Vesicles on nose of child with EPP.

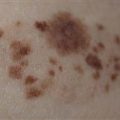
Thickened papules over the dorsal hand of a 12-year-old girl with EPP.
CLINICAL FEATURES
EPP presents in the preschool child as stinging, burning or itching of the skin, often within minutes of sun exposure. Despite the symptoms, skin changes are frequently not seen. Intense sun exposure may result in facial edema, erythema, urticaria, vesiculation and crusting. Vesicular injury may cause pitted scarring. Most children will present with chronic changes of slightly thickened skin-colored papules over the dorsa of the hands, nose and cheeks. Mild anemia may be seen in 25%. Cholelithiasis and abnormal liver function tests occur in 25%. Up to 5% of affected individuals will progress to liver failure, usually after age 30 years. EPP is caused by compound heterozygosity of the gene encoding for ferrochelatase. Lack of ferrochelatase function leads to failure of protoporphyrin incorporation into heme and thus to protoporphyrin accumulation. Visible 409-nm light reacts with the protoporphyrin in the skin, leading to the symptoms.
TREATMENT
Sun exposure minimization, the wearing of broad-brimmed hats, long-sleeved and long-legged clothing along with oral beta-carotene is the management of choice. In children, a dosage of 40–120 mg/day resulting in a beta-carotene serum level of 600–800 µg/100 mL is desired. Conventional sunscreens should be used as an adjunct, but are ineffective as sole treatment. Liver function tests should be monitored and, if abnormal, referral to a liver specialist is required.