5 Echocardiographic Evaluation of Prosthetic Valves
Introduction
Key Points
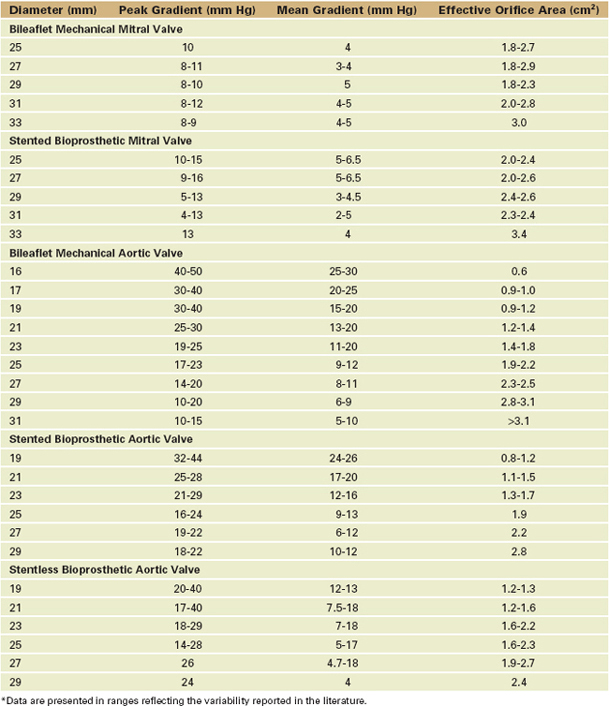
Because there are so many available prosthetic valves, each with very distinctive two-dimensional (2D) and color flow (CF) Doppler acoustic profiles (Table 5-1), the echocardiographer should have access to the type and size of the in situ prosthetic valve and the reason the study has been ordered to focus the study and facilitate image interpretation.
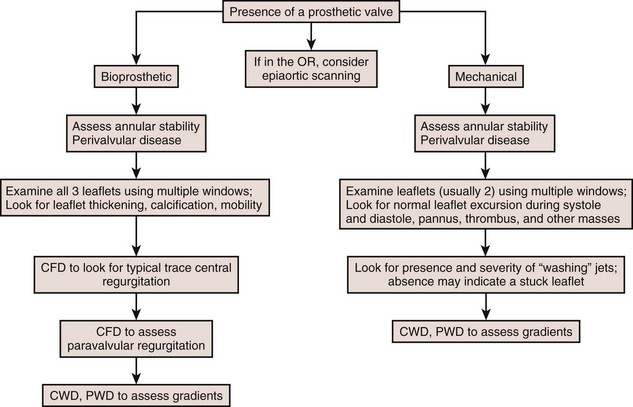
General Considerations With Prosthetic Valves (Figure 5-1)
Types of Prosthetic Valves
Prosthetic valves are usually broadly grouped as biologic or mechanical.
Bioprosthetic Valves (Figure 5-2)
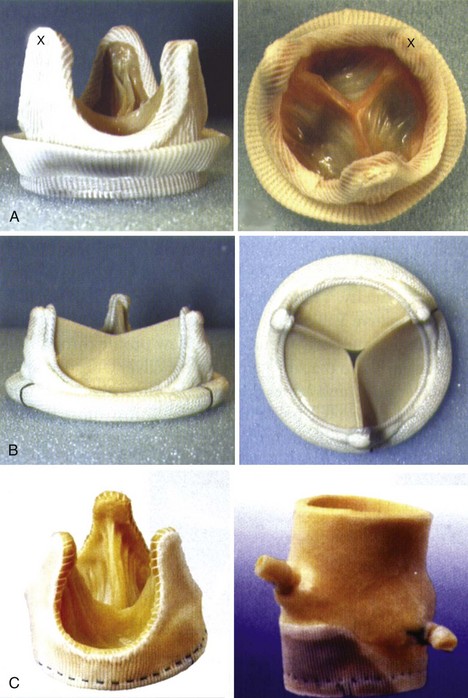
Stented Bioprosthesis
Stentless Bioprosthesis
In this category, we take liberty by including all replacement tissues without a prosthetic stent. These include the better known stentless valves by St. Jude Medical and Medtronic (see Figure 5-2) as well as autograft and homograft tissues.
