Chapter 10 Endocardial Fibroelastosis
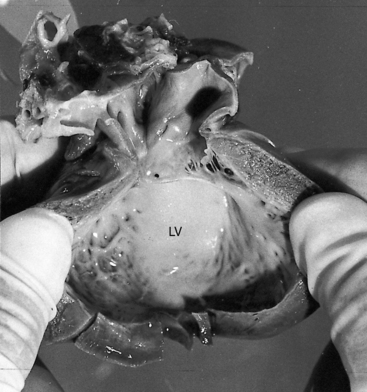
Endocardial fibroelastosis, a self-defining term introduced in 1943,1 is characterized by an opaque, pearly-white thickening that results from proliferation of collagen and elastic fibers (Figure 10-1).2,3 Isolated endocardial fibroelastosis involves the endocardium of a dilated hypertrophied left ventricle,2,3 hence the term primary endocardial fibroelastosis of the dilated type. Conversely, albeit rarely, the left ventricular cavity is small, hence the term endocardial fibroelastosis of the contracted type.2,3 Another form of endocardial fibroelastosis is considered secondary because it accompanies certain congenital malformations of the heart,3 especially aortic stenosis,4 coarctation of the aorta,5 anomalous origin of the left coronary artery from the pulmonary trunk,6 and hypoplastic left heart.7 Endocardial fibrosis is a substrate for mural thrombosis, which sets the stage for systemic emboli.8,9 The endocardium occasionally calcifies.
Pathogenesis takes into account the gross and histologic endocardial abnormalities and ventricular hypertrophy that characterize primary endocardial fibroelastosis of the dilated type. Fibroelastosis per se is a response to a variety of endocardial stimuli, with intrauterine endocardial injury as the common denominator.10–14 The disorder has been reported with or without complete heart block in fetuses and children of mothers who are positive for anti-Ro or anti-La antibodies.15,16 Fibroelastosis occurs in infants and adults after myocardial infarction,9,17 underscoring the endocardial response to injury.
Primary dilated endocardial fibroelastosis is the type that occurs in infants.18,19 Beyond infancy, the endocardial lesion tends to be patchy and is associated with myocardial fibrosis. The relationship between the infantile, the adolescent, and the adult form of the disease is unclear,18–21 and the relationship between the dilated and nondilated types has not been established.3,10,22
Primary endocardial fibroelastosis of the dilated type principally involves the left ventricle.3,23,24 The left atrium, right atrium, and right ventricle are only occasionally affected.25,26 Mitral regurgitation coexists with the dilated type3,27 because the papillary muscles originate high on the left ventricular wall (i.e., from the upper third) and accordingly exert undesirable lateral axes of tension on the chordae tendineae and mitral cusps, resulting in faulty leaflet apposition.3 In addition to being laterally aligned, the chordae tendineae are short and thick,26,27 and the papillary muscles tend to be small with histologic changes that resemble infarction.27
The physiologic consequences of primary endocardial fibroelastosis of the dilated type reflect the basic disorder of left ventricular endocardium, in concert with mitral regurgitation (Figures 10-2 and 10-3). Endocardial thickening restricts contraction of the dilated left ventricle and is responsible for global hypokinesis (see Figures 10-1 and 10-2).23 Elevated pressure in the left atrium, pulmonary veins, and pulmonary artery result in high left ventricular filling pressure and mitral regurgitation.23 Pulmonary hypertension is more pronounced in the nondilated form of the disease because the filling pressure in the small left ventricle is especially high.22,28
History
Primary endocardial fibroelastosis of the dilated type is equally distributed between the genders.29 It has been reported in siblings, in identical twins,30–32 and in more than one generation.20,33,34 The disease manifests itself in the first 6 to 12 months of life.3,29 Most affected children do not live beyond their second birthday.2 Prognosis is especially poor in neonates.14 Symptoms can run a protracted course and can begin suddenly, and death can be sudden and unexpected.2,35,36 Systemic emboli from left ventricular mural thrombi result in serious neurologic sequelae.2,8
Arterial pulse
The slow rate of rise is because of impaired left ventricular contractility. Sinus tachycardia and pulsus alternans are reflections of heart failure.2
Auscultation
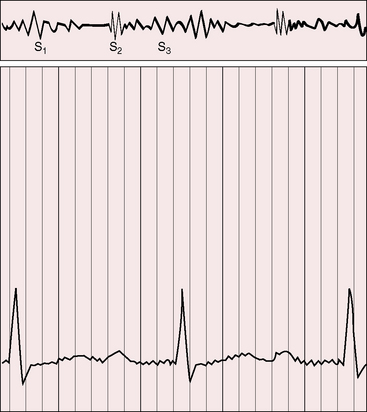
Hypokinetic left ventricular contraction diminishes the murmur of mitral incompetence despite appreciable regurgitant flow (Figure 10-4).2,29 Elevated pulmonary artery pressure augments the pulmonary component of the second heart sound and narrows the splitting. A third heart sound reflects the decrease in left ventricular distensibility2,23,29 and is especially prominent when mitral regurgitation coexists. Third and fourth heart sounds can summate to produce a triple rhythm or a short mid-diastolic murmur (see Figure 10-4).
