[level-membership-for-basic-science-category]
CHAPTER 48 Elbow
SKIN AND SOFT TISSUE
SKIN
Cutaneous vascular supply
The skin overlying the cubital fossa receives its blood supply on its anterolateral side by small perforating vessels from the radial collateral artery, together with some small musculocutaneous perforators from the radial recurrent artery which traverse brachioradialis (Fig. 45.4). On the anteromedial side, skin is supplied by small branches from the anastomosis between the inferior ulnar collateral artery and the anterior ulnar recurrent artery and by small branches from the brachial artery.
Cutaneous innervation
The skin of the cubital fossa and the epicondylar regions is innervated by the medial and lateral cutaneous nerves of the forearm (Fig. 45.15). A small proximal area on the lateral aspect is supplied by the distal part of the lower lateral cutaneous nerve of the arm. The skin over the olecranon region is innervated by the distal branches of the posterior cutaneous nerve of the arm, together with proximal branches of the posterior cutaneous nerve of the forearm.
SOFT TISSUE: CUBITAL FOSSA
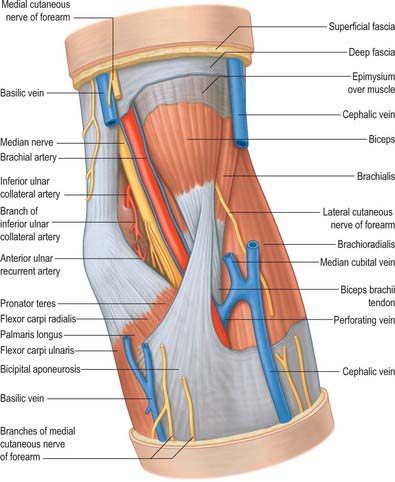
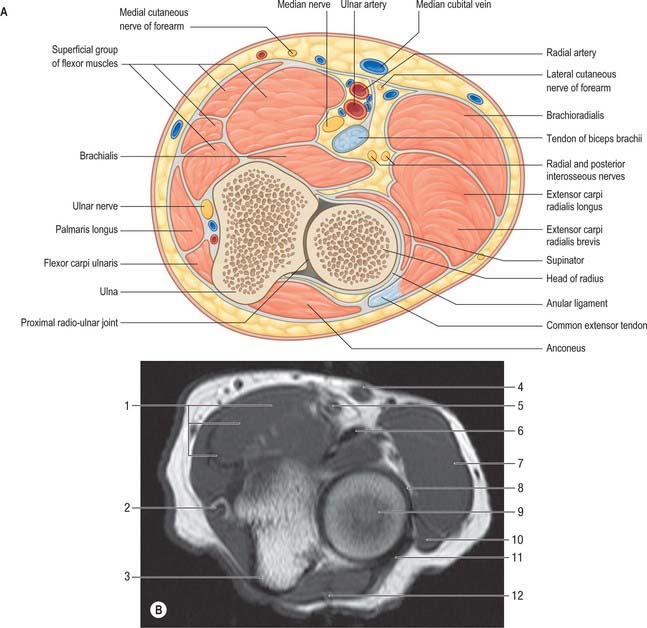
The cubital fossa forms a triangular depression in the middle of the upper part of the anterior aspect of the forearm (Fig. 48.1). The superior border of the fossa is an imaginary line, which joins the two epicondyles of the humerus. The fleshy elevation which constitutes its medial border is formed by the lateral margin of pronator teres and the elevation which forms the lateral border is the medial edge of brachioradialis. The roof of the fossa is formed by the deep fascia of the forearm, reinforced by the bicipital aponeurosis on the medial aspect. The median cubital vein lies on this deep fascia crossed superficially (or sometimes deeply) by the medial cutaneous nerve of the forearm. Brachialis and supinator form the floor of the fossa.
JOINTS
ELBOW JOINT
The elbow joint is a synovial joint. Its complexity is increased by continuity with the superior radio-ulnar joint. It includes two articulations (Fig. 48.2). These are the humero-ulnar, between the trochlea of the humerus and the ulnar trochlear notch, and the humero-radial, between the capitulum of the humerus and the radial head.