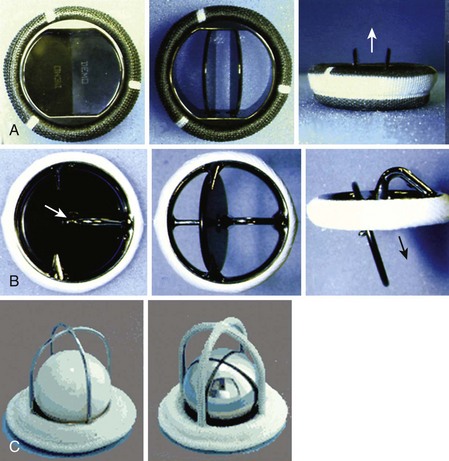
Mechanical Valves (Figure 5-3)
Basic Principles Of The Echocardiographic Examination
Two-Dimensional
Doppler Echocardiography
Color Flow Doppler
Mechanical Valves
Bioprosthetic Valves
General Points Regarding Color Doppler Assessment
Pulsed Wave and Continuous Wave Doppler





General Points
Key Points
Prosthetic Mitral Valve
Key Points
Step-by-Step Examination (Figure 5-4)
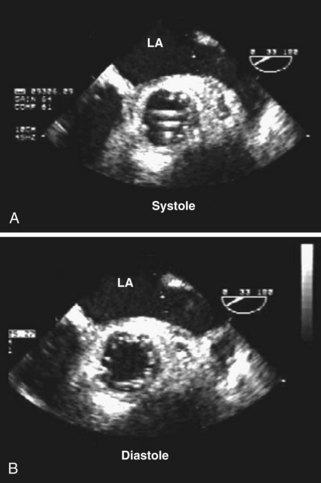
Step 1: Two-Dimensional Examination (Figure 5-7; see also Figure 5-4)

Step 2: Doppler Examination (Figures 5-8 and 5-9)

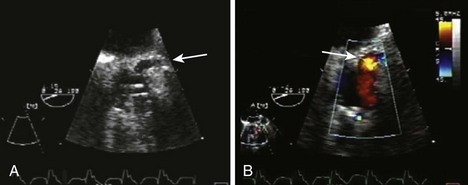
Regurgitant Flow: Normal versus Abnormal (Table 5-2; see also Figures 5-4, 5-8, and 5-9)

Forward Flow: Normal vs. Abnormal (Table 5-3; see also Figures 5-4, 5-5, and 5-7 to 5-9)
Qualitative Assessment
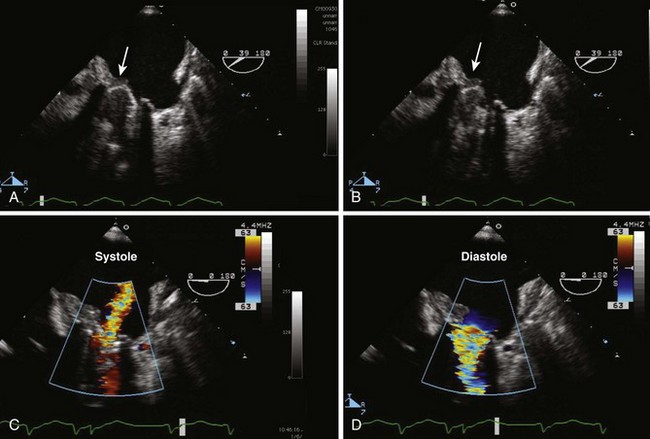
Left Ventricular Outflow Obstruction after Mitral Surgery
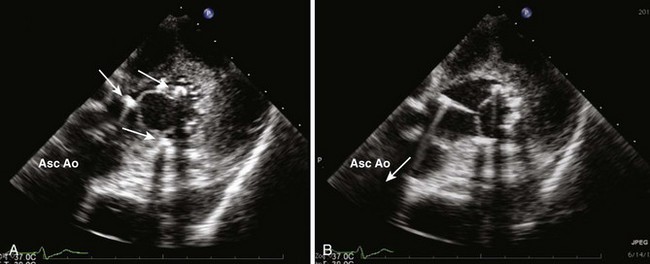