Electrocardiogram
The electrocardiogram records a variety of disturbances in rhythm and conduction, including paroxysmal atrial, junctional or ventricular tachycardia, and neonatal atrial fibrillation.3,32,37 Complete heart block has been detected in utero2,32,38 and raises the question of a relationship between maternal antibodies, congenital complete heart block, and endocardial fibroelastosis (see previous discussion15,16 and Chapter 4).13 P waves show left atrial, biatrial, or right atrial abnormalities (Figure 10-5), especially in the presence of mitral regurgitation and elevated pulmonary arterial pressure.3,29,37 The PR interval is normal or slightly increased,3,29,37 except in sporadic cases with Wolff-Parkinson-White accessory pathways.37
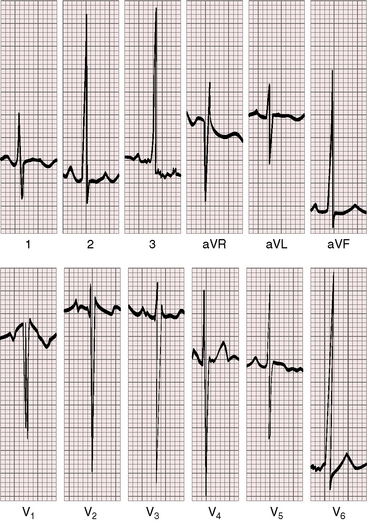
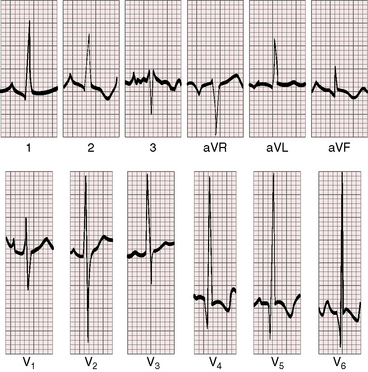
The QRS axis is normal, although rightward or leftward axes occasionally occur.29,37 Left ventricular hypertrophy is an important electrocardiographic feature of primary endocardial fibroelastosis of the dilated type (Figures 10-5 and 10-6).39 Right ventricular or biventricular hypertrophy is reserved for infants with left ventricular failure and reactive pulmonary hypertension.3,23,37 Isolated right ventricular hypertrophy occurs in the nondilated form of the disorder.23,29,40 Q waves are common in left precordial leads in the dilated form because of the volume overload of mitral regurgitation (see Figure 10-6).29 An infarct pattern is a feature of endocardial fibroelastosis associated with anomalous origin of the left coronary artery from the pulmonary trunk (see Chapter 21).41 If an infarct pattern occurs in primary endocardial fibroelastosis, the Q waves are in right precordial leads,41 not in leads 1 and aVL (see Chapter 21).
X-ray
In the dilated form, cardiomegaly is the result of enlargement of the left ventricle and left atrium, which can be massive (Figures 10-7 and 10-8).3,29,39 Calcification of the thickened endocardium is occasionally identified at necropsy but rarely in the x-ray.29 The ascending aorta and pulmonary trunk are inconspicuous compared with the striking increase in heart size (see Figures 10-7 and 10-8).
