[level-membership-for-orthopaedics-category]
CHAPTER FIVE ELBOW
INTRODUCTION
When the elbow is extended, the epicondyles and the tip of the olecranon should be at the same level. In normal elbow configuration, when a line is drawn between the epicondyles, the olecranon should bisect and be on the center of the line. When the normal elbow is flexed to an angle of 90 degrees, the tip of the olecranon should be directly below to the line joining the epicondyles. If a line from the olecranon is drawn to each epicondyle, the three prominences and line should form an isosceles triangle.
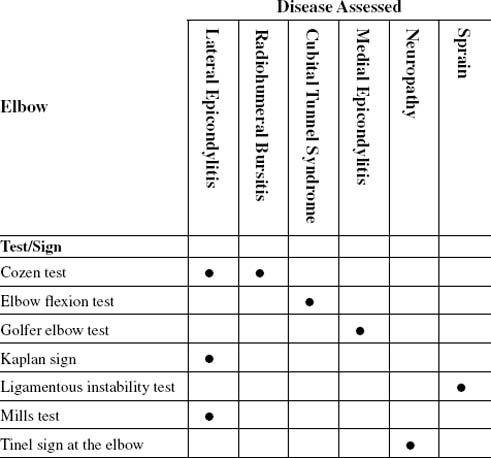
| Cubital tunnel syndrome | Elbow flexion test |
| Lateral epicondylitis |
ORTHOPEDIC GAMUT 5-1 ISOSCELES TRIANGLE OF THE ELBOW
If the angles of the isosceles triangle of the elbow are abnormal, the following may exist:
The patient may complain of sharply localized pain, typical of an extraarticular abnormality, deep joint pain, or the poorly localized pain of ulnar neuropathy with or without typical paresthesia extending to the hand. The functional interplay among the elbow, shoulder, and wrist means that examination of all of these joints may be necessary (Table 5-3). Referred pain in the elbow, especially from the neck or shoulder, is usually diffuse. Examination must include comparison of right and left arms.
TABLE 5-3 FUNCTIONAL ARC MEASUREMENTS FOR SELECTED ACTIVITIES OF DAILY LIVING
 |
From Kelley WN, et al: Textbook of rheumatology, ed 5, Philadelphia, 1997, WB Saunders.
Pain of lateral elbow origin is usually diagnosed as radiohumeral bursitis, epicondylitis, or tennis elbow. All of these problems involve the origin of the wrist extensors (tendinopathy) or, occasionally, radial nerve impingement by musculotendinous structures crossing the elbow joint.
ORTHOPEDIC GAMUT 5-4 AVASCULAR NECROSIS OF THE CAPITELLUM
Possible causes of avascular necrosis of the capitellum of the elbow (Panner disease):
ORTHOPEDIC GAMUT 5-5 HYPEREXTENSION INJURIES OF THE ELBOW
Elbow joint complaints usually consist of pain, loss of movement, weakness, clicking, or locking. The patient may complain of sharply localized pain (typical of an extraarticular abnormality), deep joint pain, or poorly localized pain of ulnar neuropathy with or without typical paresthesias extending to the hand. The functional interplay among the elbow, shoulder, and wrist means that examination of all these joints is necessary. Referred pain in the elbow, especially from the neck or shoulder, is usually diffuse (Table 5-4).
TABLE 5-4 UPPER EXTREMITY PERIARTICULAR SYNDROME DIFFERENTIAL DIAGNOSTIC LIST
| Region | Periarticular Syndrome | Monarticular Syndrome |
|---|---|---|
| Shoulder | ||
| Elbow | Ulnar nerve entrapment | |
| Wrist | Carpal tunnel syndrome | |
| Hand | Palmar fasciitis (Dupuytren contracture) | Ligamentous or capsular injury |
Modified from Kelley WN, et al: Textbook of rheumatology, ed 5, Philadelphia, 1997, WB Saunders.
The olecranon bursa is prone to injury by friction or a blow. Additionally, because of its position, swelling occurs easily and is readily visible. It is also a common site involved in crystal arthropathies (gout, or rarely, calcium pyrophosphate arthritis) or in generalized inflammatory arthritis, especially rheumatoid arthritis in which swelling of the olecranon bursa may be seen in association with rheumatoid nodules on the ulnar border of the forearm.
ESSENTIAL ANATOMY
Arterial supply to the forearm depends entirely on branches of the brachial artery. The radial artery courses to the lateral side of the forearm and aligns itself with the radius. The ulnar artery is the larger of the two branches of the brachial artery.
ESSENTIAL MOTION ASSESSMENT
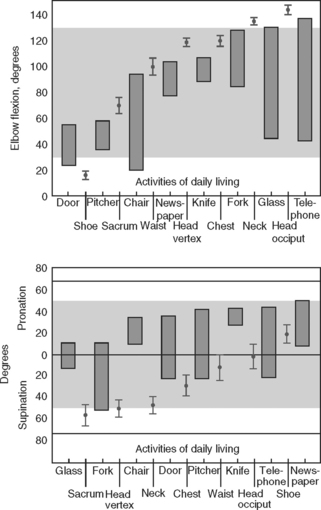
Tissue approximation limits elbow flexion to 140 to 150 degrees. Retained flexion motion of 130 degrees or less is impairment in the activities of daily living (Fig. 5-1).