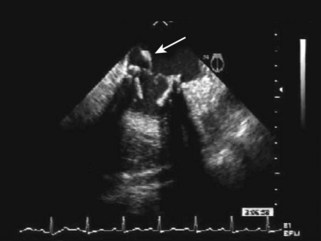
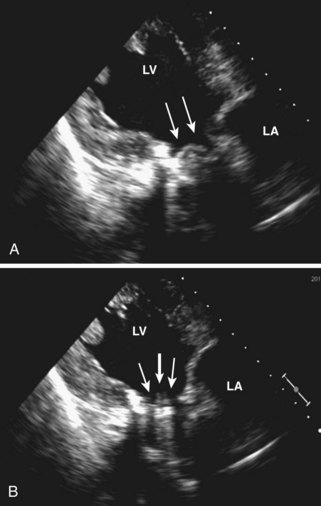
An unusual type of obstruction is obstruction of the LVOT. This can result from attempts to retain native mitral tissues (leaflets or chordae) between the mitral annulus and the prosthetic ring. This is done to preserve ventricular geometry and reduce future negative remodeling. As an unusual consequence, these native tissues may become loose and lie in the LVOT, causing a dynamic and/or fixed obstruction to systolic outflow (Figure 5-18). Another cause of obstruction can result from placement of the struts of the bioprosthetic valve in the LVOT in a relatively small ventricle. Assessment of this complication may be difficult using ME imaging as a result of shadowing; therefore, TG imaging may be necessary (see Figures 5-5 and 5-6).
Prosthetic Aortic Valve
Key Points
Step-by-Step Examination

The Echocardiographer Should
Step 1: Two-Dimensional Examination
