Hamid, S, et al. Frequency of NSAID induced peptic ulcer disease. J Pak Med Assoc. 2006; 56(5):218–222.
Pun, E, et al. Computed tomography and complicated peptic ulcer disease. Australas Radiol. 2004; 48(4):516–519.
Luzi, G, et al. Duodenal pathology and clinical-immunological implications in common variable immunodeficiency patients. Am J Gastroenterol. 2003; 98(1):118–121.
O’Connor, AS, et al. Pancreatitis and duodenitis from sarcoidosis: successful therapy with mycophenolate mofetil. Dig Dis Sci. 2003; 48(11):2191–2195.
Shankar, RR, et al. Erosive gastroduodenitis and Helicobacter pylori infection. Med Sci Monit. 2003; 9(6):CR222–CR224.
Long, FR, et al. Duodenitis in children: correlation of radiologic findings with endoscopic and pathologic findings. Radiology. 1998; 206(1):103–108.







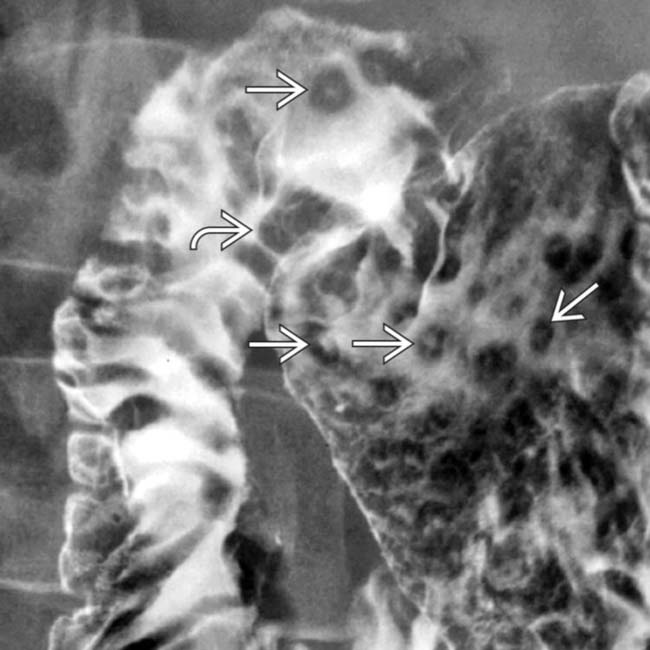
 in the gastric antrum and duodenal bulb, along with thickened duodenal folds
in the gastric antrum and duodenal bulb, along with thickened duodenal folds  , classic features of duodenitis and gastritis.
, classic features of duodenitis and gastritis.
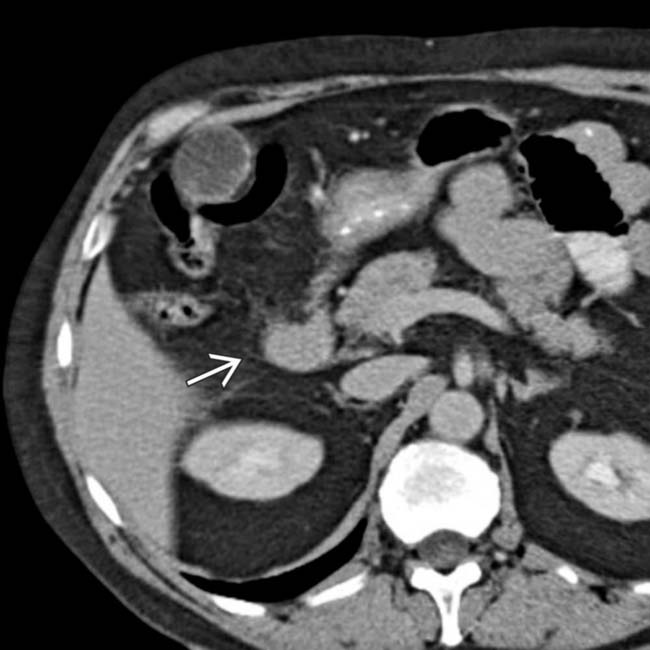
 and lack of distensibility in the gastric antrum due to gastritis.
and lack of distensibility in the gastric antrum due to gastritis.
 , due to duodenitis.
, due to duodenitis.
 due to duodenitis.
due to duodenitis.































 .
.
 .
.