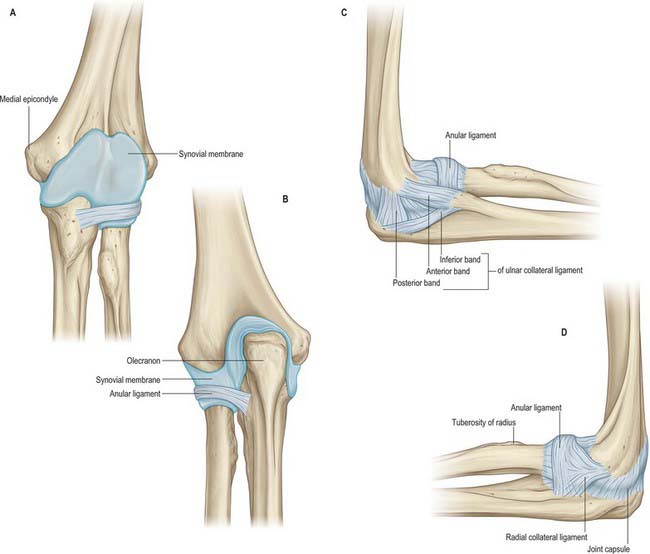
The fibrous capsule (Fig. 48.2, Fig. 48.3, 48.4) is broad and thin anteriorly. It is attached proximally to the front of the medial epicondyle and humerus above the coronoid and radial fossae, and distally to the edge of the ulnar coronoid process and anular ligament, and is continuous at its sides with the ulnar and radial collateral ligaments. Anteriorly it receives numerous fibres from brachialis. Posteriorly the capsule is thin and attached to the humerus behind its capitulum and near its lateral trochlear margin, to all but the lower part of the edge of the olecranon fossa, and to the back of the medial epicondyle. Inferomedially it reaches the superior and lateral margins of the olecranon and is laterally continuous with the superior radio-ulnar capsule deep to the anular ligament. It is related posteriorly to the tendon of triceps and to anconeus.
The humero-ulnar and humeroradial articulations have ulnar and radial collateral ligaments.
This is a triangular band, consisting of thick anterior, posterior and inferior parts united by a thin region (Fig. 48.2C). The strongest and stiffest anterior part is attached by its apex to the front of the medial epicondyle and by its broad distal base to a proximal tubercle on the medial coronoid margin. The posterior part, also triangular, is attached low on the back of the medial epicondyle and to the medial margin of the olecranon. Between these two bands intermediate fibres descend from the medial epicondyle to an inferior, oblique band, often weak, between the olecranon and coronoid processes. This converts a depression on the medial margin of the trochlear notch into a foramen, through which the intracapsular fat pad is continuous with extracapsular fat medial to the joint. The anterior band is taut throughout most of the range of flexion, while the posterior band becomes taut between half and full flexion.
This is attached low on the lateral epicondyle and to the anular ligament (Fig. 48.2D). Some of its posterior fibres cross the ligament to the proximal end of the supinator crest of the ulna. It intimately blends with attachments of supinator and extensor carpi radialis brevis. It is taut throughout most of the range of flexion.
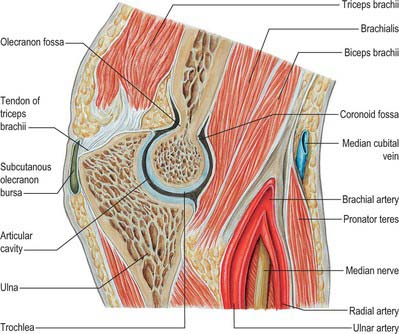
The synovial membrane (Figs 48.2–48.4) extends from the humeral articular margins, lines the coronoid, radial and olecranon fossae, the flat medial trochlear surface, the deep surface of the capsule and the lower part of the anular ligament. Projecting between the radius and ulna from behind is a crescentic synovial fold, which partly divides the joint into humero-radial and humero-ulnar parts. Irregularly triangular, it contains extrasynovial fat (Fig. 48.5). Between the capsule and synovial membrane are three other pads of fat: the largest, at the olecranon fossa, is pressed into the fossa by triceps during flexion; the other two, at the coronoid and radial fossae, are pressed in by brachialis during extension. They are all slightly displaced in contrary movements. Smaller synovial-covered tags of fat project into the joint near constrictions flanking the trochlear notch, and cover small non-articular areas of bone.