Elbow extension is 0 degrees. Up to 10 degrees of hyperextension is still within normal limits if the patient has no history of trauma to the joint. The inability to return the elbow to within 10 degrees of the neutral position is impairment in the activities of daily living (Fig. 5-2).

Supination of the elbow is limited by tissue stretch to 90 degrees. Retained supination motion of 60 degrees or less is impairment in the activities of daily living (Fig. 5-3).

Elbow pronation is the same as supination, 80 to 90 degrees. Retained pronation motion of 70 degrees or less is impairment in the activities of daily living (Fig. 5-4).

ESSENTIAL MUSCLE FUNCTION ASSESSMENT
The prime movers in flexion of the elbow are the biceps brachii (musculocutaneous nerve, C5, and C6), brachialis (musculocutaneous nerve, C5, and C6), and brachioradialis (radial nerve, C5, and C6) muscles. The flexor muscles of the forearm arising from the medial epicondyle of the humerus are the accessory muscles (Fig. 5-5).

The prime mover in extension of the elbow is the triceps brachii muscle (radial nerve, C7, and C8); the anconeus muscle is an accessory. When the arm is horizontally abducted, the long head of the triceps is shortened over the shoulder joint. When the shoulder is flexed, the long head of the triceps is shortened over the elbow joint and elongated over the shoulder joint (Fig. 5-6).

Although the triceps and anconeus act together in extending the elbow joint, the two muscles can be differentiated. The belly of the anconeus muscle is below the elbow joint and is easily distinguished from the triceps by palpation. Paralysis of the anconeus materially reduces the strength of elbow extension (Fig. 5-7).

The primary supinators are the biceps brachii and the supinator. The accessory muscle in this movement is the brachioradialis. In addition to its role in supination, the biceps also functions as an elbow flexor. Its total biceps function is well illustrated in the act of twisting a corkscrew into the cork of a bottle and then pulling the cork out of the bottle (Fig. 5-8).

The primary pronators are the pronator teres and the pronator quadratus. The accessory muscle in this movement is the flexor carpi radialis. Pronation and supination are complex movements (Fig. 5-9) that occur simultaneously around an axis best described as an imaginary line between the head of the radius proximally and the medial end of the triangular articular disc distally. In the proximal radioulnar joint, the head of the radius can rotate within the perimeter created by the annular ligament.