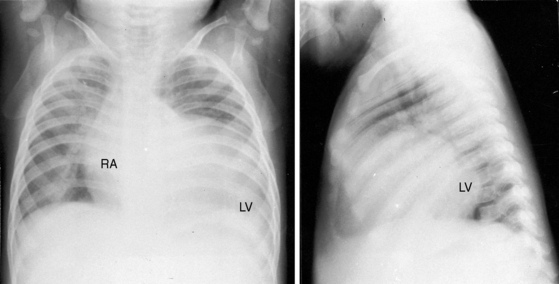
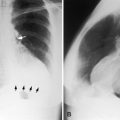
Figure 10-7 X-rays from the 2-month-old male whose electrocardiogram is shown in Figure 10-5. The left ventricle (LV) is strikingly dilated in both projections, and the right atrium (RA) is considerably enlarged. The great arteries are inconspicuous. The lung fields exhibit pulmonary venous congestion.
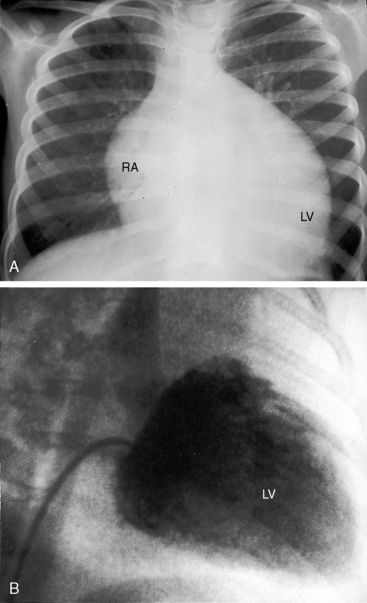
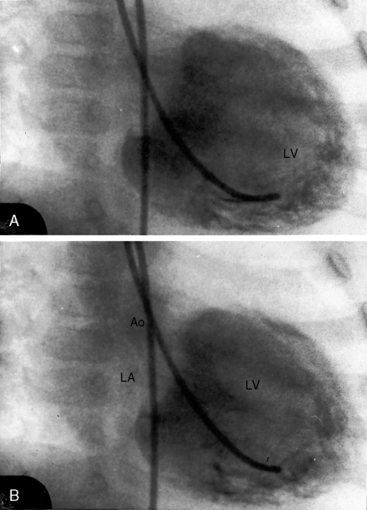
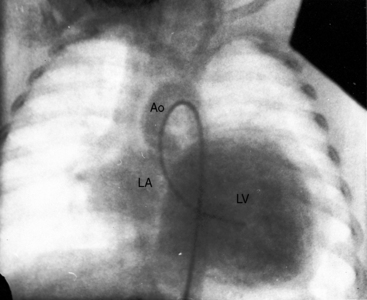
Figure 10-8 A, X-ray from the 6-month-old female whose phonocardiogram is shown in Figure 10-4. The left ventricle (LV) and the right atrium (RA) are strikingly enlarged in contrast with the inconspicuous great arteries. There is pulmonary venous congestion. B, Angiogram showing the dilated hypokinetic left ventricle (LV).
Echocardiogram
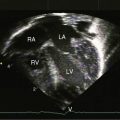
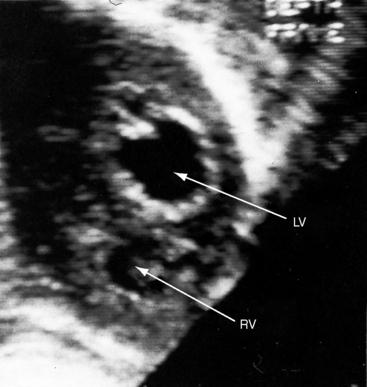
The dilated type of primary endocardial fibroelastosis appears as spherical left ventricular enlargement with striking global hypokinesis.11 Septal and free wall thicknesses are increased because of left ventricular hypertrophy (Figure 10-9). The left atrium is dilated, sometimes massively so. Color flow imaging is used to determine the degree of mitral regurgitation. The echocardiogram permits intrauterine detection.10 The diagnosis of primary endocardial fibroelastosis can be difficult to establish with echocardiography, even though bright echoes appear in the thickened endocardium (see Figures 10-1 and 10-9). Magnetic resonance imaging with perfusion and myocardial delayed enhancement42 and multidetector computed tomography43 can be useful.
