24 Earlobe rejuvenation
Summary and Key Features
Anatomy and classification of earlobes
The earlobe is composed of tough areolar and adipose connective tissues and lacks the firmness and elasticity of the rest of the pinna. Earlobes have a tendency to elongate slightly with age. The surgery literature places an emphasis on repairing the elongated earlobe to complement the youthful face after a rhytidectomy. As early as 1972, Loeb recognized the potential need for earlobe rejuvenation. He described the distance between the intertragal notch and the otobasion inferius (the anterior implantation of the earlobe to the cheek skin) as a parameter requiring evaluation (Fig. 24.1). In his observations, he noted a range of 1–2.5 cm between the intertragal notch and the otobasion inferius (attached anterior segment; Fig. 24.1) and advocated correction when this distance exceeded 2.0 cm. A large study by Azaria et al (2003), which focused on the anatomy of the earlobe, used a line of balance through the long axis of the ear and measured the earlobe length based on the distance from the intertragic notch to the caudal tip (Fig. 24.2). The study consisted of 547 adult subjects ranging in age from 20 to 80 years. The subjects included 383 women (70%) and 164 men (30%). The average length of the left earlobe was 1.97 cm and that of the right earlobe 2.01 cm. From the data, the earlobes are naturally found to be slightly asymmetrical, which becomes clinically relevant so that the practitioner carefully assesses the size of each earlobe prior to treatment. Another study suggested that a complete assessment of earlobe height requires accounting for the entire lobule length as designated by its two components: the attached cephalic segment (the intertragal notch to otobasion inferius distance as described by Loeb), as well as its free caudal segment, which is the otobasion inferius to subaurale distance (see Fig. 24.1). Both measurements can be taken into consideration; however, it is more common to measure the earlobe length from the intertragal notch to the subaurale.
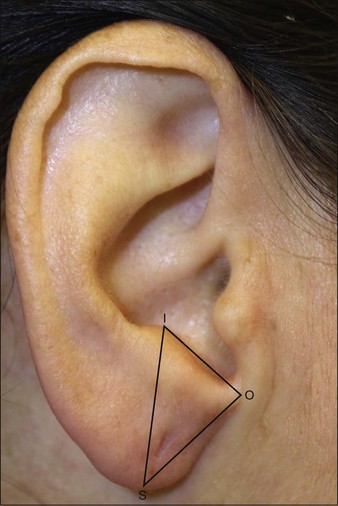

Figure 24.2 Measurement technique of earlobes: line of balance (line A) and earlobe length (line B).
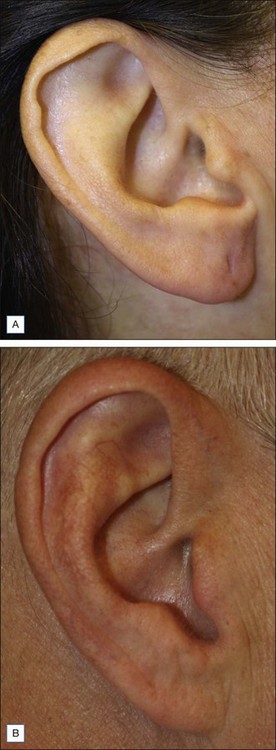
The shape of the earlobe is normally smooth but occasionally exhibits creases. Creased earlobes are associated with genetic disorders, including Beckwith–Wiedemann syndrome. Recently, diagonal earlobe creases have been associated with an increased risk of heart attack and coronary heart disease. However, since earlobes become more creased over time and heart disease is more common among the elderly, age may account for the findings linking heart attack risk to earlobe creases. The earlobe shape can be classified as being attached or unattached (Fig. 24.3). The unattached earlobe is controlled by a dominant gene, while the attached earlobe is inherited in a recessive pattern. Patients with the attached pattern have a lesser tendency to experience elongation.
Use of fillers for earlobe rejuvenation
 -inch (1.25 cm) needle for the injections. The author recommends placing the needle into the mid-dermis at a 30–45° angle to fill the earlobe. The suggested techniques include a series of small injections or a threading technique where the needle is withdrawn as the hyaluronic acid is injected. After the injection, the earlobe can be gently massaged to evenly distribute the product.
-inch (1.25 cm) needle for the injections. The author recommends placing the needle into the mid-dermis at a 30–45° angle to fill the earlobe. The suggested techniques include a series of small injections or a threading technique where the needle is withdrawn as the hyaluronic acid is injected. After the injection, the earlobe can be gently massaged to evenly distribute the product.Pearl 3
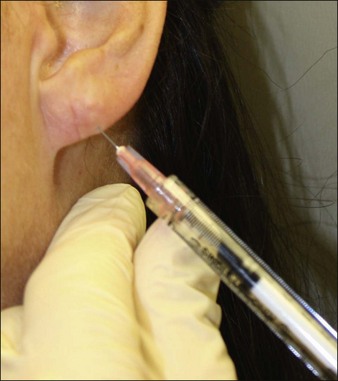
In our experience, topical anesthesia is not usually necessary, especially with the use of hyaluronic acid formulations that contain anesthesia. Needle gauge is up to the injector’s preference. We use between 27- and 30-gauge needles depending on the product selected, the patient, the earlobe, and the injector. The injection can be made from the inferior pole of the earlobe as a depot injection and then massaged into place (Fig. 24.4). The exact volume depends on the amount of volume loss. We have found that use of hyaluronic acid in the earlobes tends to last longer than its placement in the face.
Case Study 1
Earlobe Rejuvenation
A 46-year-old woman presented with thinning and elongation of her left earlobe. She had earlobe repair surgery 1 year prior to correct a tear in the lobule, and since then she had noticed the thinning. She was concerned about developing another tear, and she had earlobe rejuvenation with Restylane-L. The earlobe was cleansed with alcohol, and the earlobe with stabilized with injector’s non-dominant hand. A 28-gauge needle was used for the injection. The hyaluronic acid was injected from the inferior pole of the earlobe as a depot injection and then massaged into place (Fig. 24.4). A total of 0.3 mL of hyaluronic acid was used to obtain a full appearance in the earlobe.
Azaria R, Adler N, Silfen R, et al. Morphometry of the adult human earlobe: a study of 547 subjects and clinical application. Plastic and Reconstructive Surgery. 2003;111(7):2398–2402.
De Oliveria Monteiro E. Hyaluronic acid for restoring earlobe volume. Skin Medicine. 2006:293–294.
Farkas LG. Anthropometry of the normal and defective ear. Clinical Plastic Surgery. 1990;17:213.
Friedlander AH, Lopez-Lopez J, Velasco-Oretga E. Diagonal ear lobe crease and atherosclerosis: a review of the medical literature and dental implications. Medicina Oral, Patologia Oral, Cirugia Bucal. 2012;17(1):e153–159.
Hotta T. Earlobe rejuvenation. Plastic Surgery Nursing. 2011;31(1):39–40.
Loeb R. Earlobe tailoring during facial rhytidoplasties. Plastic and Reconstructive Surgery. 1972;49:485–488.
Mowlavi A, Meldrum D, Wilhelmi B, et al. Incidence of earlobe ptosis and pseudoptosis in patients seeking facial rejuvenation surgery and effects of aging. Plastic and Reconstructive Surgery. 2004;113(2):712–717.
Mowlavi A, Meldrum DG, Wilhelmi BJ, et al. Effect of face lift on earlobe ptosis and pseudoptosis. Plastic and Reconstructive Surgery. 2004;114(4):988–991.