• Transjugular intrahepatic portosystemic shunt (TIPS) provides more physiological means of treating varices and ascites than other surgical procedures
(Left) Graphic shows dilated, tortuous, submucosal collateral veins (varices) within the wall of the esophagus.
(Right) Double-contrast esophagram shows tortuous, nodular longitudinal folds, typical of varices. These are unusually well depicted, even with the esophageal lumen distended, suggesting that the varices may be thrombosed or sclerosed by endoscopic injection.
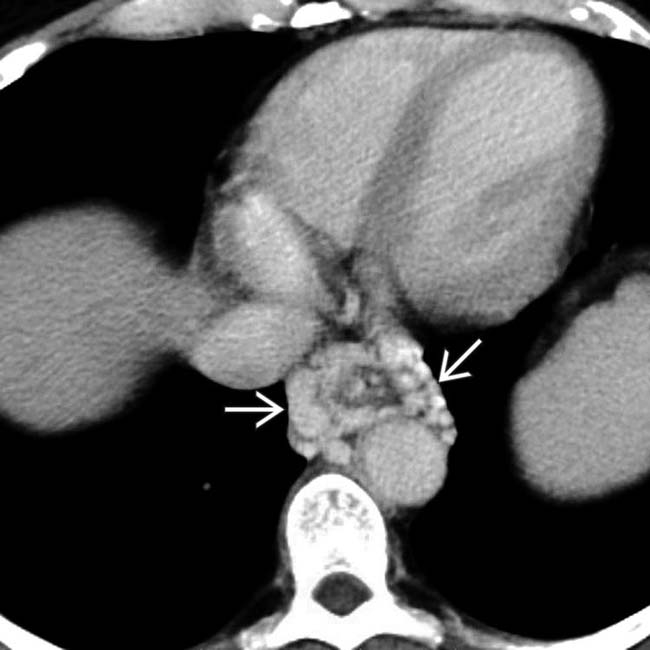
(Left) Axial CECT in a 55-year-old man with upper GI bleeding shows large esophageal varices .
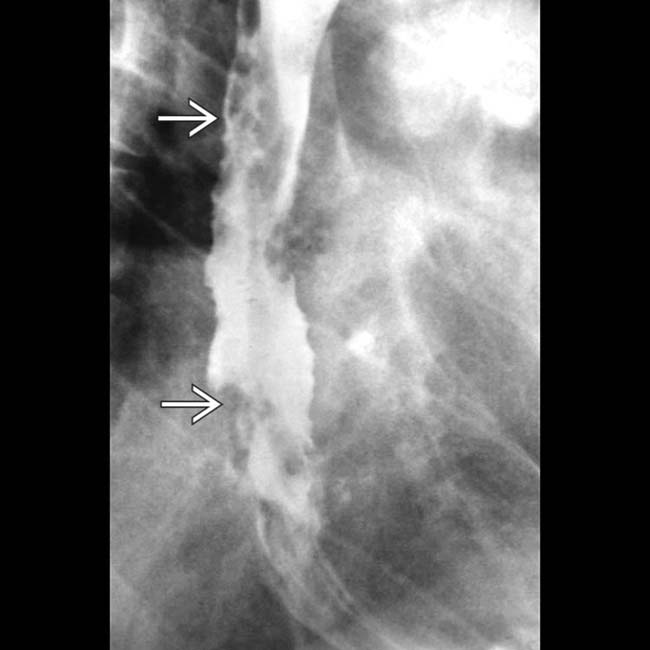
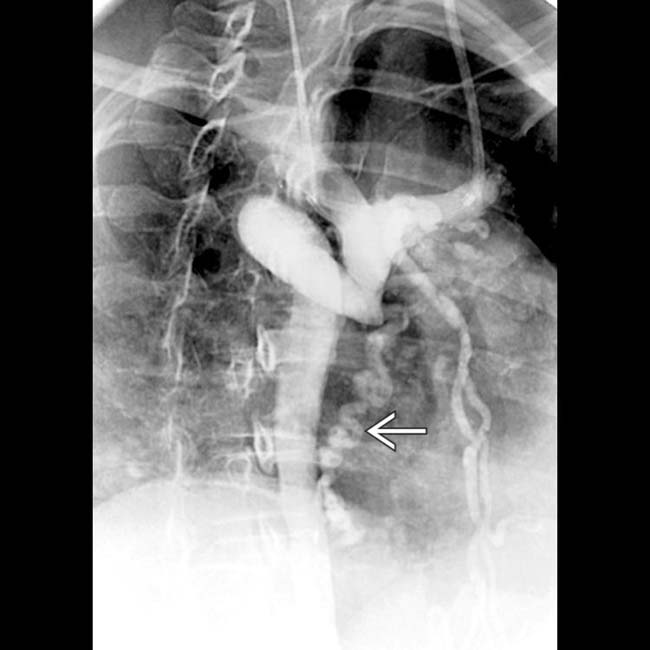
(Right) Esophagram in the same patient performed after endoscopic sclerosis of the varices shows fixed filling defects in the esophageal wall and lumen. The fixed nature of these mimics the appearance of the “varicoid” morphology of some esophageal carcinomas.