1 Weinberg T., Himelfarb A.J. Endocardial fibroelastosis (so-called fetal endocarditis). Bulletin of the Johns Hopkins Hospital. 1943;72:299.
2 Andersen D.H., Kelly J. Congenital endocardial fibro-elastosis. II. A clinical and pathologic investigation of those cases without associated cardiac malformations including report of two familial instances. Pediatrics. 1956;18:539-555.
3 Moller J.H., Lucas R.V.Jr, Adams P.Jr, Anderson R.C., Jorgens J., Edwards J.E. Endocardial fibroelastosis. A clinical and anatomic study of 47 patients with emphasis on its relationship to mitral insufficiency. Circulation. 1964;30:759-782.
4 Dushane J.W., Edwards J.E. Cardiac clinics. CXLII. Congenital aortic stenosis in association with endocardial sclerosis of the left ventricle. Proceedings of the Staff Meetings Mayo Clinic. 1954;29:102-108.
5 Oppenheimer E.H. The association of adult-type coarctation of the aorta with endocardial fibroelastosis in infancy. Bulletin of the Johns Hopkins Hospital. 1953;93:309-319.
6 Noren G.R., Raghib G., Moller J.H., Amplatz K., Adams P.Jr, Edwards J.E. Anomalous origin of the left coronary artery from the pulmonary trunk with special reference to the occurrence of mitral insufficiency. Circulation. 1964;30:171-178.
7 Noonan J.A., Nadas A.S. The hypoplastic left heart syndrome; an analysis of 101 cases. Pediatr Clin North Am. 1958;5:1029-1056.
8 Branch G.L., Castle R.F. Thromboembolic complications in primary endocardial fibroelastosis. J Pediatr. 1966;69:250-258.
9 Lee K.T., Mcgavran M.H., Rabin E.R., Thomas W.A. Endocardial fibroelastosis in infants associated with thrombosis and calcification of arteries and myocardial infarcts. N Engl J Med. 1956;255:464-468.
10 Carceller A.M., Maroto E., Fouron J.C. Dilated and contracted forms of primary endocardial fibroelastosis: a single fetal disease with two stages of development. Br Heart J. 1990;63:311-313.
11 Schryer M.J., Karnauchow P.N. Endocardial fibroelastosis; etiologic and pathogenetic considerations in children. Am Heart J. 1974;88:557-565.
12 Shone J.D., Munoz Armas S., Manning J.A., Keith J.D. The mumps antigen skin test in endocardial fibroelastosis. Pediatrics. 1966;37:423-429.
13 Singsen B.H., Akhter J.E., Weinstein M.M., Sharp G.C. Congenital complete heart block and SSA antibodies: obstetric implications. Am J Obstet Gynecol. 1985;152:655-658.
14 Westwood M., Harris R., Burn J.L., Barson A.J. Heredity in primary endocardial fibroelastosis. Br Heart J. 1975;37:1077-1084.
15 Nield L.E., Silverman E.D., Smallhorn J.F., et al. Endocardial fibroelastosis associated with maternal anti-Ro and anti-La antibodies in the absence of atrioventricular block. J Am Coll Cardiol. 2002;40:796-802.
16 Nield L.E., Silverman E.D., Taylor G.P., et al. Maternal anti-Ro and anti-La antibody-associated endocardial fibroelastosis. Circulation. 2002;105:843-848.
17 Hutchins G.M., Bannayan G.A. Development of endocardial fibroelastosis following myocardial infarction. Arch Pathol. 1971;91:113-118.
18 Rafinski T., Golenia A., Wozniewicz B., Wlad S. Familial endocardial fibroelastosis. J Pediatr. 1967;70:574-576.
19 Thomas W.A., Randall R.V., Bland E.F., Castleman B. Endocardial fibroelastosis; a factor in heart disease of obscure etiology: a study of 20 autopsied cases in children and adults. N Engl J Med. 1954;251:327-338.
