Chapter 15 Early Pregnancy
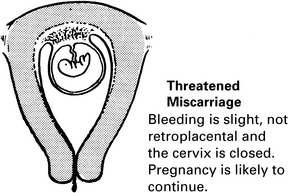
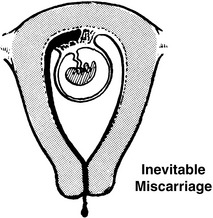
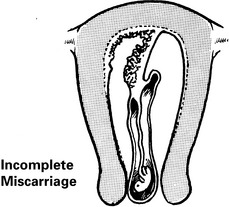
Miscarriage
Management
Early pregnancy loss (≤12Weeks’ Gestation)
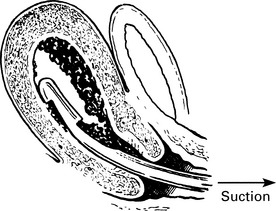
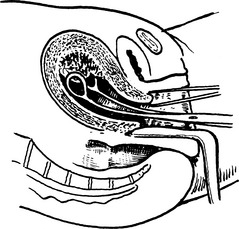
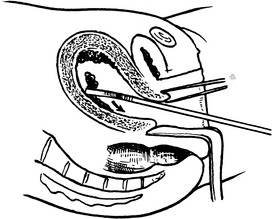
Surgical Evacuation of the Products of Conception
Complications
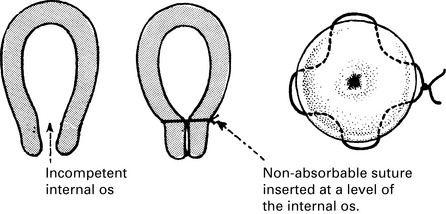
Recurrent miscarriage
Causes of recurrent miscarriage
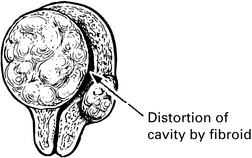
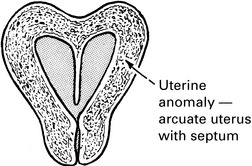
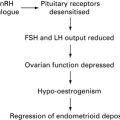
Endocrine Factors
Termination of pregnancy
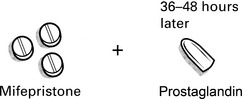
First trimester termination of pregnancy
In the first trimester of pregnancy termination can be carried out by surgical or medical methods.
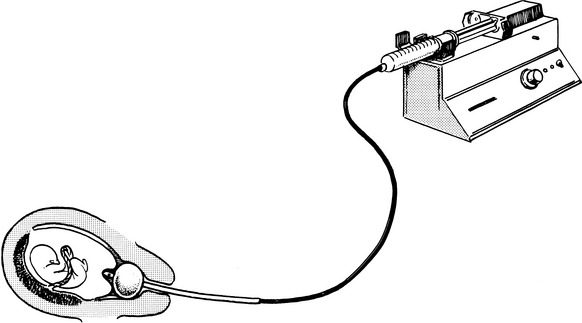
Second trimester termination of pregnancy
This method may be used if the mifepristone and prostaglandin pessaries are unavailable.
PGE2 is very slowly instilled into the cervix through a Foley catheter.