Vascular supply and lymphatic drainage
Articular arteries are derived from the numerous periarticular anastomoses (Fig. 47.6).
PROXIMAL (SUPERIOR) RADIO-ULNAR JOINT
The proximal radio-ulnar joint is a uniaxial pivot joint.
VASCULAR SUPPLY AND LYMPHATIC DRAINAGE
ARTERIES
Brachial artery
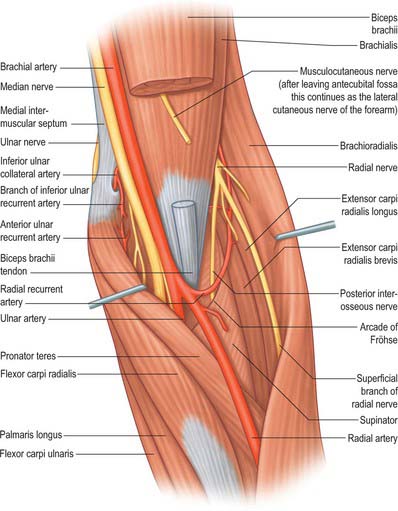
The brachial artery is central and divides near the neck of the radius into its terminal branches, namely the radial and ulnar arteries (Fig. 48.1, Fig. 48.6). The skin, superficial fascia and median cubital vein are anterior, separated by the bicipital aponeurosis. Posteriorly, brachialis separates it from the elbow joint. The median nerve is medial proximally but is separated from the ulnar artery by the ulnar head of pronator teres. Lateral are the tendon of biceps and the radial nerve, the latter concealed between supinator and brachioradialis.
Radial artery
The radial artery passes deep to brachioradialis and gives off the radial recurrent artery before continuing into the forearm (Fig. 48.1, Fig. 48.6).
The radial recurrent artery (Fig. 47.6, Fig. 48.6) arises just distal to the elbow, passing between superficial and deep branches of the radial nerve to ascend behind brachioradialis, anterior to supinator and brachialis. It supplies these muscles and the elbow joint, anastomosing with the radial collateral branch of the profunda brachii.
Ulnar artery
The ulnar artery gives off the anterior and then the posterior ulnar recurrent arteries before passing deep to pronator teres to continue its course in the forearm (Fig. 48.1, Fig. 48.6). In the forearm, the posterior interosseous artery (a branch of the ulnar artery via the common interosseous artery), gives rise to the posterior interosseous recurrent artery which passes proximally to supply the elbow region.
The common interosseous, anterior interosseous and posterior interosseous arteries, and muscular branches of the ulnar artery, are described on p. 852.
Anterior ulnar recurrent artery
The anterior ulnar recurrent artery (Fig. 47.6) arises just distal to the elbow, ascends between brachialis and pronator teres, supplies them and anastomoses with the inferior ulnar collateral artery anterior to the medial epicondyle.
Posterior ulnar recurrent artery
The posterior ulnar recurrent artery (Fig. 47.6) arises distal to the anterior ulnar recurrent, and passes dorsomedially between flexors digitorum profundus and superficialis, ascending behind the medial epicondyle; between this and the olecranon, it is deep to flexor carpi ulnaris, ascending between its heads with the ulnar nerve. It supplies adjacent muscles, nerve, bone and elbow joint, and anastomoses with the ulnar collateral and interosseous recurrent arteries (Fig. 47.6).
