(Left) Barium esophagram shows complete obstruction of the esophageal lumen and a filling defect representing an incompletely chewed piece of meat. Following removal, a Schatzki ring was found.
(Right) This 1-year-old child swallowed a watch battery , which is lodged in the cervical esophagus. Note the smooth outer contour that distinguishes it from the serrated surface of a coin. The coin was removed, but resulted in a persistent stricture of the esophagus.
(Left) Esophagram demonstrates the outline of a plastic comb impacted in the distal esophagus and extending into the stomach. On first impression, this might be misinterpreted as an esophageal stent that had been placed across an obstructing esophageal lesion.
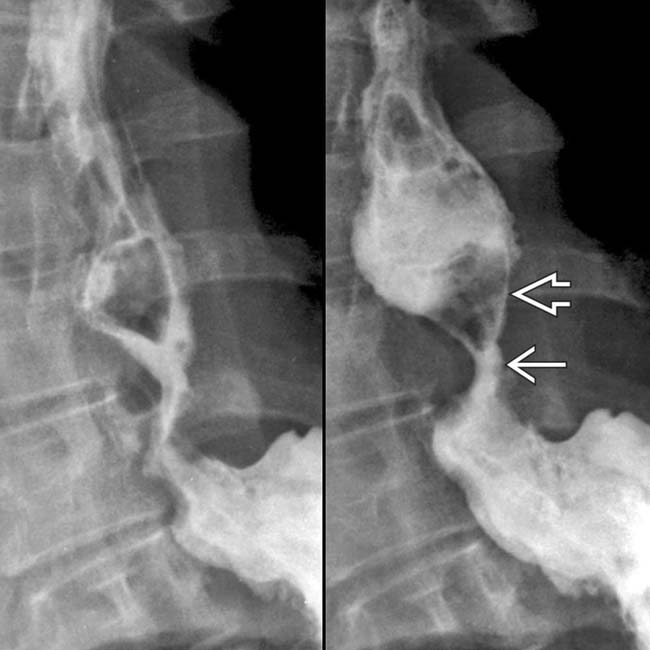
(Right) Oblique esophagram following endoscopic removal of a foreign body shows extravasation of contrast medium and free air within the abdomen . Surgical repair was required.
TERMINOLOGY
Abbreviations
• Esophageal foreign body (FB)
Definitions
• Ingested FB impacted within esophagus
IMAGING
General Features
• Best diagnostic clue
History of ingestion followed by dysphagia or odynophagia
• Location
Gastroesophageal junction: Area of indentation by aortic arch or left main bronchus
Above preexisting stricture, Schatzki ring, or tumor
Bones tend to lodge in cervical esophagus, just below level of cricopharyngeus muscle (C6 level)
• Size
Smooth objects measuring < 1-2 cm in diameter usually pass uneventfully
• Morphology
Radiolucent: Food, plastic, wood, medication, etc.
Radiopaque: Coin, battery, pin, nail, needle, etc.
Sharp or dull, pointed or blunt, toxic or nontoxic
Radiographic Findings
• Radiography
Lateral neck radiograph: Radiopaque FB
– Ingested bone fragments: Linear or slightly curved densities with well-defined margins
• Surgical removal: Rarely indicated for complications
Esophagram shows an intramural mass effect in the distal esophagus due to an ingested chicken bone that was imbedded in the wall, causing an inflammatory reaction.
Esophagram shows complete obstruction of the mid esophagus with a meniscus of barium outlining a piece of ingested meat, impacted above a stricture in Barrett esophagus.
Esophagrams show a hiatal hernia with a peptic stricture . The foreign body , a walnut, is impacted above the stricture.
Esophagram shows complete obstruction of the esophagus with distal filling defect due to ingested meat. After endoscopic removal of the foreign body, a Schatzki ring was found.












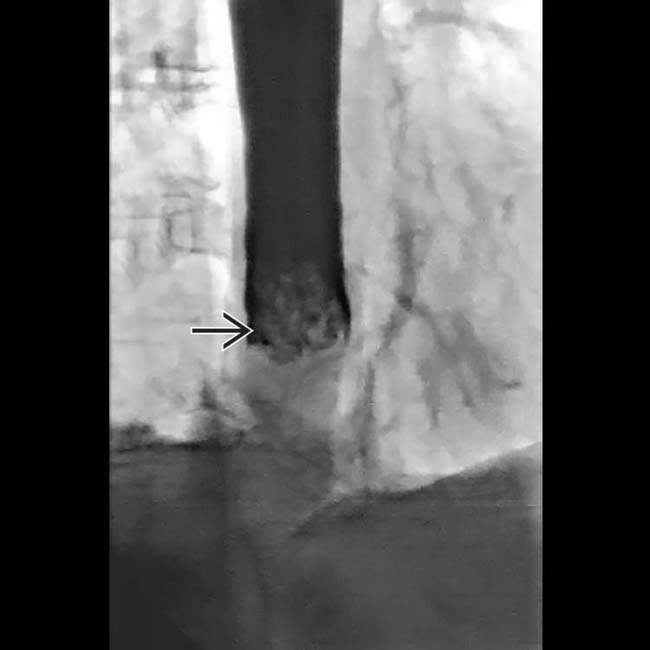
 representing an incompletely chewed piece of meat. Following removal, a Schatzki ring was found.
representing an incompletely chewed piece of meat. Following removal, a Schatzki ring was found.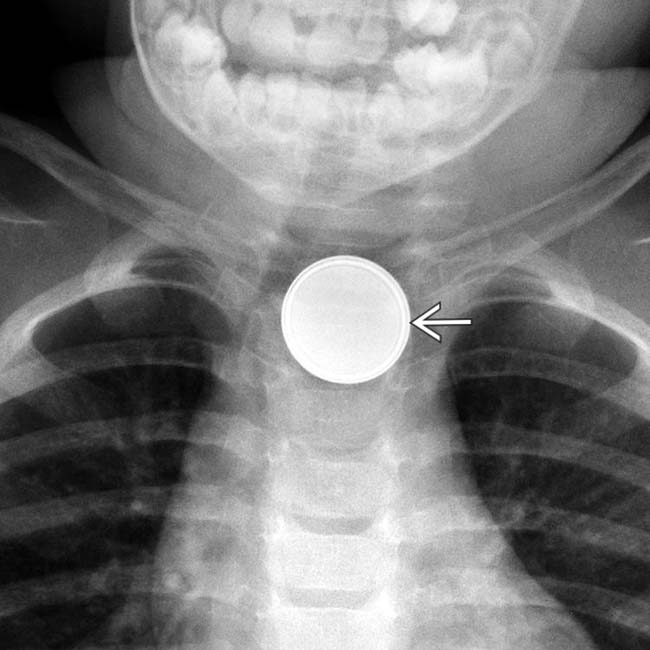
 , which is lodged in the cervical esophagus. Note the smooth outer contour that distinguishes it from the serrated surface of a coin. The coin was removed, but resulted in a persistent stricture of the esophagus.
, which is lodged in the cervical esophagus. Note the smooth outer contour that distinguishes it from the serrated surface of a coin. The coin was removed, but resulted in a persistent stricture of the esophagus.

 and free air within the abdomen
and free air within the abdomen  . Surgical repair was required.
. Surgical repair was required.




























 . The foreign body
. The foreign body  , a walnut, is impacted above the stricture.
, a walnut, is impacted above the stricture.


