Endometriosis
Synonyms/Description
Endometriosis signifies the presence of endometrial tissue outside the endometrial cavity. These ectopic glands respond to the cyclical hormones, thus causing microscopic internal bleeding and pain during the course of the menstrual cycle. This ectopic tissue bleeds episodically, causing inflammation, adhesions, and scarring. These ectopic glands can also react to hormones of pregnancy.
Etiology
The exact cause of endometriosis is unknown and there are multiple theories. In addition, the true prevalence of this condition is also unclear because endometriosis is not always symptomatic. There does, however, appear to be a higher incidence in women who are diagnosed with infertility and pelvic pain.
Endometriosis can occur in many forms, including the formation of cysts known as endometriomas (chocolate cysts), which typically develop in ovarian tissue. Endometriosis can also occur in the uterus with the propagation of endometrial glands through the junctional zone into the myometrium, a condition known as adenomyosis (see Adenomyosis). Endometriosis can also take the form of small deep implants of endometrial tissue in many different places in the body, including the wall of the bladder, the anterior abdominal wall, the bowel wall, and the uterosacral ligaments, as well as other pelvic sites. Rarely, endometriosis can occur in distal sites such as the lung, potentially causing hemoptysis.
Ultrasound Findings
Endometrioma
The typical appearance of an endometrioma is that of a unilocular cyst with homogeneous low-level echoes and through transmission of sound. The ground-glass texture of the cyst content is very characteristic and makes 90% of endometriomas easily recognizable. Some benign endometriomas also have solid components (often echogenic) in the inner aspect of the cysts, but these are typically without discernible blood flow and represent clot. When interrogating endometriomas with color Doppler, there is no discernible flow in the cyst (only in the wall) and there is usually no visible streaming of the low-level echoes within the cyst, thus distinguishing it from cystadenomas and other cysts. Patients with endometriomas often have adhesions so that tubal disease in the form of a hydrosalpinx or other signs of adhesive disease may be a common finding.
When the cyst wall is thickened and irregular, the possibility of malignancy, specifically endometrioid carcinoma, must be considered. Typically endometrioid carcinoma looks like an endometrioma but with internal solid nodularity that contains abundant color Doppler flow. In a study of 309 endometrioid cysts surgically removed, 1.2% were classified as borderline, and 3.4% as invasive endometrioid tumors. Patients with malignancies were typically older (median 52 years) compared with those with benign cysts (median 34 years). All of the malignant and borderline tumors were characterized as having solid components with evidence of color flow, compared with only 7.8% of the benign lesions.
Decidualized Endometrioma
If the patient is pregnant, the endometrioma may become decidualized and have ultrasound characteristics suggestive of a malignancy. The stromal transformation of endometrial cells within the endometrioma can occur because of high levels of progesterone in pregnancy. In gravid patients, these cysts can contain internal solid nodularity with blood flow, and are indistinguishable from borderline or even frank ovarian cancers sonographically.
Therefore such cysts may potentially be watched with frequent serial ultrasounds before making a final decision to remove the cyst during the pregnancy. If the cyst remains unchanged, it is unlikely to be malignant, and removal can be planned after delivery.
Deep Penetrating Bowel Wall and Pelvic Implants
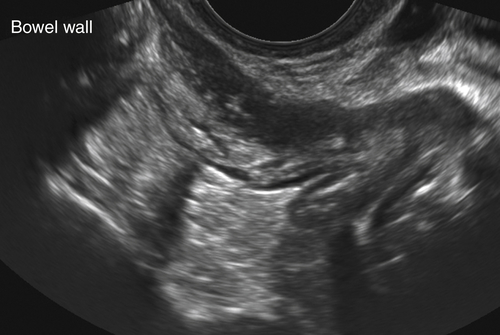
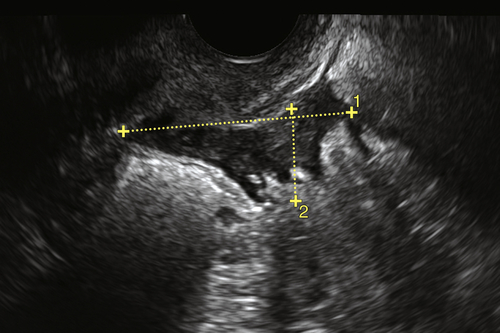
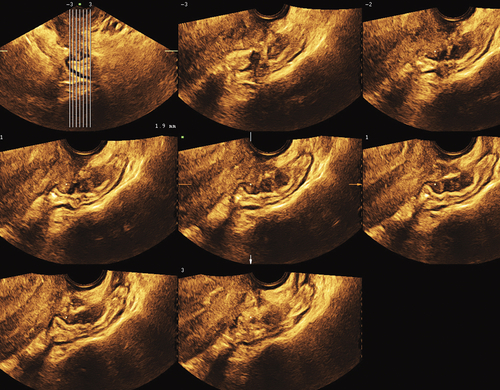
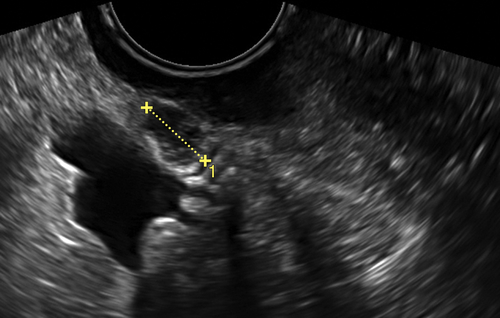