VEINS
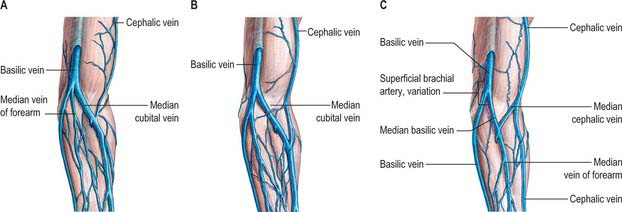
The deep and superficial veins supplying the elbow and related structures are described on page 853. Fig. 48.7 shows the common variants of the superficial veins of the cubital fossa: their easy access means that the cubital veins are common sites for venous blood puncture and intravenous fluid and drug administration.
INNERVATION
Median nerve
In the cubital fossa the median nerve lies medial to the brachial artery, deep to the bicipital aponeurosis and anterior to brachialis (Fig. 48.1, Fig. 48.6).
This is an uncommon entrapment neuropathy of the median nerve occurring in the elbow region. Entrapment can occur typically at four sites. The first occurs at the site of the ligament of Struthers. This ligament represents an anatomical variant and when present connects a small supracondylar spur of bone to an accessory origin of pronator teres. The median nerve can be compressed as it passes under this ligament. The nerve may also be trapped as it passes deep to the bicipital aponeurosis; the aponeurotic edge of the deep head of pronator teres muscle; or the tendinous aponeurotic arch forming the proximal free edge of the radial attachment of flexor digitorum superficialis.
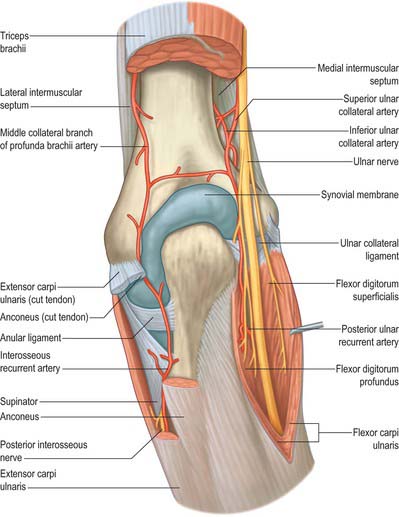
Ulnar nerve
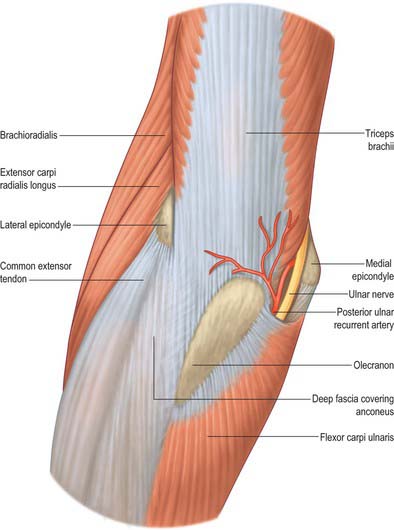
At the elbow the ulnar nerve is in a groove on the dorsum of the medial epicondyle. It enters the forearm between the two heads of flexor carpi ulnaris superficial to the posterior and oblique parts of the ulnar collateral ligament (Fig. 48.6, Fig. 48.8, Fig. 48.9).
[/level-membership-for-basic-science-category][not-level-membership-for-basic-science-category]
CHAPTER 48 Elbow
SKIN AND SOFT TISSUE
SKIN
Cutaneous vascular supply
The skin overlying the cubital fossa receives its blood supply on its anterolateral side by small perforating vessels from the radial collateral artery, together with some small musculocutaneous perforators from the radial recurrent artery which traverse brachioradialis (Fig. 45.4). On the anteromedial side, skin is supplied by small branches from the anastomosis between the inferior ulnar collateral artery and the anterior ulnar recurrent artery and by small branches from the brachial artery.
Cutaneous innervation
The skin of the cubital fossa and the epicondylar regions is innervated by the medial and lateral cutaneous nerves of the forearm (Fig. 45.15). A small proximal area on the lateral aspect is supplied by the distal part of the lower lateral cutaneous nerve of the arm. The skin over the olecranon region is innervated by the distal branches of the posterior cutaneous nerve of the arm, together with proximal branches of the posterior cutaneous nerve of the forearm.