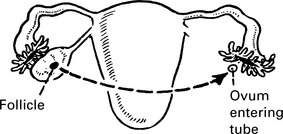
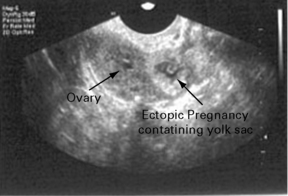
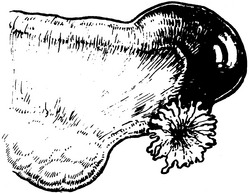
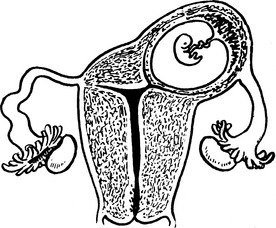
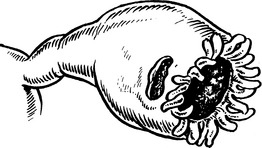
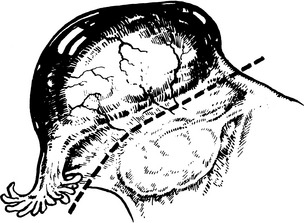
Ectopic pregnancy
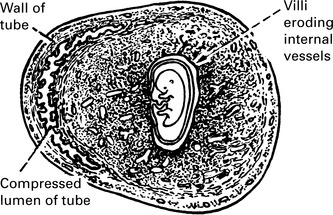
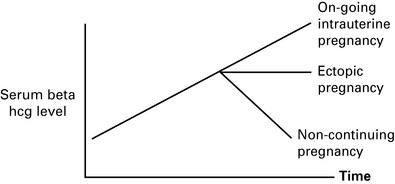
Diagnosis of tubal pregnancy
Diagnosis of tubal pregnancy
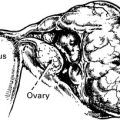
Sites of implantation

Gestational trophoblastic disease
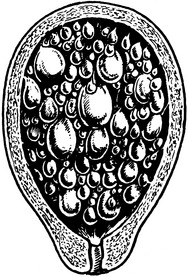
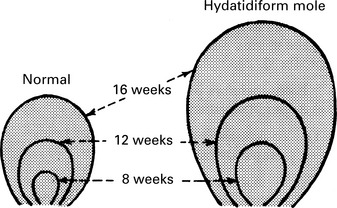
Hydatidiform Mole
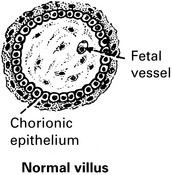
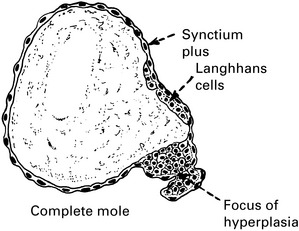
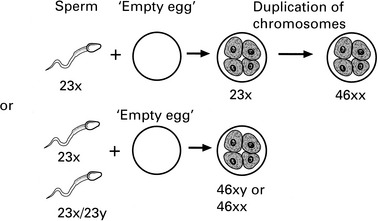
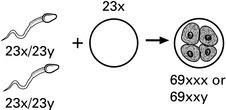
Table 15.1 Features of Partial and Complete Hydatidiform Moles
| Feature | Partial mole | Complete mole |
|---|---|---|
| Karyotype | Most commonly | Most commonly |
| 69, XXX or –, XXY | 46, XX or –, XY | |
| Pathology | ||
| Fetus | Often present | Absent |
| Amnion, fetal RBC | Usually present | Absent |
| Villous edema | Variable, focal | Diffuse |
| Trophoblastic proliferation | Focal, slight–moderate | Diffuse, slight–severe |
| Clinical presentation | ||
| Diagnosis | Missed miscarriage | Molar gestation |
| Uterine size | Small for dates | 50% large for dates |
| Theca lutein cysts | Rare | 25–30% |
| Medical complications | Rare | 10–25% |
| Post-molar GTN | 2.5–7.5% | 6.8–20% |
RBC, red blood cells; GTN, gestational trophoblastic neoplasia.
(From DISAIA Clinical Gynecologic Oncology 7E Mosby 2007)
Gestational trophoblastic disease – presentation and genetics
Presentation
The degree of bleeding is variable but can be significant.
This is related to high levels of serum βHCG.
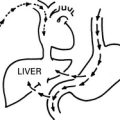
βHCG is a thyrotropic molecule and when in excess, they bind to the TSH receptor
Gestational trophoblastic disease – treatment
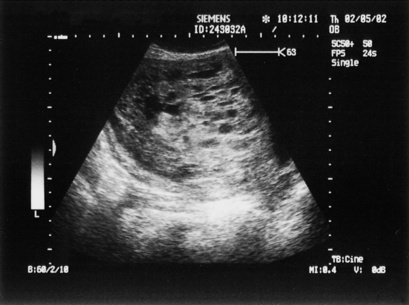
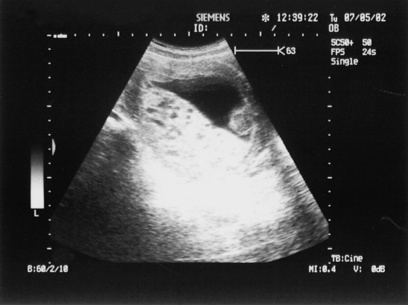
The diagnosis is made using an ultrasound (see p. 326) and βHCG levels. Partial moles may appear as a missed miscarriage and may not detected until the pathology is available. If a molar pregnancy is suspected, then uterine evacuation should be performed.