TERMINOLOGY
Definitions
• Dilated tortuous submucosal venous plexus of esophagus
IMAGING
General Features
• Best diagnostic clue
Tortuous or serpiginous longitudinal filling defects on esophagography
• Location
Uphill varices: Distal 1/3 or 1/2 of esophagus (more common)
Downhill varices: Upper or middle 1/3 of esophagus (less common)
• Morphology
Tortuous dilated veins in long axis of esophagus, protruding directly beneath mucosa or in periesophageal tissue
• Other general features
Usually due to portal hypertension (HTN) with cirrhosis or other liver diseases
Idiopathic varices: In patients with no portal HTN or superior vena cava (SVC) block (very rare)
Classification of esophageal varices based on pathophysiology
– Uphill varices: ↑ portal venous pressure → upward venous flow via dilated esophageal collaterals to SVC
– Downhill varices: Obstruction of SVC → downward venous flow via esophageal collaterals to portal vein and inferior vena cava (IVC)
Radiographic Findings
• Radiography
Chest radiograph
– Retrocardiac posterior mediastinal lobulated mass
– Commonly see spontaneous shunts develop between varices and systemic veins
Left renal > gonadal > other intra- and retroperitoneal veins
– Mesenteric varices
Commonly form around ostomy sites in patients with portal hypertension (e.g., patient with cirrhosis due to primary sclerosing cholangitis whose ulcerative colitis was treated with colectomy)
MR Findings
• T1WI and T2WI
Multiple areas of flow void
• T1WI C+
Portal venous phase (PVP)
– Enhancement of varices seen
Ultrasonographic Findings
• Grayscale ultrasound
Increased esophageal wall thickness at least 5 mm with irregular wall surface
• Color Doppler
Hepatofugal venous flow within esophageal wall
Angiographic Findings
• Conventional
Portal venogram
– Uphill varices: May show cavernous transformation of portal vein and reversal of blood flow via splenic vein → coronary vein → esophageal varices
Imaging Recommendations
• Helical NE + CECT
• Fluoroscopic-guided esophagography
Position: Prone right anterior oblique (RAO)
Mucosal relief views; avoid repetitive swallowing
DIFFERENTIAL DIAGNOSIS
Esophageal Carcinoma
• May simulate varices
• Varicoid carcinoma
Produce thickened, tortuous folds in esophagus due to submucosal spread of tumor
(Left) Axial CECT in a middle-aged man with cirrhosis demonstrates cirrhosis but relatively small esophageal varices. The portal vein was thrombosed (not shown).
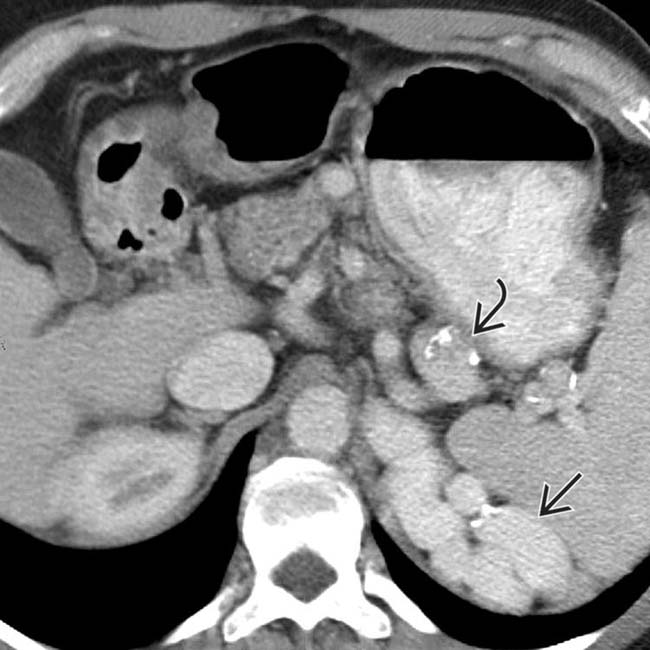
(Right) Axial CECT in the same patient shows large perisplenic varices and calcification present in the walls of some varices that might be mistaken for arterial aneurysms.
