Chapter 1 Embryology of the Reproductive Tract

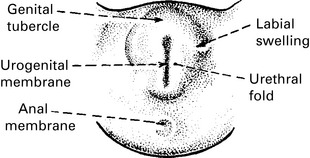
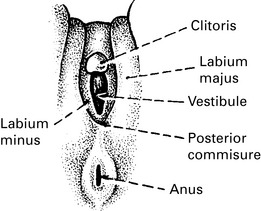
Development of external genitalia
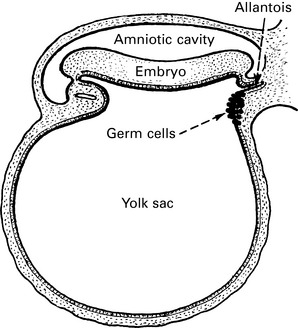
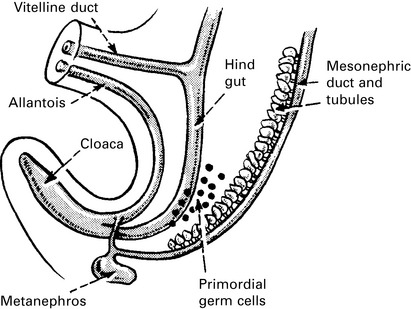
At an early stage, the hind gut and the various urogenital ducts open into a common cloaca.
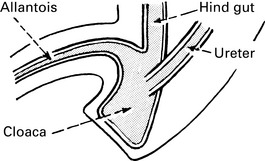
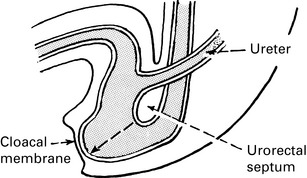
A septum (urorectal) grows down between the allantois and the hind gut during the 5th week.
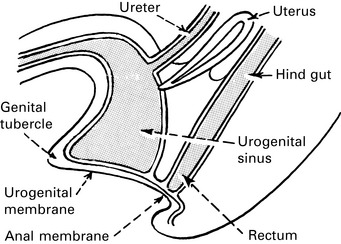
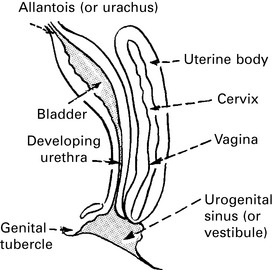
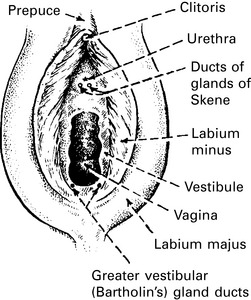
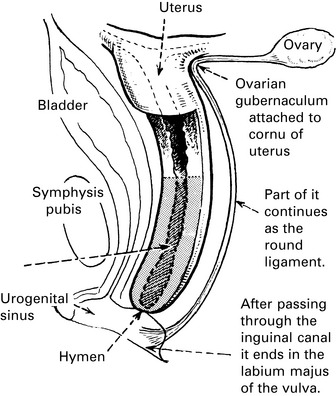
Certain small, but clinically important, glands are formed in and around the urogenital sinus.