Step 2: Doppler Examination
Regurgitant Flow: Normal versus Abnormal (Table 5-4)
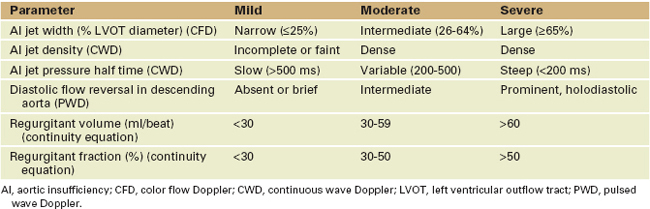
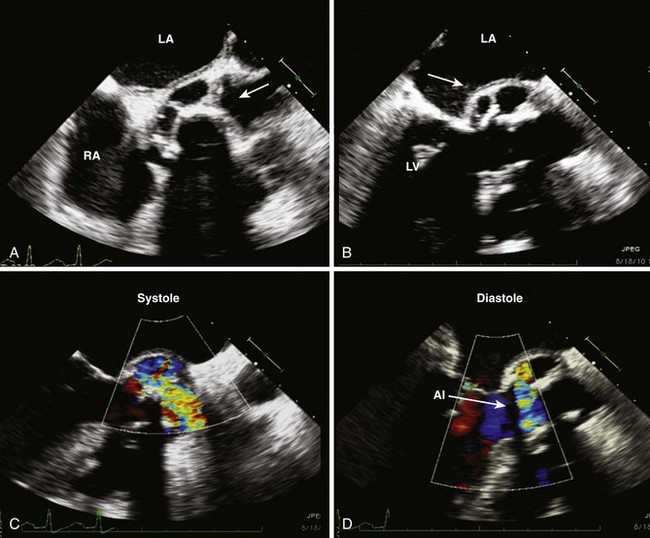
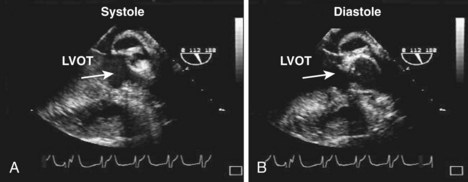
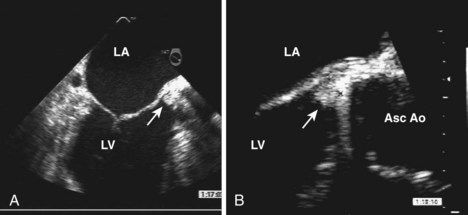
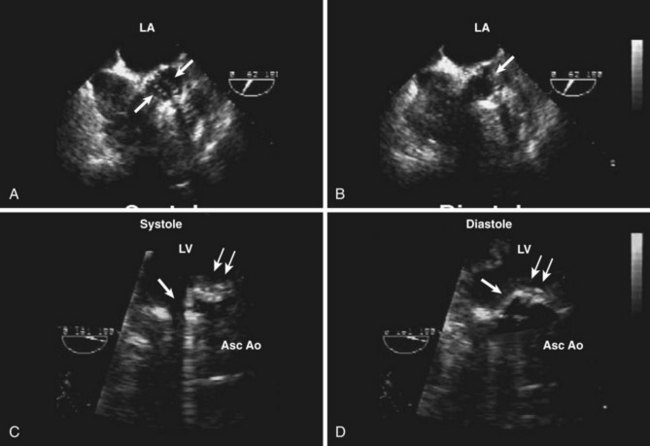
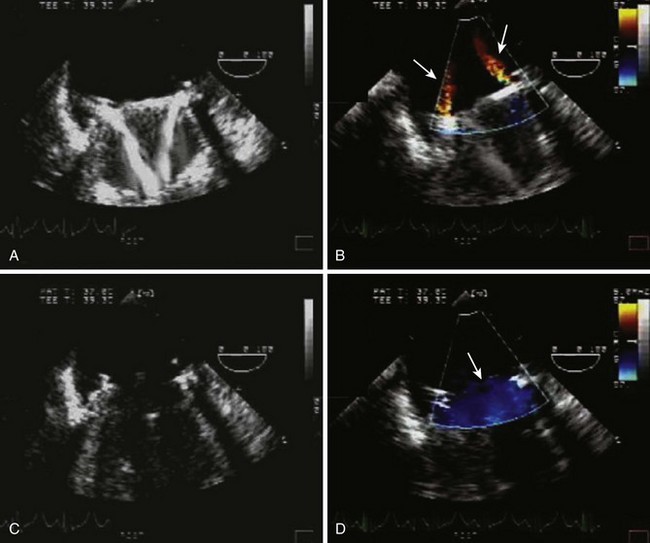
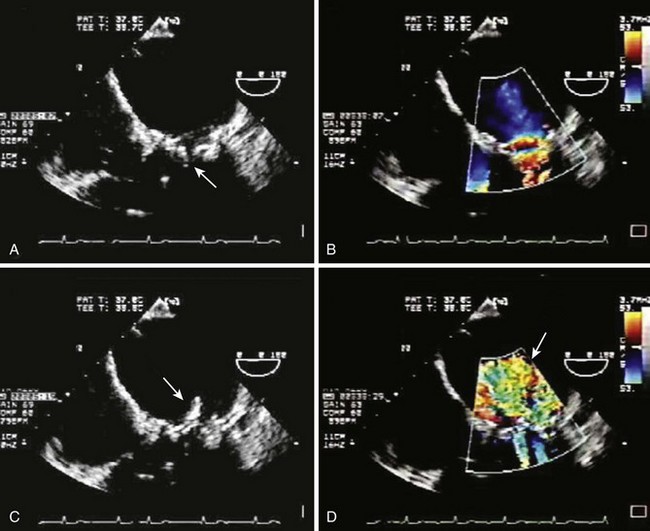
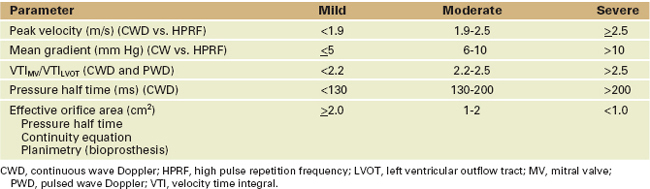
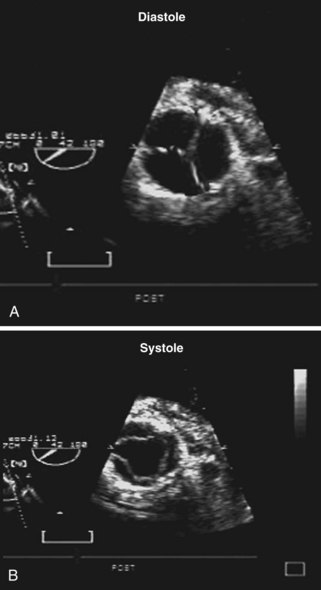
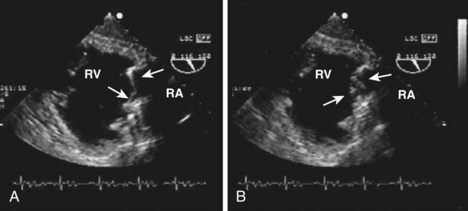
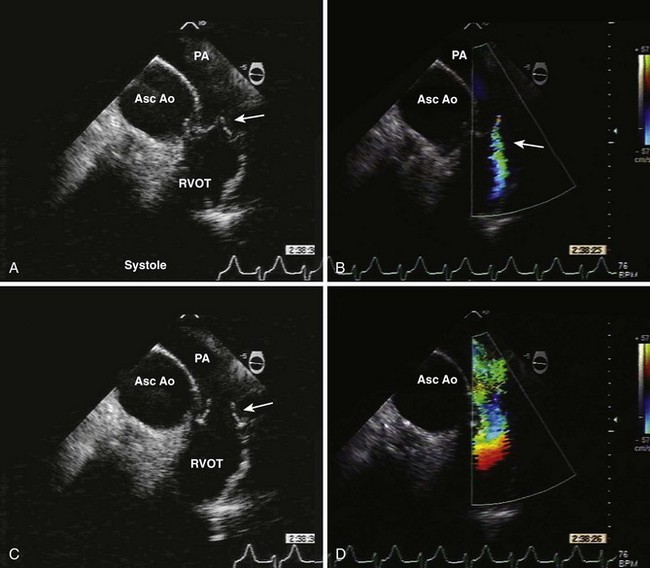
Figure 5-32 Stuck mechanical leaflet in the aortic position. Four images demonstrate restricted motion of one mechanical leaflet of the prosthetic AV. A and B, Short axis images of the mechanical valve. A, The two leaflet edges (arrows) are seen as also noted in Figure 5-19. However, in B, a leaflet edge (arrow) is still seen during diastole. C and D, TG imaging with the transducer rotated to 160 degrees. C, A single leaflet