[level-membership-for-radiology-category] Dysphagia, weight loss, hematemesis, or asymptomatic
• Esophageal metastases
Direct, lymphatic, or hematogenous spread
Direct invasion most common route: Gastric and lung cancer most common primary tumors
• Complications
GI bleeding, perforation, obstruction
• Treatment
Chemotherapy; radiation therapy
Surgical resection of complicating lesions (obstruction, upper GI bleed)
Endoluminal stent for obstructing lesions
• Prognosis
Usually poor
DIAGNOSTIC CHECKLIST
• Check for history of primary extraesophageal cancer; biopsy required
• Overlapping radiographic features of esophageal metastases, lymphoma, and primary carcinoma
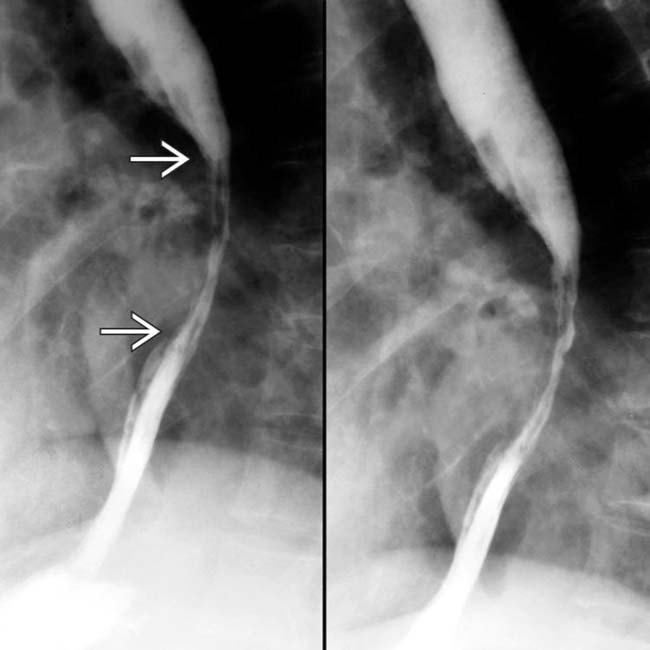
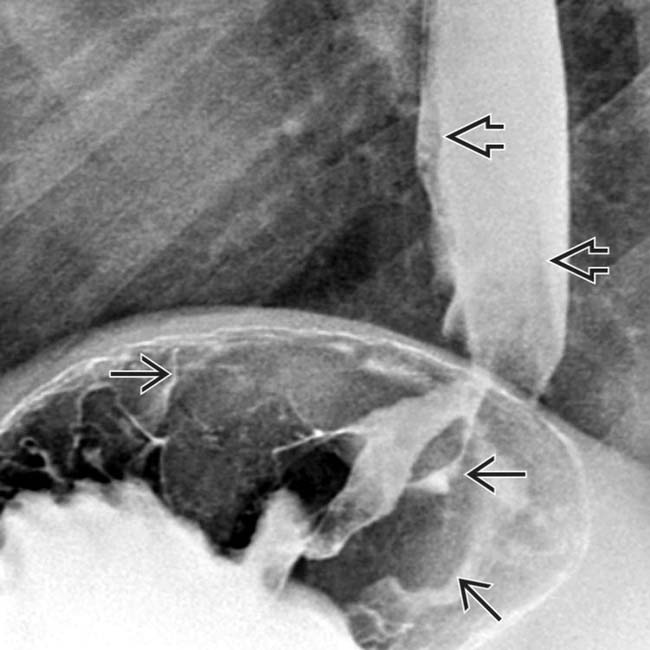
(Left) In this 60-year-old woman with lung cancer and progressive dysphagia, 2 views from an esophagram show extrinsic or intramural narrowing of the mid esophagus , but intact mucosal folds, representing invasion by her lung cancer.
(Right) Esophagram in a man with known lung cancer and dysphagia shows a broad shelf-like indentation along the anterior wall of the mid esophagus.
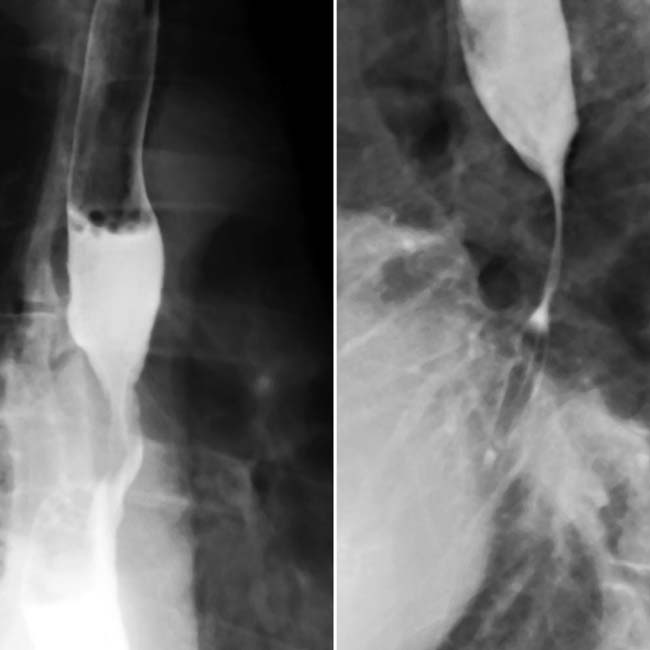
(Left) In this 62-year-old man, a spot film of the distal esophagus shows a distal stricture and mucosal irregularity that mimics primary esophageal cancer. However, other views (not shown) showed nodular thickened folds in the gastric fundus.