ESSENTIAL IMAGING
COZEN TEST
Assessment for Lateral Epicondylitis and Radiohumeral Bursitis
Comment
Because of the proximity of the epicondyle, the radiohumeral joint, and the supinator aponeurosis, diagnosis of exact tissue involvement can be confusing. In many instances, the conditions are caused by the same mechanisms, overuse of the elbow joint (Table 5-5).
TABLE 5-5 CONDITIONS MIMICKING OR CONTRIBUTING TO CHRONIC LATERAL EPICONDYLITIS
Adapted from Greenfield C, Webster V: Chronic lateral epicondylitis: survey of current practice in the outpatient departments in Scotland, Physiotherapy 88(10):578-594, 2002.
PROCEDURE

ELBOW FLEXION TEST (WADSWORTH ELBOW FLEXION TEST)
PROCEDURE

PROCEDURE

KAPLAN SIGN
PROCEDURE

PROCEDURE



TINEL SIGN AT THE ELBOW (ALSO KNOWN AS FORMICATION SIGN, DISTAL TINGLING ON PERCUSSION [DTP] SIGN, AND HOFFMAN-TINEL SIGN)
PROCEDURE

[/level-membership-for-orthopaedics-category][not-level-membership-for-orthopaedics-category]
CHAPTER FIVE ELBOW
INTRODUCTION
When the elbow is extended, the epicondyles and the tip of the olecranon should be at the same level. In normal elbow configuration, when a line is drawn between the epicondyles, the olecranon should bisect and be on the center of the line. When the normal elbow is flexed to an angle of 90 degrees, the tip of the olecranon should be directly below to the line joining the epicondyles. If a line from the olecranon is drawn to each epicondyle, the three prominences and line should form an isosceles triangle.
| Cubital tunnel syndrome | Elbow flexion test |
| Lateral epicondylitis |
ORTHOPEDIC GAMUT 5-1 ISOSCELES TRIANGLE OF THE ELBOW
If the angles of the isosceles triangle of the elbow are abnormal, the following may exist:
The patient may complain of sharply localized pain, typical of an extraarticular abnormality, deep joint pain, or the poorly localized pain of ulnar neuropathy with or without typical paresthesia extending to the hand. The functional interplay among the elbow, shoulder, and wrist means that examination of all of these joints may be necessary (Table 5-3). Referred pain in the elbow, especially from the neck or shoulder, is usually diffuse. Examination must include comparison of right and left arms.
TABLE 5-3 FUNCTIONAL ARC MEASUREMENTS FOR SELECTED ACTIVITIES OF DAILY LIVING
|
From Kelley WN, et al: Textbook of rheumatology, ed 5, Philadelphia, 1997, WB Saunders.
Pain of lateral elbow origin is usually diagnosed as radiohumeral bursitis, epicondylitis, or tennis elbow. All of these problems involve the origin of the wrist extensors (tendinopathy) or, occasionally, radial nerve impingement by musculotendinous structures crossing the elbow joint.
ORTHOPEDIC GAMUT 5-4 AVASCULAR NECROSIS OF THE CAPITELLUM
Possible causes of avascular necrosis of the capitellum of the elbow (Panner disease):
ORTHOPEDIC GAMUT 5-5 HYPEREXTENSION INJURIES OF THE ELBOW
Elbow joint complaints usually consist of pain, loss of movement, weakness, clicking, or locking. The patient may complain of sharply localized pain (typical of an extraarticular abnormality), deep joint pain, or poorly localized pain of ulnar neuropathy with or without typical paresthesias extending to the hand. The functional interplay among the elbow, shoulder, and wrist means that examination of all these joints is necessary. Referred pain in the elbow, especially from the neck or shoulder, is usually diffuse (Table 5-4).
TABLE 5-4 UPPER EXTREMITY PERIARTICULAR SYNDROME DIFFERENTIAL DIAGNOSTIC LIST
| Region | Periarticular Syndrome | Monarticular Syndrome |
|---|---|---|
| Shoulder | ||
| Elbow | Ulnar nerve entrapment | |
| Wrist |
