5
Endurance Training
1. Recognize the differences between muscular and cardiovascular endurance.
2. Define activities/exercises that are aerobic or anaerobic.
3. Describe benefits associated with cardiovascular fitness training.
4. Compare moderate- and vigorous-intensity exercises.
5. Describe methods to measure exercise intensity.
6. Describe the role of aerobic exercise for patients with an orthopedic injury.
7. Define the training parameters to improve muscular endurance.
CARDIOVASCULAR TRAINING
Energy Metabolism for Aerobic Training
The catabolism of macronutrients (carbohydrates, proteins, and fats) creates energy for the human body. These fuel sources are ultimately converted into adenosine triphosphate (ATP), the main energy source for muscular function. Three metabolic pathways (Box 5-1) in the human body are responsible for the production of ATP. Energy metabolism may occur either with (aerobic metabolism) or without (anaerobic metabolism) the presence of oxygen.



When an endurance-based activity is initiated, the initial production of ATP is supplied by the ATP-creatine phosphate (ATP-CP) and the glycolysis systems. The ATP-CP system can only provide enough ATP for approximately 15 seconds of activity and the glycolysis system can only supply up to an additional 2 minutes worth of ATP. Continuation of an endurance-based activity requires the constant supply of oxygen for the body to continue to produce ATP.2,11,25 The oxidative system produces approximately 19 times the ATP (38 to 39 ATP, dependent upon the fuel substrate) as produced by the phosphagen energy system (2 ATP).11,25
Benefits of Cardiovascular Fitness Training
More than 60% of adults in the United States are considered either overweight or obese.16,21 Obesity is a leading risk factor for developing heart disease, diabetes, hypertension, and some cancers. Obesity may also contribute to the development of certain musculoskeletal injuries.15 An individual with a chronic disease who initiates an aerobic exercise program may experience a decrease in the severity of symptoms associated with their disease. Likewise, participating in a regular aerobic fitness program may help to reduce the risk of developing a chronic disease.
There are many positive physical and physiologic changes that occur when one participates in a cardiovascular fitness program. Individuals who perform a cardiovascular fitness program have a lower risk of developing many chronic diseases including cardiovascular disease, type 2 diabetes, and some cancers.3,5,12,17–19,26,29,32,33 Additional training benefits associated with regular participation in an aerobic exercise program include reduction/control of one’s weight, an increase in muscular strength, a reduction in the risk of falls, and a reduced mortality.9,13
The most notable physical and physiologic changes associated with regular participation in an aerobic exercise training are4,23,25:
 Increased size and number of mitochondria
Increased size and number of mitochondria

 Increased heart weight and size
Increased heart weight and size
 Increased cardiac output and stroke volume
Increased cardiac output and stroke volume
 Improved mobilization and use of fat and carbohydrates
Improved mobilization and use of fat and carbohydrates
 Selective hypertrophy of type I slow twitch oxidative muscle fibers
Selective hypertrophy of type I slow twitch oxidative muscle fibers
 Decreased resting heart rate and submaximal heart rate
Decreased resting heart rate and submaximal heart rate

 Increased blood volume and hemoglobin
Increased blood volume and hemoglobin
 Reduced systolic and diastolic blood pressure
Reduced systolic and diastolic blood pressure
 Significantly improved oxygen extraction rates from the blood
Significantly improved oxygen extraction rates from the blood
MINIMUM AEROBIC EXERCISE GUIDELINES FOR AMERICANS
The Centers for Disease Control and Prevention (CDC) has provided physical activity guidelines for children, adults, healthy pregnant or postpartum women, and older adults.1,9 Table 5-1 presents the minimum aerobic exercise guidelines suggested to improve one’s aerobic fitness.1,9
Table 5-1
Minimum Weekly Aerobic Exercise Guidelines for Adults
| Intensity Level | Adults | Older Adults(65 years of age or older) | Healthy Pregnant or Postpartum Women |
| Moderate intensity aerobic activity | 2 hours and 30 minutes weekly | 2 hours and 30 minutes weekly | 2 hours and 30 minutes weekly |
| Vigorous intensity aerobic activity | 1 hour and 15 minutes weekly | 1 hour and 15 minutes weekly | May continue vigorous intensity activities, such as running, if performing these exercises before her pregnancy. |
| Combination | Equal amount of moderate and vigorous intensity aerobic activity | Equal amount of moderate and vigorous intensity aerobic activity | N/A |

From Centers for Disease Control and Prevention: Physical activity for everyone (website): www.cdc.gov/physicalactivity/everyone/guidelines/index.html. Accessed March 15, 2010.
