[level-membership-for-pediatrics-category]
CHAPTER 8 Esophageal Replacement
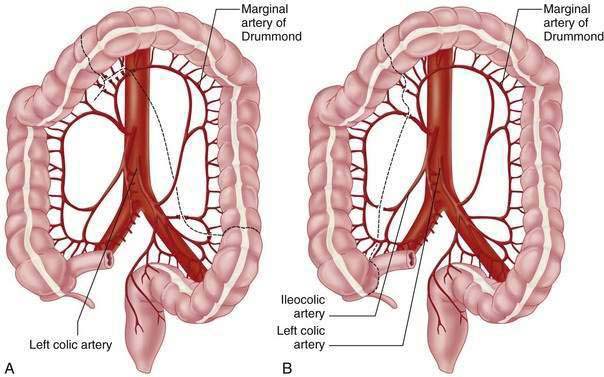
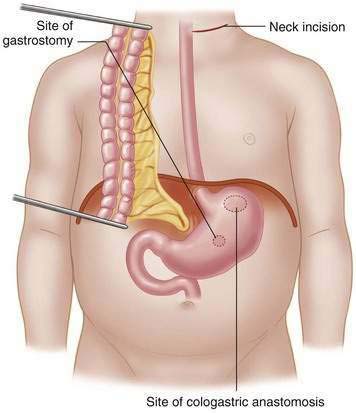
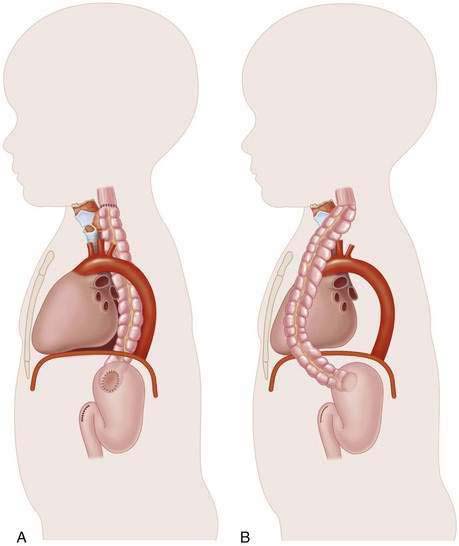
Colonic Interposition
Step 1: Surgical Anatomy
Step 2: Preoperative Considerations
Step 3: Operative Steps
Incision
Step 4: Postoperative Care



Step 5: Pearls and Pitfalls
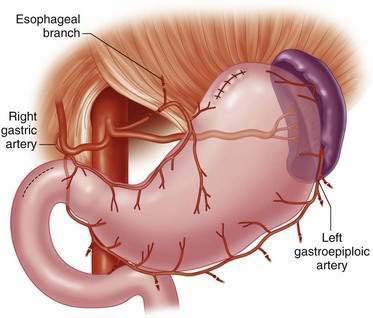
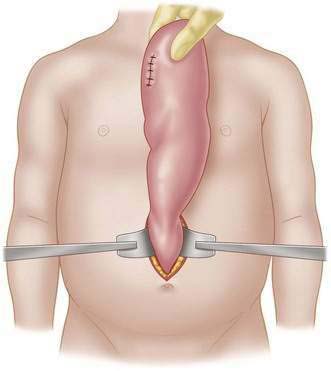
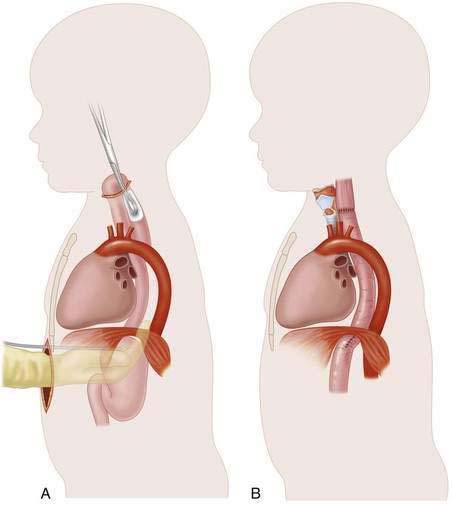
Gastric Transposition
Step 1: Surgical Anatomy
Step 2: Preoperative Considerations
Step 3: Operative Steps
Incision


Step 5: Pearls and Pitfalls
Ahmed A, Spitz L. The outcome of colonic replacement of the esophagus in children. Progr Pediatr Surg. 1986;19:37-54.
Ahmad SA, Sylvester JG, Hebra A, et al. Esophageal replacement using the colon: Is it a good choice? J Pediatr Surg. 1996;31:1026-1031.
Anderson KD, Noblett H, Belsey R, Randolph JG. Long-term follow-up of children with colon and gastric tube interposition for esophageal atresia. Surgery. 1992;1111:131-136.
Azar H, Chrispin AR, Waterston DJ. Esophageal replacement with transverse colon in infants and children. J Pediatr Surg. 1971;66:333-342.
Choi RS, Lillehei CW, Lund DP, et al. Esophageal replacement in children who have caustic pharyngoesophageal strictures. J Pediatr Surg. 1971;6:3-9.
Gross RE, Firestone FN. Colonic reconstruction of the esophagus in infants and children. Surgery. 1967;61:955-964.
Kelly JP, Shackelford GD, Roper CL. Esophageal replacement with colon in children; functional results and long-term growth. Ann Thorac Surg. 1983;36:634-643.
Poppeo E, Coosemans W, De Leyn P, Denette G, Van Raemdonck D, Lerut T. Esophageal replacement with colon in children using either the intrathoracic or retrosternal route: an analysis of both surgical and long-term results. Surg Today. 1997;27:729-734.
West KW, Vane DW, Grosfeld JL. Esophageal replacement in children: Experience with thirty-one cases. Surgery. 1986;100:751-757.
[/level-membership-for-pediatrics-category][not-level-membership-for-pediatrics-category]
CHAPTER 8 Esophageal Replacement
Colonic Interposition
Step 1: Surgical Anatomy
Step 2: Preoperative Considerations
Step 3: Operative Steps
Incision
[/not-level-membership-for-pediatrics-category]
