the incision down to the popliteal crease and crosses it horizontally from medial to lateral, then down distally along the lateral calf (Fig. 38-4, A). At this point, the small (short) saphenous vein is encountered and ligated or harvested for bypass, if it is of adequate size (Fig. 38-4, B).
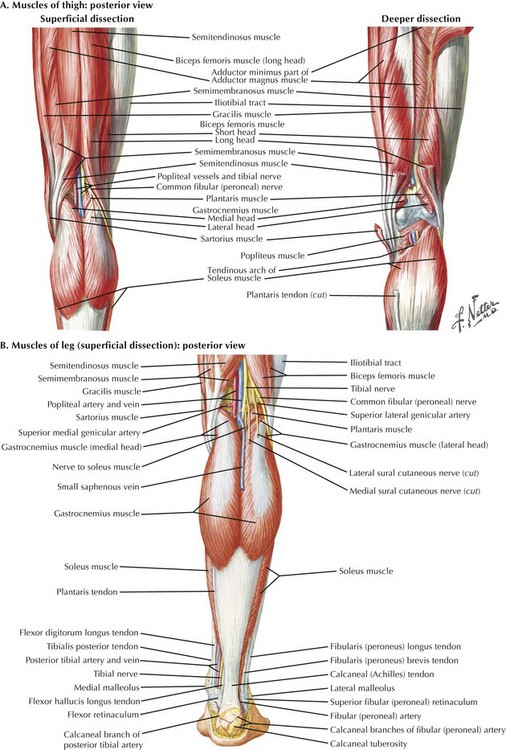
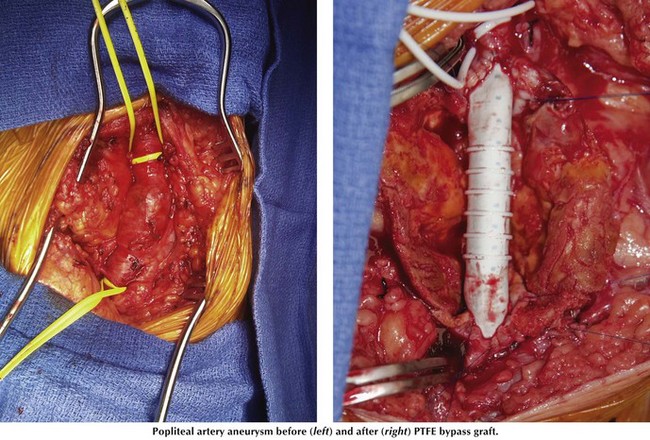
Figure 38-5 provides an example of a popliteal artery aneurysm and subsequent bypass with polytetrafluoroethylene (PTFE) using the posterior approach.
Gelabert, HA, Colburn, MD, Machleder, HI. Posterior exposure of the popliteal artery in reoperative vascular surgery. Ann Vasc Surg. 1996;10(1):53–58.
Kropman, RH, van Santvoort, HC, Teijink, J, et al. The medial versus the posterior approach in the repair of popliteal artery aneurysms: a multicenter case-matched study. J Vasc Surg. 2007;46(1):24–30.
Norgren, L, Hiatt, WR, Dormandy, JA, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). J Vasc Surg. 2007;45(Suppl):S5–7.
Ziegler, KR, Muto, A, Eghbalieh, SD, Dardik, A. Basic data related to surgical infrainguinal revascularization procedures: a twenty year update. Ann Vasc Surg. 2011;25(3):413–422.