Exercise Guidelines for Adults
The minimum exercises guidelines for adults, older adults, and healthy pregnant or postpartum women are based on the volume of moderate or vigorous intensity aerobic activity one performs.9 The CDC has provided both relative and absolute guidelines to help one appreciate the intensity of his or her exercise session.9 The talk test may be used to determine the relative intensity of an exercise session.9 If one is able to talk during exercise, that exercise is of moderate-intensity. If one is unable to speak more than a few words before needing to pause for a breath, then they are likely performing a vigorous intensity exercise. The absolute intensity guidelines are based on the amount of energy one typically uses during 1 minute of exercise.9 Examples of moderate intensity exercises include walking briskly, water aerobics, doubles tennis, and cycling at a pace less than 10 miles per hour.9 Running, swimming laps, singles tennis, cycling faster than 10 miles per hour, and hiking are all examples of vigorous intensity exercises.9
The CDC recommends that as adults’ fitness level improves, they should increase their level of either moderate intensity aerobic activity to 5 hours a week, or to 21⁄2 hours of vigorous intensity aerobic activity each week, or to an equal mix of both types.9
Exercise Guidelines for Children
The number of children and adolescents who are considered overweight or obese has at least doubled during the past twenty years.21 Recent studies have demonstrated that the likelihood that one will be obese as an adult increases if he or she was obese as a child.31 To combat pediatric obesity, children and adolescents need to participate in daily physical activity. A lack of physical education in many school districts limits the opportunities during the day for a child to exercise.20
The CDC recommends that children perform at least 60 minutes of moderate intensity exercises each day.9,30 In addition, children should perform vigorous intensity exercises at least 3 times a week.9 The physical therapy team may play a crucial role in educating a family as to the importance of daily physical activity for a child as well as developing and implementing a fitness program for the child.8
ADDITIONAL METHODS TO MEASURE EXERCISE INTENSITY
In a clinical exercise physiology setting the efficiency of one’s aerobic fitness may be determined by measuring the maximum volume of oxygen consumed during exercise. This measure has been termed the maximal oxygen uptake or the Vo2 max.2,11,25 Using this number, a clinician can prescribe a particular exercise intensity based on a percentage of one’s Vo2 max.
The aforementioned talk test (previous section) is one manner to determine a client’s aerobic exercise intensity. Two other methods used to measure aerobic intensity are the target heart rate/estimated maximum heart rate method and the perceived exertion method.9
Target Heart Rate and Estimated Maximum Heart Rate
The CDC recommends that an individual who is performing moderate intensity exercise should do so at a target heart rate range of 50% to 70% of one’s maximum heart rate (beats per minute).9 When an individual performs vigorous intensity exercise, their target heart rate (THR) should be 70% to 85% of their maximal heart rate (MHR).9 How is the MHR measured? To calculate a client’s/patient’s MHR, the individual’s age is subtracted from 220 (e.g., 220 − 30). To establish the THR, the MHR is multiplied by the desired intensities. These two calculations (Table 5-2) will provide the lower and upper limit target heart rates for someone who is performing moderate or vigorous intensity exercises.9
Table 5-2
Target Heart Rate Calculations for a 30-Year-Old Individual
| Moderate Intensity Exercise | Vigorous Intensity Exercise | |
| Formula | MHR × (0.50) or (0.70) | MHR × (0.70) or (0.85) |
| Lower limit | (220 − 30) × 0.50 = 95 beats per minute | (220 − 30) × 0.70 = 113 beats per minute |
| Upper limit | (220 − 30) × 0.70 = 113 beats per minute | (220 − 30) × 0.85 = 162 beats per minute |
The Karvonen method has been suggested as an alternative method of calculating THR.25 The Karvonen method differs from the aforementioned technique in that it accounts for one’s resting heart rate. In the previous example (see Table 5-2), the THR for a 30-year-old individual performing moderate intensity exercise is 95 to 113 beats per minute. If this individual has a resting heart rate of 70 beats per minute, the THR range would be 130 to 154 beats per minute (Table 5-3).