open (single arrow) while the other leaflet (double arrow) is stuck in an intermediate position. D, The mobile leaflet is shown to be closed and the stuck leaflet to be unchanged.
Forward Flow: Normal versus Abnormal (Table 5-5)
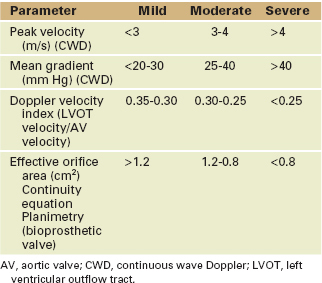
Quantitative Assessment
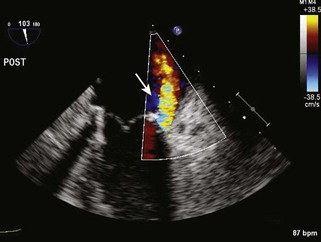
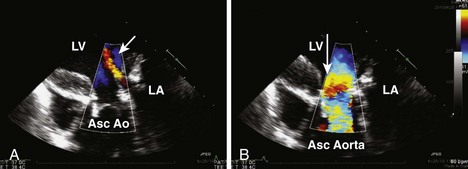
Doppler assessment of forward flow across the prosthetic AV is the standard to evaluate valve patency. However, a host of variables affect the Doppler data. These include changes in cardiac loading conditions, coexisting lesions that affect forward flow across the valve, or the pressure gradient between the left ventricle and ascending aorta. These include, but are not limited to, left ventricular failure (decreased forward flow), AI (increased forward flow), MR (decrease forward flow), and atrial arrhythmias (reduced LV preload) (Figures 5-34 and 5-35; see also Figure 5-27).
