8 Equipment guidelines
Pearls and pitfalls
Resuscitation equipment
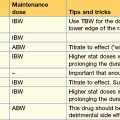
Endotracheal tubes – cuffed vs. uncuffed
• helps to prevent aspiration of gastric contents
• prevents the leakage of ventilation past the ETT leading to gastric insufflation
• the use of the exact size is less important than with an uncuffed tube.
Bag–valve resuscitator
The bag–valve resuscitator must be tested before use. This can be done in the following easy steps:
1. Place a hand underneath the patient-connection end.
2. Squeeze the self-inflating portion of the bag and check that air is expelled.
3. Seal the patient-connection end with the palm of your hand.
4. Squeeze the self-inflating portion of the bag and check that there is no leakage in the rest of the bag.
5. If a pop-off valve is present, perform the abovementioned steps first with the valve open, and secondly with the valve closed.
6. Lastly, the reservoir should be attached to the patient-connection end and held in place while the self-inflating portion of the bag is squeezed repeatedly. This should inflate the reservoir bag completely, and reveal any leaks in the reservoir. This also exposes any fault with the one-way non-return valve of the bag–valve resuscitator: if the reservoir inflates and deflates, this may indicate that the one-way valve is dysfunctional.

Normal vital signs
With reference to the Charts in Chapter 5.
Average BP
This is the average expected BP for a patient. It is the 50th percentile for expected age.
Minimum BP
• <60 mmHg in term neonates (0 to 28 days).
• <70 mmHg in infants (1 month to 12 months).
Recent data suggest using 65 mmHg instead of 70 mmHg for children 1–10 years of age.
Initial ventilator settings
Pressure support/assisted spontaneous breath and peak inspiratory pressure
Some ventilators work on the following principle:

where the PS/ASB would be equivalent to the driving pressure.