Table 5-3
Target Heart Rate Calculations Using the Karvonen Method
| Moderate Intensity Exercise | |
| Formula | MHR (or HRmax) = 220 − 30 = 190 |
| 50% MHR | [(190 − 70) × 0.50] + 70 = 130 |
| 70% MHR | [(190 − 70) × 0.70] + 70 = 154 |
Target heart rate (THR) = [(HRmax – HRrest) × % Intensity] + HRrest; MHR, maximum heart rate.
Borg Rating of Perceived Exertion
The Borg Rating of Perceived Exertion scale may be used to assess exercise intensity based on an individual’s perception of exertion. While the client is exercising, ask him or her to rate how hard he or she is exercising based on the Borg scale. The Borg scale ranges from 6 to 20 points, with a 6 corresponding to “no exertion at all” and a 20 corresponding to “maximal exertion.”6 The client/patient should be asked to view the scale each time when measuring perceived exertion. The Borg scale has also been found to correlate with one’s heart rate.6,7 This is a helpful feature allowing the clinician to monitor exercise intensity level based on an estimate of heart rate. To determine heart rate from the Borg scale, multiply the perceived rating (e.g., 13) by a factor of 10 (e.g., 130 beats per minute).
AEROBIC EXERCISE FOR PATIENTS WITH AN ORTHOPEDIC INJURY
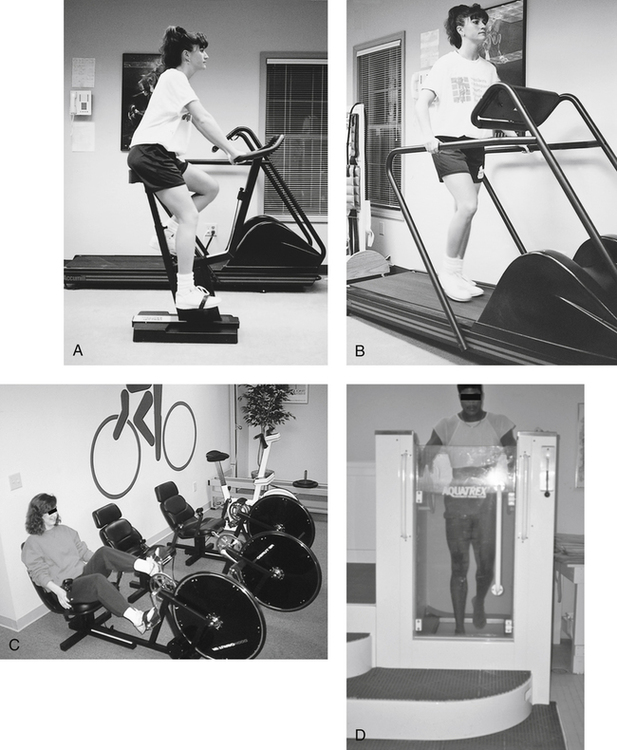
Evidence suggests that aerobic fitness activities should be included in a rehabilitation program for a patient recovering from a back injury.27 Riding a stationary bicycle or walking on a treadmill (Fig. 5-1, A–B) may help to facilitate initial aerobic training. However, sitting on the saddle seat of a stationary ergometer may be uncomfortable or provoke symptoms for many patients with back problems. A recumbent cycle, with its large bucket seat (Fig. 5-1, C) to provide lumbar support, may be preferred by many clients. Patients who are unable to tolerate land based aerobic exercises may benefit from walking on an underwater treadmill. Immersion in the water can provide enough buoyancy during walking, unloading the spine, allowing the patient to exercise without exacerbating symptoms (Fig. 5-1, D).