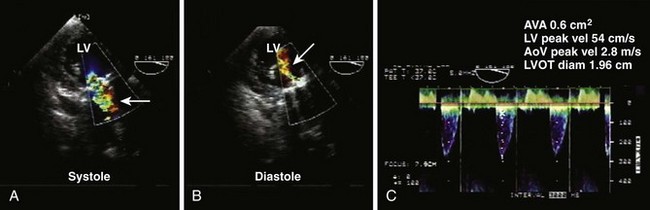
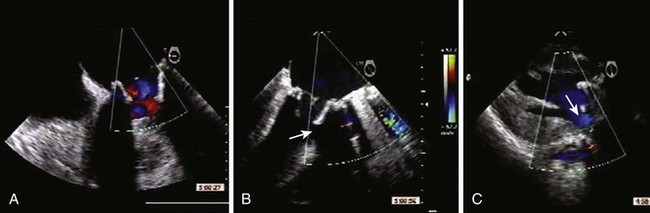
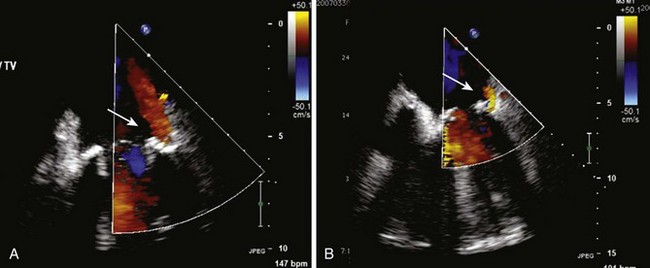
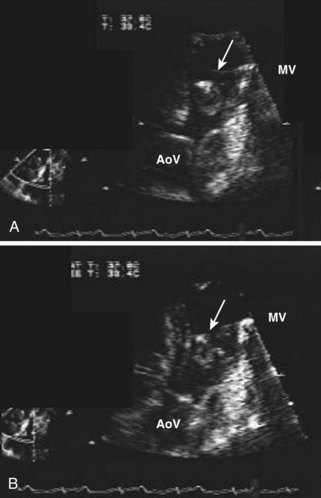
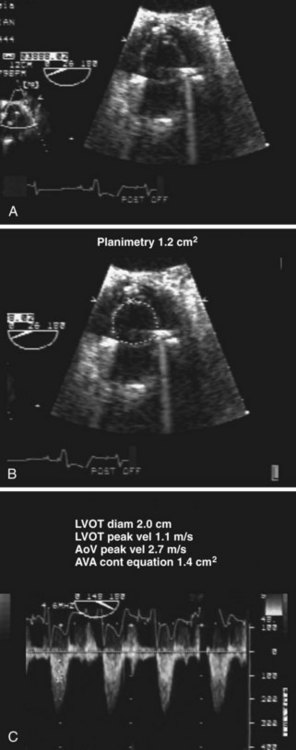
Figure 5-34 Stuck mechanical leaflet. These three TG images allow both qualitative and quantitative assessment of the same patient in Figure 5-32. A, Forward flow (arrow) is seen across the mobile leaflet. B, An abnormal regurgitant jet (arrow) coming from the stuck leaflet in the intermediate position. C, Significant AV stenosis with an AVA of 0.6 cm2.
Prosthetic Tricuspid Valve
Key Points
Step-by-Step Examination
Step 1: Two-Dimensional Examination
Step 2: Doppler Examination
Regurgitant Flow: Normal versus Abnormal (Table 5-6)
Forward Flow: Normal versus Abnormal (Table 5-7)
| Parameter | Normal | Abnormal |
|---|---|---|
| Peak velocity (m/s) (CWD) | ≤1.7 | >1.7 |
| Mean gradient (mm Hg) (CWD) | <5-6 | >7 |
| Pressure half time (ms) (CWD) | <200 | >230 |
| Size of vena cava (cm) | ≤1.5 with respiratory variation | >2.0 without respiratory variation |
CWD, continuous wave Doppler.
