[level-membership-for-internal-medicine-category]
57 Dystrophia myotonica
Salient features
History
• Onset usually in the third and fourth decade. However, if the mother is the carrier then the disease may manifest in infancy and undergo rapid deterioration at the usual age of onset
• Onset dominated by weakness or myotonia or both
• Difficulty in releasing grip
• Leg weakness (difficulty in kicking a ball)
• ‘Pseudo-drop attacks’ (caused by weakness of quadriceps muscle)
• Ask the patient if they have dysphagia (oesophageal involvement)
• Impotence (caused by gonadal atrophy)
• Recurrent respiratory infections (caused by weakness of muscles of bronchioles)
Examination
• While shaking hands with the patient, note the myotonia
• Frontal baldness (the patient may be wearing a wig and it is important to mention if this is so)
• Ptosis (bilateral or unilateral) with a smooth forehead
• Cataracts (posterior capsular cataracts) or evidence of surgery for cataracts
• Difficulty in opening the eyes after firm closure
• Expressionless face (‘hatchet face’; Fig. 57.1) with wasting of temporalis, masseters and sternomastoids and ‘swan neck’ caused by thinning of the neck.
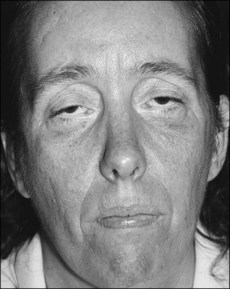
Fig. 57.1 Muscle wasting in myotonic dystrophy gives the characteristic drawn appearance of ‘hatchet facies.’
(With permission from Yanoff, Duker 2008.)
Remember: Respiratory failure is the commonest cause of death.
Advanced-level questions
What are the other features of this condition?
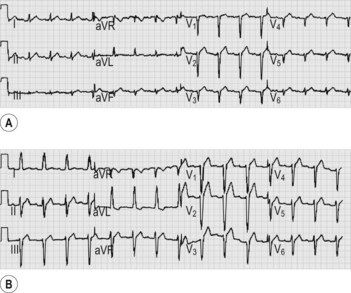
• Cardiomyopathy and cardiac conduction defects (Fig. 57.2). A severe abnormality on the ECG and a diagnosis of an atrial tachyarrhythmia predict sudden death (N Engl J Med 2008;358:2688–97). An implantable cardioverter defibrillator should be considered in all patients
How would you manage such patients?
• Foot drop is controlled by calipers or molded-foot orthoses.
• Myotonia when disabling may respond to phenytoin (avoid quinidine and procainamide as they can worsen cardiac conduction).
• Advanced heart block with or without syncope should be considered for pacemaker insertion.
[/level-membership-for-internal-medicine-category][not-level-membership-for-internal-medicine-category]
57 Dystrophia myotonica
Salient features
History
• Onset usually in the third and fourth decade. However, if the mother is the carrier then the disease may manifest in infancy and undergo rapid deterioration at the usual age of onset
• Onset dominated by weakness or myotonia or both
• Difficulty in releasing grip
• Leg weakness (difficulty in kicking a ball)
• ‘Pseudo-drop attacks’ (caused by weakness of quadriceps muscle)
• Ask the patient if they have dysphagia (oesophageal involvement)
• Impotence (caused by gonadal atrophy)
• Recurrent respiratory infections (caused by weakness of muscles of bronchioles)
Examination
• While shaking hands with the patient, note the myotonia
• Frontal baldness (the patient may be wearing a wig and it is important to mention if this is so)
• Ptosis (bilateral or unilateral) with a smooth forehead
• Cataracts (posterior capsular cataracts) or evidence of surgery for cataracts
• Difficulty in opening the eyes after firm closure
• Expressionless face (‘hatchet face’; Fig. 57.1) with wasting of temporalis, masseters and sternomastoids and ‘swan neck’ caused by thinning of the neck.
Fig. 57.1 Muscle wasting in myotonic dystrophy gives the characteristic drawn appearance of ‘hatchet facies.’
(With permission from Yanoff, Duker 2008.)
Remember: Respiratory failure is the commonest cause of death.