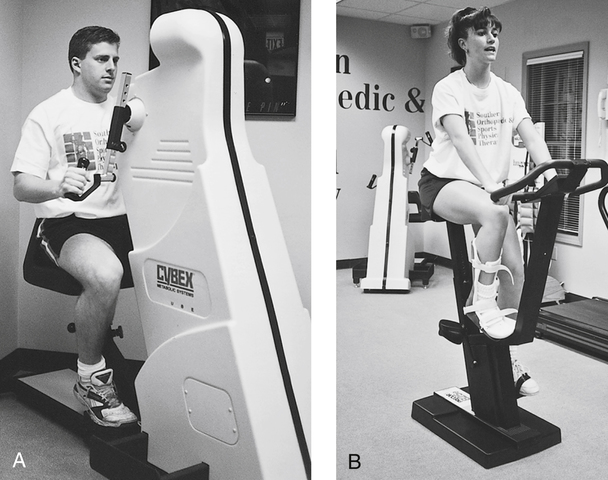
Patients who have sustained a lower extremity injury or are recovering after a lower extremity surgery can maintain or improve cardiorespiratory fitness using an upper body ergometer (UBE) (Fig. 5-2, A). The UBE is ideal for individuals who are contraindicated from either bearing weight or performing range of motion activities with their involved lower extremity. The single-leg stationary bicycle ergometer exercise (Fig. 5-2, B) may also be safely initiated by a patient before beginning double-leg cycling.
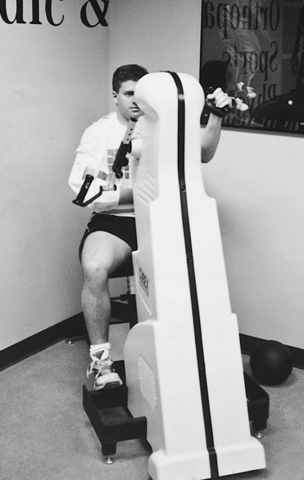
Patients with upper extremity conditions can use a stationary cycle or treadmill for endurance training. Patients also can be instructed to use one-arm cycling on a UBE (Fig. 5-3) to maintain upper body aerobic fitness.
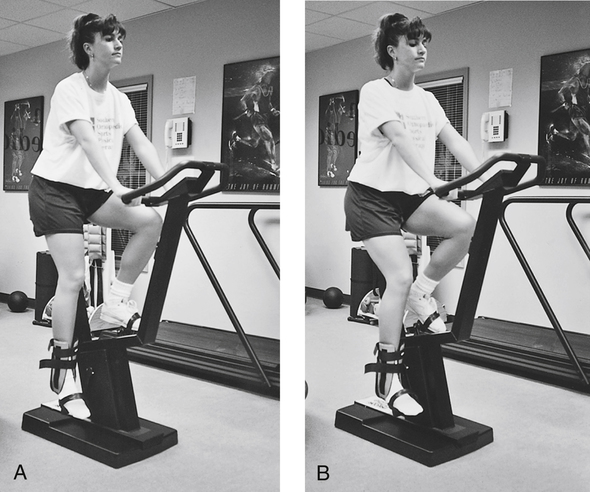
Modifications can be made on stationary cycles to allow for continued aerobic conditioning after an ankle injury or surgery. Typically the seat height should allow for slight knee flexion (~10°) at the end of the pedal stroke. With the seat in normal position, the foot generally plantar flexes toward the end of the pedal stroke, causing stress to the anterior talofibular ligament. Therefore the seat height is lowered for a patient with a severe ankle sprain to allow for a complete pedal stroke and keep the ankle joint in neutral (Fig. 5-4).
MUSCULAR ENDURANCE TRAINING
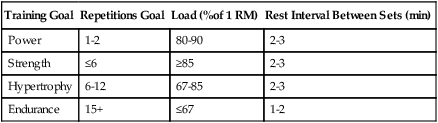
To increase muscular endurance, sets of high repetitions should be performed. At least 15 repetitions should be performed per set.2,10 Each repetition should be performed at or below 67% of one’s 1 RM (repetition maximum). A period of 1 to 2 minutes should be allowed for rest in between each set. Table 5-4 compares variables associated with the four main types of muscular training: power, strength, hypertrophy, and endurance.
Table 5-4
Training Variables Associated with Training Goals
| Training Goal | Repetitions Goal | Load (%of 1 RM) | Rest Interval Between Sets (min) |
| Power | 1-2 | 80-90 | 2-3 |
| Strength | ≤6 | ≥85 | 2-3 |
| Hypertrophy | 6-12 | 67-85 | 2-3 |
| Endurance | 15+ | ≤67 | 1-2 |
Muscular endurance training plays a key role when rehabilitating patients with an orthopedic injury.14,22,24,27,28 Using the muscular endurance training principles allows the physical therapy team to prescribe strengthening exercises during the subacute phase of healing (see Chapter 11) while reducing the risk of overstressing the healing tissue.