20 Hanukoglu A., Fried D., Somekh E. Inheritance of familial primary endocardial fibroelastosis. Clin Pediatr (Phila). 1986;25:272-275.
21 Hoffman F.G. Adult endocardial fibroelastosis associated with dextrocardia and situs inversus. Circulation. 1960;22:437-447.
22 Ursell P.C., Neill C.A., Anderson R.H., Ho S.Y., Becker A.E., Gerlis L.M. Endocardial fibroelastosis and hypoplasia of the left ventricle in neonates without significant aortic stenosis. Br Heart J. 1984;51:492-497.
23 Lynfield J., Gasul B.M., Luan L.L., Dillon R.F. Right and left heart catheterization and angiocardiographic findings in idiopathic cardiac hypertrophy with endocardial fibroelastosis. Circulation. 1960;21:386-400.
24 Manning J.A., Keith J.D. Fibroelastosis in children. Prog Cardiovasc Dis. 1964;7:172-178.
25 Bjorkhem G., Lundstrom N.R., Wallentin I., Carlgren L.E. Endocardial fibroelastosis with predominant involvement of left atrium. Possibility of diagnosis by non-invasive methods. Br Heart J. 1981;46:331-337.
26 Burke E.C. Pediatric clinicopathologic conference. Mayo Clin Proc. 1970;45:467.
27 Davachi F., Moller J.H., Edwards J.E. Diseases of the mitral valve in infancy. An anatomic analysis of 55 cases. Circulation. 1971;43:565-579.
28 Fixler D.E., Cole R.B., Paul M.H., Lev M., Girod D.A. Familial occurrence of the contracted form of endocardial fibroelastosis. Am J Cardiol. 1970;26:208-213.
29 Sellers F.J., Keith J.D., Manning J.A. The diagnosis of primary endocardial fibroelastosis. Circulation. 1964;29:49-59.
30 Greaves J.L., Wilkins P.S., Pearson S. Endocardial fibro-elastosis in identical twins. Arch Dis Child. 1954;29:447-450.
31 Lee M.H., Liebman J., Steinberg A.G., Perrin E.V., Whitman V. Familial occurrence of endocardial fibroelastosis in three siblings, including identical twins. Pediatrics. 1973;52:402-411.
32 Rios B., Duff J., Simpson J.W. Endocardial fibroelastosis with congenital complete heart block in identical twins. Am Heart J. 1984;107:1290-1293.
33 Nielsen J.S. Primary endocardial fibroelastosis in three siblings. Acta Med Scand. 1965;177:145-151.
34 Vestermark S. Primary endocardial fibroelastosis in siblings. Acta Paediatr. 1962;51:94-96.
35 Alter B.P., Czapek E.E., Rowe R.D. Sweating in congenital heart disease. Pediatrics. 1968;41:123-129.
36 Vestermark S. Primary endocardial fibroelastosis. Cardiologia. 1966;48:520-531.
37 Vlad P., Rowe R.D., Keith J.D. The electrocardiogram in primary endocardial fibroelastosis. Br Heart J. 1955;17:189-197.
38 Hung W., Walsh B.J. Congenital auricular fibrillation in a newborn infant with endocardial fibroelastosis. Report of a case with necropsy. J Pediatr. 1962;61:65-69.
39 Freundlich E., Munk J., Griffel B., Steinlauf J. Primary myocardial disease in infancy. Am J Cardiol. 1964;13:721-733.
40 Tingelstad J.B., Shiel F.O., Mccue C.M. The elctrocardiogram in the contracted type of primary endocardial fibroelastosis. Am J Cardiol. 1971;27:304-308.
41 Lintermans J.P., Kaplan E.L., Morgan B.C., Baum D., Guntheroth W.G. Infarction patterns in endocardial fibroelastosis. Circulation. 1966;33:202.
42 Stranzinger E., Ensing G.J., Hernandez R.J. MR findings of endocardial fibroelastosis in children. Pediatr Radiol. 2008;38:292-296.
43 Suh S.Y., Kim E.J., Yong H.S., et al. Endocardial fibroelastosis demonstrated on multidetector computed tomography. Int J Cardiol. 2008;124:e51-e52.