(Right) CT in the same patient shows a mass within the wall of the fundus with extension into the perigastric tissues and nodes. Endoscopy confirmed a primary gastric carcinoma.
TERMINOLOGY
Definitions
• Metastases from primary cancer of other sites
• Lymphoma: Malignant tumor of lymphocytes
IMAGING
General Features
• Best diagnostic clue
From gastric cancer: Ulcerated/polypoid mass of gastric cardia extending into distal esophagus
From lung cancer: Extrinsic indentation of upper esophagus from primary cancer or malignant adenopathy
Radiographic Findings
• Fluoroscopic-guided double-contrast barium study
Direct invasion, gastric carcinoma: Distal esophagus
– Ulcerated/polypoid mass of cardia/fundus
– Irregular or smooth, tapered narrowing of distal esophagus ± discrete mass
Direct invasion of cancer of larynx, pharynx, thyroid, lung: Cervical or thoracic esophagus
– Smooth or slightly irregular esophageal wall, soft tissue mass in adjacent neck/mediastinum
– Serrated, scalloped, or nodular esophageal wall → narrowing/obstruction
– Thyroid cancer: Expansile intraluminal mass
Contiguous involvement by mediastinal nodes (breast, lung cancer): Mid esophagus
– Smooth, lobulated esophageal indentation or ulceration at level of carina
Usually in older adults (same demographics as for primary extraesophageal cancer)
Esophageal lymphoma
– Least common site within GI tract (1% of cases)
– Usually NHL, less commonly Hodgkin
– Secondary lymphoma (90%) > > primary (10%)
– Primary esophageal lymphoma seen in AIDS
Natural History & Prognosis
• Complications: GI bleeding, perforation, obstruction
• Prognosis: Usually poor
Treatment
• Chemotherapy; radiation therapy
• Endoluminal stent for obstructing lesions
DIAGNOSTIC CHECKLIST
Consider
• Check for history of primary extraesophageal cancer; biopsy required
Image Interpretation Pearls
• Overlapping radiographic features of esophageal metastases, lymphoma, and primary carcinoma
• Imaging important to identify and stage malignancy
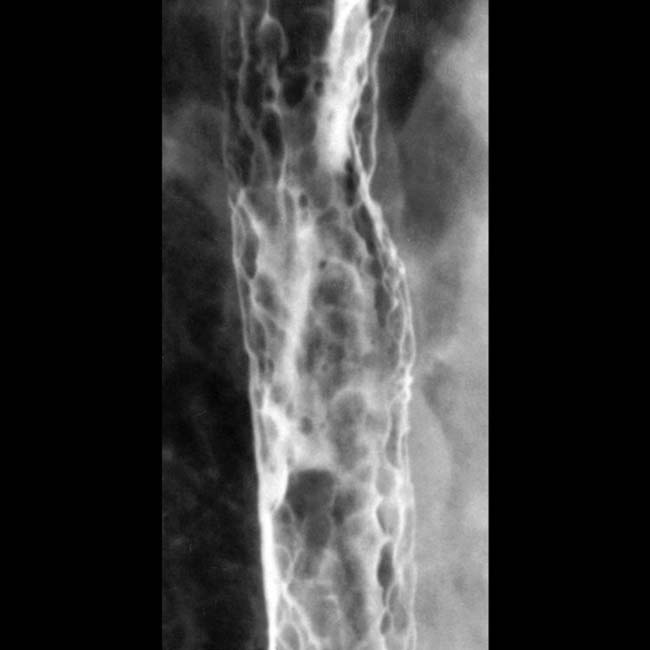
Esophagram shows innumerable submucosal nodules, 3-10 mm in size, due to lymphoma. (Courtesy M. Levine, MD.)
Esophagram shows smooth stricture of the mid esophagus due to direct invasion by lung cancer.
Axial CECT shows gastric carcinoma in the fundus extending cephalad into the esophagus .