(Left) Axial CECT in the same patient shows a spontaneous splenorenal shunt with enlargement of the left renal vein . Spontaneous or surgically created shunts help to decompress esophageal varices but increase the incidence of encephalopathy and portal vein thrombosis, making subsequent liver transplantation difficult or impossible.
(Right) Celiac arteriogram in the same patient shows opacification of the splenic vein and varices but no portal vein flow.
(Left) Axial CECT in an elderly woman presenting with a puffy face shows obstruction of superior vena cava (SVC) with collateral flow through an enlarged azygous vein and various mediastinal collateral veins.
(Right) Coronal CECT (same patient) shows enlarged azygous vein and mediastinal collateral veins . The collaterals are carrying flow from tributaries of the SVC into abdominal circulation to be returned to the heart via the inferior vena cava (IVC). These are sometimes referred to as “downhill varices.”
Axial CECT in a cirrhotic patient shows massive varices as tortuous enhanced vessels in the periesophageal region.
Axial CECT in the same patient shows massive varices in the gastric fundus wall.
Esophagram shows serpiginous submucosal filling defects in the proximal 1/2 of the esophagus; downhill varices.
Catheter venacavogram shows obstruction of the superior vena cava. The SVC is occluded above the azygous arch. Downhill varices in the periesophageal region are part of collateral venous drainage.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Distal 1/3 or 1/2 of esophagus
More common
• Downhill varices: Obstruction of SVC → downward venous flow via esophageal collaterals to portal vein and inferior vena cava (IVC)
Upper or middle 1/3 of esophagus
Less common
• Fluoroscopy: Tortuous, serpiginous, longitudinal radiolucent filling defects in collapsed or partially collapsed esophagus
After sclerotherapy varices may appear as fixed, rigid filling defects
• CECT: Serpiginous periesophageal, gastric, etc.
Enhance as other abdominal veins
Esophageal, coronary ± paraumbilical: Most commonly visualized
TOP DIFFERENTIAL DIAGNOSES
• Esophageal (varicoid) carcinoma
Thickened, tortuous folds due to submucosal spread of tumor
• Transjugular intrahepatic portosystemic shunt (TIPS) provides more physiological means of treating varices and ascites than other surgical procedures
(Left) Graphic shows dilated, tortuous, submucosal collateral veins (varices) within the wall of the esophagus.
(Right) Double-contrast esophagram shows tortuous, nodular longitudinal folds, typical of varices. These are unusually well depicted, even with the esophageal lumen distended, suggesting that the varices may be thrombosed or sclerosed by endoscopic injection.
(Left) Axial CECT in a 55-year-old man with upper GI bleeding shows large esophageal varices .
(Right) Esophagram in the same patient performed after endoscopic sclerosis of the varices shows fixed filling defects in the esophageal wall and lumen. The fixed nature of these mimics the appearance of the “varicoid” morphology of some esophageal carcinomas.
TERMINOLOGY
Definitions
• Dilated tortuous submucosal venous plexus of esophagus
IMAGING
General Features
• Best diagnostic clue
Tortuous or serpiginous longitudinal filling defects on esophagography
• Location
Uphill varices: Distal 1/3 or 1/2 of esophagus (more common)
Downhill varices: Upper or middle 1/3 of esophagus (less common)
• Morphology
Tortuous dilated veins in long axis of esophagus, protruding directly beneath mucosa or in periesophageal tissue
• Other general features
Usually due to portal hypertension (HTN) with cirrhosis or other liver diseases
Idiopathic varices: In patients with no portal HTN or superior vena cava (SVC) block (very rare)
Classification of esophageal varices based on pathophysiology
– Uphill varices: ↑ portal venous pressure → upward venous flow via dilated esophageal collaterals to SVC
– Downhill varices: Obstruction of SVC → downward venous flow via esophageal collaterals to portal vein and inferior vena cava (IVC)
Radiographic Findings
• Radiography
Chest radiograph
– Retrocardiac posterior mediastinal lobulated mass












 .