Normal Flows
Prosthetic Pulmonary Valve
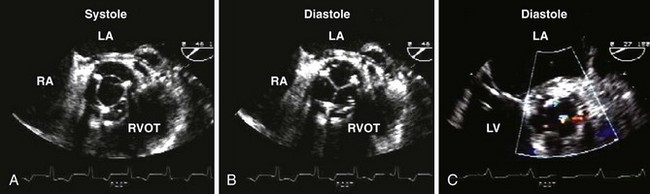
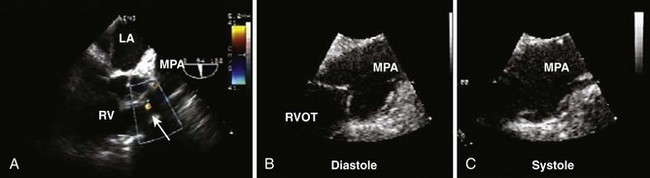
Before evaluating the prosthetic PV, it is important to know what kind of valve was placed, and to have some prior knowledge of how the images should appear. The majority of valves are either stented or stentless (xenografts) bioprosthetic valves. There is a lack of data regarding prosthetic valve function in the pulmonic position. Determination of what is normal and abnormal parallels that of normal native valve function (Figures 5-39 and 5-40).
Step-by-Step Examination
Step 1: Two-Dimensional Examination
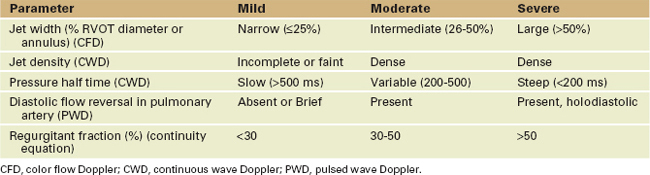
Regurgitant Flow: Normal versus Abnormal (Table 5-8)
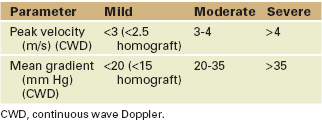
Forward Flow: Normal versus Abnormal (Table 5-9)
1 Zoghbi WA, Enriquez-Sarano M, Foster E, et al. American Society of Echocardiography. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr. 2003;16:777-802.
2 Baumgartner H, Jung J, Bermejo J, et al. Echocardiographic assessment of valve stenosis: EAE/ASE recommendation for clinical practice. J Am Soc Echocardiogr. 2009;22:1-23.
3 Zoghbi WA, Chambers JB, Dumesnil JG, et al. Recommendations for evaluation of prosthetic valves with echocardiography and Doppler ultrasound. J Am Soc Echocardiogr. 2009;22:975-1014.
Three invaluable references in the management of patients with valvular heart disease.
4 Rosenhek R, Binder T, Maurer G, Baumgartner H. Normal values for Doppler echocardiographic assessment of heart valve prostheses. J Am Soc Echocardiogr. 2003;16:1116-1127.
An important reference for Doppler values of commonly used prosthetic valves.
5 Goetze S, Brechtken J, Agler DA, et al. In vivo short-term Doppler hemodynamic profiles of 189 Carpentier-Edwards Perimount pericardial bioprosthetic valves in the mitral position. J Am Soc Echocardiogr. 2004;17:981-987.
6 Maslow AD, Haering JM, Heindel S, et al. An evaluation of prosthetic aortic valves using transesophageal echocardiography: the double-envelope technique. Anesth Analg. 2000;91:509-516.
7 Chafizadeh ER, Zoghbi WA. Doppler echocardiographic assessment of the St. Jude Medical prosthesis valve in the aortic position using the continuity equation. Circulation. 1991;83:213-223.
8 Wiseth R, Levang OW, Sande E, et al. Hemodynamic evaluation by Doppler echocardiography of small (less than or equal to 21 mm) prostheses and bioprostheses in the aortic valve position. Am J Cardiol. 1992;70:240-246.