Upper GI series shows a mass in the gastric fundus extending cephalad into the esophagus in this patient with gastric carcinoma.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Dysphagia, weight loss, hematemesis, or asymptomatic
• Esophageal metastases
Direct, lymphatic, or hematogenous spread
Direct invasion most common route: Gastric and lung cancer most common primary tumors
• Complications
GI bleeding, perforation, obstruction
• Treatment
Chemotherapy; radiation therapy
Surgical resection of complicating lesions (obstruction, upper GI bleed)
Endoluminal stent for obstructing lesions
• Prognosis
Usually poor
DIAGNOSTIC CHECKLIST
• Check for history of primary extraesophageal cancer; biopsy required
• Overlapping radiographic features of esophageal metastases, lymphoma, and primary carcinoma
(Left) In this 60-year-old woman with lung cancer and progressive dysphagia, 2 views from an esophagram show extrinsic or intramural narrowing of the mid esophagus , but intact mucosal folds, representing invasion by her lung cancer.
(Right) Esophagram in a man with known lung cancer and dysphagia shows a broad shelf-like indentation along the anterior wall of the mid esophagus.
(Left) In this 62-year-old man, a spot film of the distal esophagus shows a distal stricture and mucosal irregularity that mimics primary esophageal cancer. However, other views (not shown) showed nodular thickened folds in the gastric fundus.
(Right) CT in the same patient shows a mass within the wall of the fundus with extension into the perigastric tissues and nodes. Endoscopy confirmed a primary gastric carcinoma.
TERMINOLOGY
Definitions
• Metastases from primary cancer of other sites
• Lymphoma: Malignant tumor of lymphocytes
IMAGING
General Features
• Best diagnostic clue
From gastric cancer: Ulcerated/polypoid mass of gastric cardia extending into distal esophagus
From lung cancer: Extrinsic indentation of upper esophagus from primary cancer or malignant adenopathy
Radiographic Findings
• Fluoroscopic-guided double-contrast barium study
Direct invasion, gastric carcinoma: Distal esophagus
– Ulcerated/polypoid mass of cardia/fundus
– Irregular or smooth, tapered narrowing of distal esophagus ± discrete mass
Direct invasion of cancer of larynx, pharynx, thyroid, lung: Cervical or thoracic esophagus
– Smooth or slightly irregular esophageal wall, soft tissue mass in adjacent neck/mediastinum
–
Buy Membership for Radiology Category to continue reading. Learn more here







 , but intact mucosal folds, representing invasion by her lung cancer.
, but intact mucosal folds, representing invasion by her lung cancer.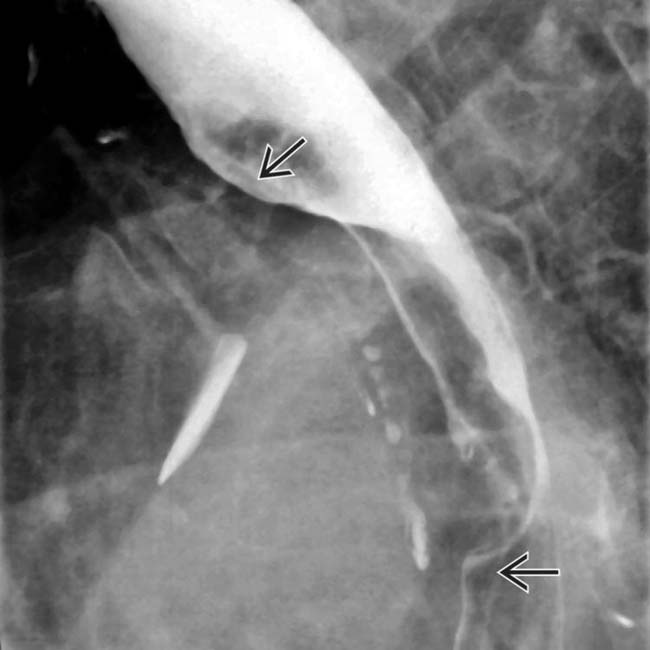
 along the anterior wall of the mid esophagus.
along the anterior wall of the mid esophagus.
 that mimics primary esophageal cancer. However, other views (not shown) showed nodular thickened folds in the gastric fundus.
that mimics primary esophageal cancer. However, other views (not shown) showed nodular thickened folds in the gastric fundus.
 within the wall of the fundus with extension into the perigastric tissues and nodes. Endoscopy confirmed a primary gastric carcinoma.
within the wall of the fundus with extension into the perigastric tissues and nodes. Endoscopy confirmed a primary gastric carcinoma.


















 extending cephalad into the esophagus
extending cephalad into the esophagus  .
.
 in the gastric fundus extending cephalad into the esophagus
in the gastric fundus extending cephalad into the esophagus  in this patient with gastric carcinoma.
in this patient with gastric carcinoma. Direct invasion of cancer of larynx, pharynx, thyroid, lung: Cervical or thoracic esophagus
Direct invasion of cancer of larynx, pharynx, thyroid, lung: Cervical or thoracic esophagus