.
 in the esophageal wall and lumen. The fixed nature of these mimics the appearance of the “varicoid” morphology of some esophageal carcinomas.
in the esophageal wall and lumen. The fixed nature of these mimics the appearance of the “varicoid” morphology of some esophageal carcinomas.




















































 and calcification present
and calcification present  in the walls of some varices that might be mistaken for arterial aneurysms.
in the walls of some varices that might be mistaken for arterial aneurysms.
 . Spontaneous or surgically created shunts help to decompress esophageal varices but increase the incidence of encephalopathy and portal vein thrombosis, making subsequent liver transplantation difficult or impossible.
. Spontaneous or surgically created shunts help to decompress esophageal varices but increase the incidence of encephalopathy and portal vein thrombosis, making subsequent liver transplantation difficult or impossible.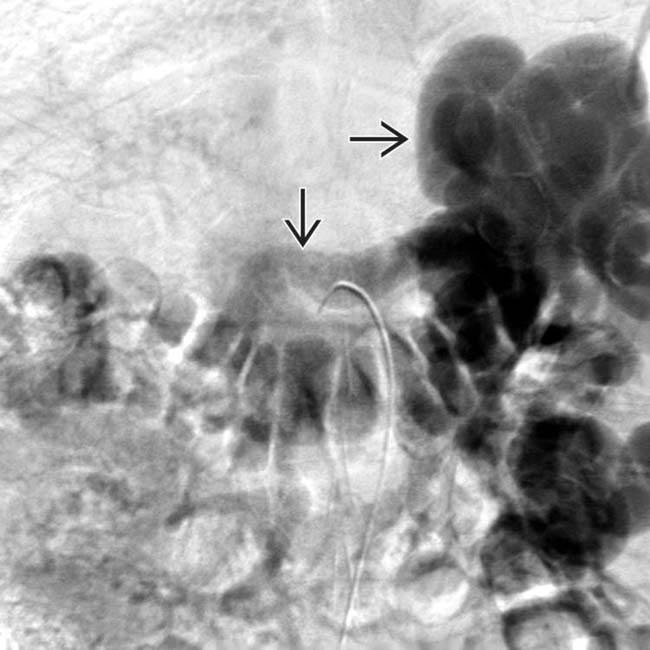
 but no portal vein flow.
but no portal vein flow.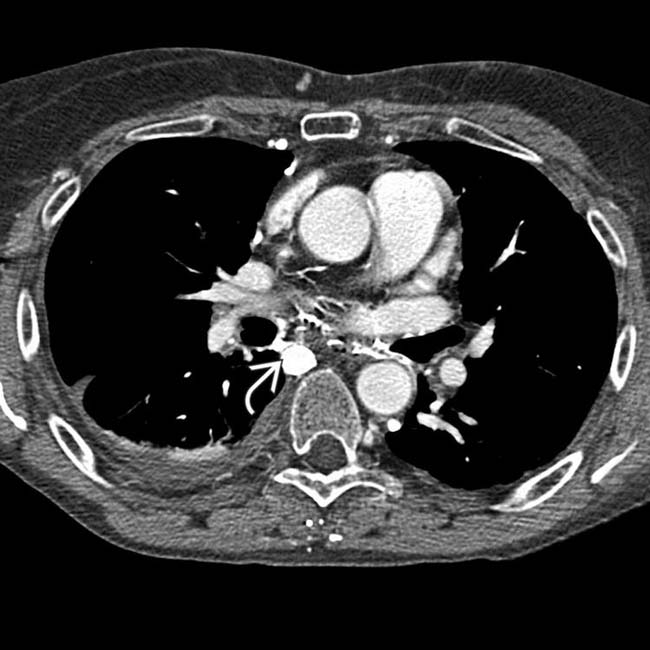
 and various mediastinal collateral veins.
and various mediastinal collateral veins.
 and mediastinal collateral veins
and mediastinal collateral veins  . The collaterals are carrying flow from tributaries of the SVC into abdominal circulation to be returned to the heart via the inferior vena cava (IVC). These are sometimes referred to as “downhill varices.”
. The collaterals are carrying flow from tributaries of the SVC into abdominal circulation to be returned to the heart via the inferior vena cava (IVC). These are sometimes referred to as “downhill varices.”

 in the gastric fundus wall.
in the gastric fundus wall.
 in the periesophageal region are part of collateral venous drainage.
in the periesophageal region are part of collateral venous drainage. Location
Location