SOFT TISSUE: CUBITAL FOSSA
The cubital fossa forms a triangular depression in the middle of the upper part of the anterior aspect of the forearm (Fig. 48.1). The superior border of the fossa is an imaginary line, which joins the two epicondyles of the humerus. The fleshy elevation which constitutes its medial border is formed by the lateral margin of pronator teres and the elevation which forms the lateral border is the medial edge of brachioradialis. The roof of the fossa is formed by the deep fascia of the forearm, reinforced by the bicipital aponeurosis on the medial aspect. The median cubital vein lies on this deep fascia crossed superficially (or sometimes deeply) by the medial cutaneous nerve of the forearm. Brachialis and supinator form the floor of the fossa.
JOINTS
ELBOW JOINT
The elbow joint is a synovial joint. Its complexity is increased by continuity with the superior radio-ulnar joint. It includes two articulations (Fig. 48.2). These are the humero-ulnar, between the trochlea of the humerus and the ulnar trochlear notch, and the humero-radial, between the capitulum of the humerus and the radial head.
The fibrous capsule (Fig. 48.2, Fig. 48.3, 48.4) is broad and thin anteriorly. It is attached proximally to the front of the medial epicondyle and humerus above the coronoid and radial fossae, and distally to the edge of the ulnar coronoid process and anular ligament, and is continuous at its sides with the ulnar and radial collateral ligaments. Anteriorly it receives numerous fibres from brachialis. Posteriorly the capsule is thin and attached to the humerus behind its capitulum and near its lateral trochlear margin, to all but the lower part of the edge of the olecranon fossa, and to the back of the medial epicondyle. Inferomedially it reaches the superior and lateral margins of the olecranon and is laterally continuous with the superior radio-ulnar capsule deep to the anular ligament. It is related posteriorly to the tendon of triceps and to anconeus.
The humero-ulnar and humeroradial articulations have ulnar and radial collateral ligaments.
This is a triangular band, consisting of thick anterior, posterior and inferior parts united by a thin region (Fig. 48.2C). The strongest and stiffest anterior part is attached by its apex to the front of the medial epicondyle and by its broad distal base to a proximal tubercle on the medial coronoid margin. The posterior part, also triangular, is attached low on the back of the medial epicondyle and to the medial margin of the olecranon. Between these two bands intermediate fibres descend from the medial epicondyle to an inferior, oblique band, often weak, between the olecranon and coronoid processes. This converts a depression on the medial margin of the trochlear notch into a foramen, through which the intracapsular fat pad is continuous with extracapsular fat medial to the joint. The anterior band is taut throughout most of the range of flexion, while the posterior band becomes taut between half and full flexion.
This is attached low on the lateral epicondyle and to the anular ligament (Fig. 48.2D). Some of its posterior fibres cross the ligament to the proximal end of the supinator crest of the ulna. It intimately blends with attachments of supinator and extensor carpi radialis brevis. It is taut throughout most of the range of flexion.
The synovial membrane (Figs 48.2–48.4) extends from the humeral articular margins, lines the coronoid, radial and olecranon fossae, the flat medial trochlear surface, the deep surface of the capsule and the lower part of the anular ligament. Projecting between the radius and ulna from behind is a crescentic synovial fold, which partly divides the joint into humero-radial and humero-ulnar parts. Irregularly triangular, it contains extrasynovial fat (Fig. 48.5). Between the capsule and synovial membrane are three other pads of fat: the largest, at the olecranon fossa, is pressed into the fossa by triceps during flexion; the other two, at the coronoid and radial fossae, are pressed in by brachialis during extension. They are all slightly displaced in contrary movements. Smaller synovial-covered tags of fat project into the joint near constrictions flanking the trochlear notch, and cover small non-articular areas of bone.
[/not-level-membership-for-basic-science-category]