Sonographically, deep implants of endometriosis are small solid masses with little if any detectable blood flow using color Doppler. The bowel wall implants are nodular and fusiform swellings of one side of the bowel wall. This swelling is often adherent to the back of the cervix, thus hindering any sliding of the uterus past the bowel on exam. Bazot reports a sensitivity and specificity of 78.5% and 95.2%, respectively, for detecting disease in that location, suggesting that ultrasound (in experienced hands) is accurate in diagnosing rectosigmoid endometriosis. Hudelist and colleagues report a sensitivity and specificity of 91% and 98%, respectively, and positive likelihood ratio and negative likelihood ratios of 30.4 and 0.1, respectively, for detecting bowel wall endometriosis using ultrasound. Although MRI can also detect implants of endometriosis, evidence shows that pain-guided transvaginal ultrasound is likely more sensitive for detecting bowel involvement.
Implants in the rectovaginal septum are also nodular, small, rounded, solid structures best seen along the most distal portion of the cervix and along the posterior fornix and upper vagina. Implants may also be found on the pelvic ligaments such as the uterosacral ligaments and para pelvic regions.
Bladder Wall, Ureter, and Anterior Abdominal Wall Lesions (Also See Bladder Masses)
Implants of endometriosis can occur practically anywhere; however, the more common areas of involvement include the bladder wall, ureter, and anterior abdominal wall in patients who have had abdominal surgery such as a prior C-section or laparoscopy. Endometriosis of the bladder wall appears as a fusiform solid thickening of the wall itself. If endometrial implants impinge on the ureter, the patient may have chronic ureteral obstruction that is silent and may lead to a nonfunctioning kidney.
In patients who have had prior abdominal surgery, endometriosis may present as a hard, solid mass in the anterior abdominal wall in the region of the scar. Little color flow may be present, and the mass is often tender.
Differential Diagnosis
Endometrioma
Most endometriomas involve the ovary and have a characteristic appearance, which is a unilocular cyst with homogeneous low-level echoes and no color flow. Some endometriomas can be multilocular or septate or have a thickened wall with echogenic material. These cysts may be confused with dermoids (echogenic area), cystadenomas (septations), or even malignancy if there is some solid component. Color Doppler is essential to interrogate these solid areas for blood flow. The absence of flow may suggest a cystadenoma-fibroma or endometrioma. If color flow is present, one must consider decidualized endometrioma (in pregnancy) versus a borderline or invasive endometrioid carcinoma.
Streaming is typically absent in endometriomas when using Doppler. If the cyst has streaming echoes, a diagnosis other than endometriosis should be considered.
Deep Penetrating Bowel Wall and Pelvic Implants
Patients with deep bowel wall and pelvic endometrial implants are typically in a lot of pain during the transvaginal examination, and the pelvic organs tend to be adherent to each other. It is important to try to move the uterus with the vaginal probe to see if it slides past the anterior wall of the rectosigmoid and the ovaries. If these organs are stuck together in a patient with pain, then endometriosis is likely. Other lesions involving the bowel wall include inflammatory bowel disease or lymphoma; however, both of these diseases have diffuse (nonfocal) bowel involvement without extensive adhesions or focal pain (see Bowel Diseases). Solid implants with color flow in the peritoneal cavity may indicate carcinomatosis, although this is usually accompanied by ascites.
Bladder Wall Lesions
Endometriosis of the bladder wall is usually well contained within the wall and has little detectable blood flow. The mucosal surface remains smooth, unlike a transitional cell carcinoma, which is a fungating vascular lesion of the mucosal surface.
Clinical Aspects and Recommendations
The three general categories that comprise the clinical manifestations of endometriosis include (1) pelvic pain, (2) infertility, and (3) pelvic mass. The goal of any therapy is to relieve the symptoms. There are so many different medical treatments that decisions regarding management must be individualized, taking into account severity of symptoms, extent and location of the disease, desire for future fertility, medication side effects, surgical complication rates, and even cost.
Detailed treatment options are beyond the scope of this section, but would include expectant management, analgesia, various hormonal medical therapies, surgical intervention, which may be conservative and tissue sparing or definitive (total abdominal hysterectomy and possible bilateral salpingo-oophorectomy), or combinations of these therapies. As always, minimally invasive surgery in the form of laparoscopy would be preferable to open laparotomy although often the extent of adhesions may make a minimally invasive approach difficult, if not impossible.
Figures
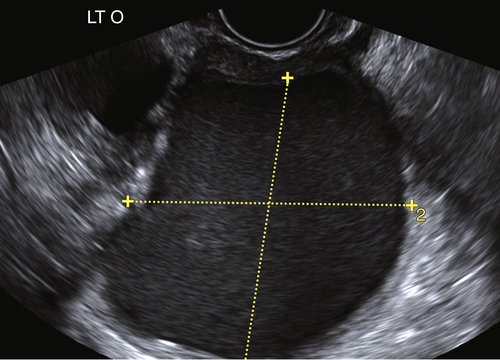
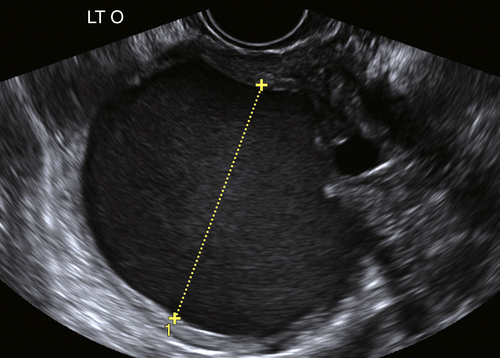
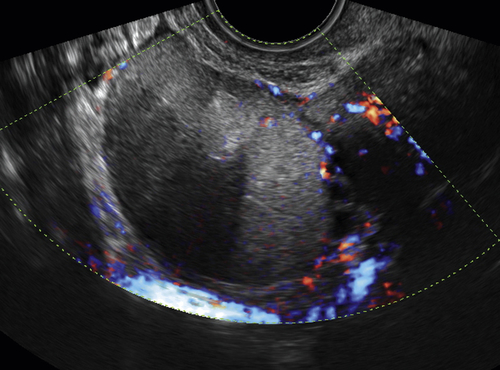
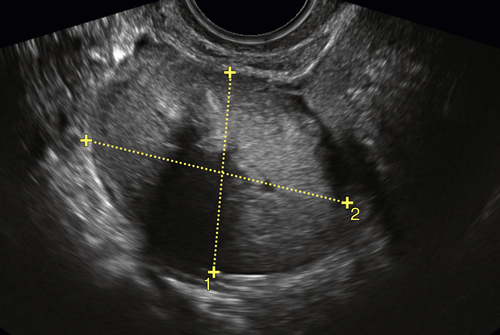
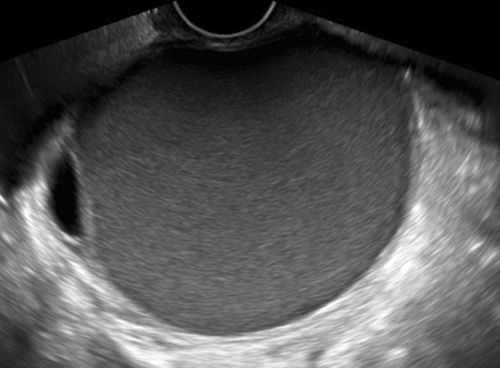
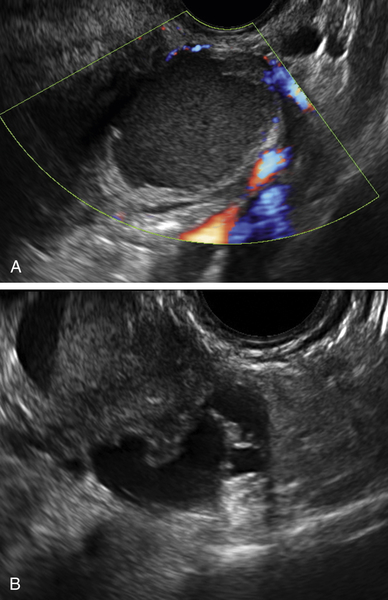
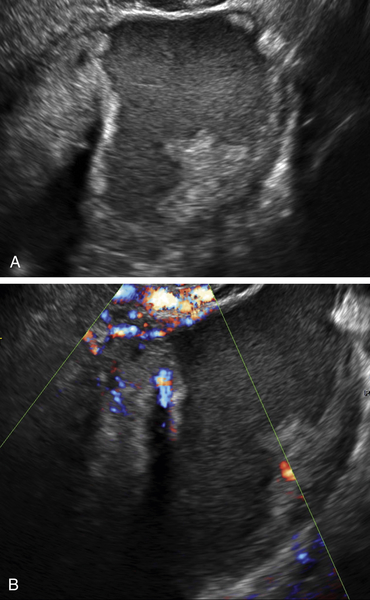
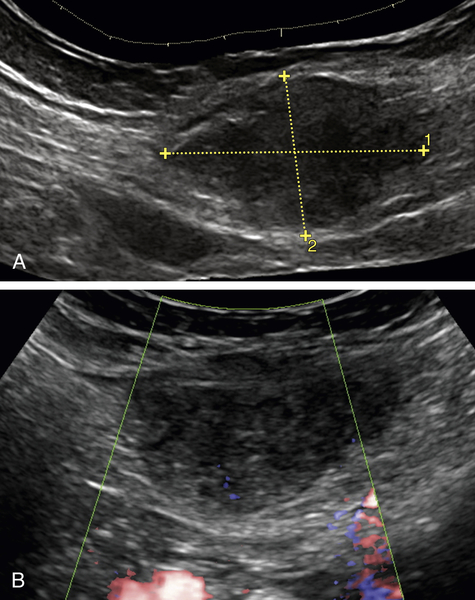
Figure E4-5 A, Cystic mass in a pregnant patient showing an irregular and nodular inner wall with cystic contents displaying low-level echoes. B, Image showing blood flow in the solid areas, a finding that is worrisome for a malignancy. This mass was proved to be a decidualized endometrioma at surgery.
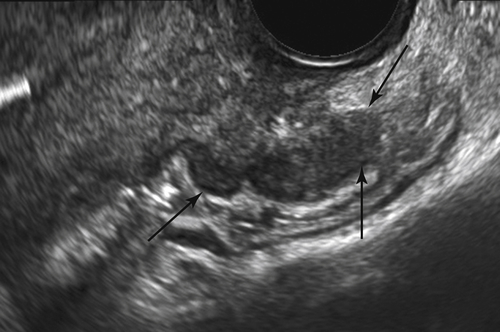
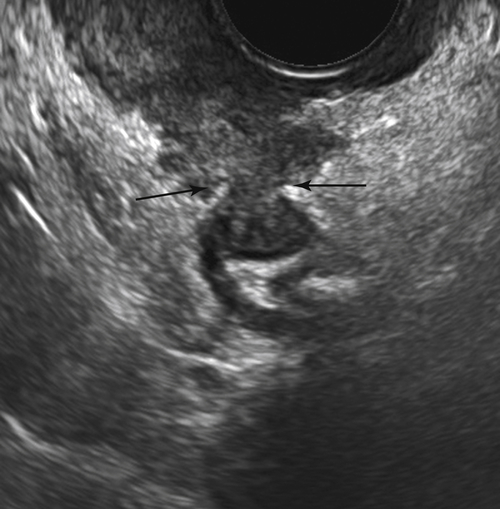
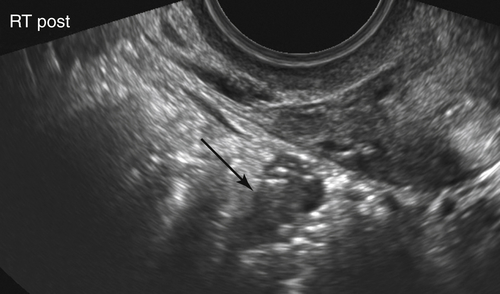
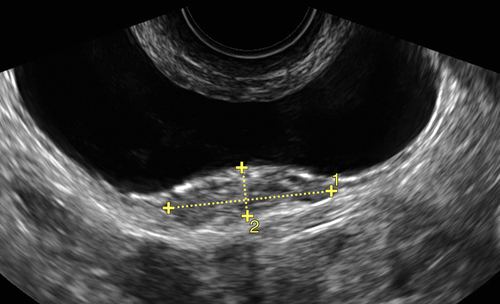
Figure E4-6 Transverse and longitudinal views of the anterior wall of the rectosigmoid, showing solid nodular masses compressing the lumen (arrows). These are typical of endometriotic implants in the bowel wall. Note that the involved bowel is adjacent to the back of the cervix and posterior fornix of the vagina.