Chapter 14 Drug eruptions
1. A patient presents to your office with a 10-page typed out medical history. She states that she is “allergic” to twenty different medicines. Is she likely to have drug allergies or drug intolerances to most of these drugs?
Drug intolerance. Drug intolerances account for 90% of adverse drug reactions. An adverse reaction to a drug is an undesirable and usually unanticipated response independent of the intended therapeutic purpose of the medication. An adverse drug reaction may be either immunologic (i.e., drug allergy) or nonimmunologic (i.e., drug intolerance).
2. Name some nonimmunologic drug reactions.
• Nonimmunologic activation of effector pathways, such as direct release of histamine from mast cells and basophils by aspirin, nonsteroidal antiinflammatory drugs (NSAIDs), opiates, polymyxin B, d-tubocurarine, and radiocontrast media
• Cumulative toxicity, such as the accumulation of drugs or metabolites in the skin (e.g., argyria with the use of silver nitrate spray)
• Normal pharmacologic effects of the drug that are not the primary therapeutic objective (e.g., alopecia following chemotherapy)
• Drug interactions (e.g., administration of ketoconazole may lead to higher levels of cyclosporine and increased toxicity)
• Metabolic changes, such as warfarin producing a hypercoagulable state that results in warfarin necrosis
• Exacerbation of preexisting dermatologic diseases (e.g., lithium can exacerbate acne, psoriasis, and subcorneal pustular dermatosis)
• Ecologic changes, such as antibiotics that reduce the bacteriologic flora, predisposing the patient to candidal infections
• Inherited enzyme or protein deficiencies (e.g., the phenytoin hypersensitivity syndrome occurs in patients deficient in epoxide hydrolase, an enzyme required for metabolism of a toxic epoxide derived from phenytoin)
3. What is the most common manifestation of an adverse drug reaction?
Cutaneous reactions are the most common adverse drug reaction and produce a wide range of manifestations: pruritus, maculopapular eruptions, urticaria, angioedema, phototoxic and photoallergic reactions, fixed drug reactions, erythema multiforme, vesiculobullous reactions, and exfoliative dermatitis. Drug-attributed skin reactions are seen in 2% to 5% of inpatients and >1% of outpatients.
4. How does a cutaneous drug eruption typically present?
• Stevens-Johnson syndrome: 4%
Key Points: Drug Eruptions
1. Consider a fixed drug eruption in a patient who presents with bullous or hyperpigmented lesions that are recurrent at the same site.
2. Consider a drug reaction in any patient who presents with an abrupt-onset, symmetrical, cutaneous reaction.
5. How should a suspected drug reaction be evaluated?
7. Can preexisting diseases enhance the chance of getting a maculopapular skin eruption when using amoxicillin or ampicillin?
Amoxicillin or ampicillin produces a maculopapular eruption in about 5% of patients taking these drugs (Fig. 14-1). In patients with infectious mononucleosis, the risk of developing a maculopapular eruption increases to 69% to 100%. In chronic lymphocytic leukemia, the incidence is 60% to 70%. Some studies report that maculopapular eruptions are more common in patients who are also taking allopurinol, but this is not accepted by all authorities. The pathogenesis for this phenomenon is unknown.
8. What infectious disease increases the chance of a cutaneous adverse reaction to trimethoprim-sulfamethoxazole?
9. Which feared drug eruption results in sloughing of the entire skin surface and mucous membranes?
Toxic epidermal necrolysis (TEN) is one of the most severe cutaneous drug eruptions. The skin is initially erythematous and tender but quickly sloughs off in large sheets like “wet wallpaper” (Fig. 14-2). The condition can progress very rapidly, with one of seven patients losing their entire epidermis in 24 hours. Without an epidermis, the body has difficulty keeping fluids in and bacteria out. Despite aggressive supportive care, the mortality rate ranges from 11% to 35%, with the majority of deaths being attributed to sepsis.
Table 14-1. Drugs Most Likely to Produce a Cutaneous Reaction
| DRUG | REACTIONS PER 1000 PATIENTS |
|---|---|
| Amoxicillin | 51.4 |
| Trimethoprim-sulfamethoxazole | 47 |
| Ampicillin | 42 |
| Ipodate sodium | 27.8 |
| Whole blood | 28 |
| Cephalosporins | 13 |


10. Why do some patients get toxic epidermal necrolysis?
The etiology is not completely understood, but recent evidence has found a genetic predisposition in at least some classes of drugs (e.g., association of aromatic antiepileptic drugs and HLA-B*1502 in the Han Chinese). It is likely that continued research will uncover more ties to a genetic predisposition. The molecular and immunologic events are still not fully elucidated; however, the recent demonstration of very high levels of soluble FasL interacting with Fas, which is expressed on the keratinocytes in toxic epidermal necrolysis, may provide insight into the pathophysiology of this life-threatening disorder. In one series, 77% of cases were clearly established as drug-induced. Since the average patient with TEN is on 4.4 drugs, identifying the offending drug can be problematic. Frequent offenders include allopurinol, ampicillin, amoxicillin, carbamazepine, NSAIDs, phenobarbital, phenytoin, sulfonamides, and carbamazepine.
11. What is the difference between erythema multiforme major, Stevens-Johnson syndrome, and toxic epidermal necrolysis?
This is a critical and important question that is difficult to answer because this nosological nightmare continues to be controversial. The short version of these distinctions is as follows:
• Erythema multiforme major is best defined as presentation with targetoid skin lesions that are typical of erythema multiforme, with a more severe variant that is more likely to demonstrate oral lesions, fever, and systemic symptoms. While this variant can be drug-induced, it is more commonly induced by infections such as herpes simplex and Mycoplasma. Some dermatologists consider this to be in the spectrum of Stevens-Johnson syndrome. Microscopically, the keratinocytes are being damaged by lymphocytes (satellite cell necrosis).
• Stevens-Johnson syndrome is most commonly defined as presentation with widespread targetoid lesions that are a flat and atypical when compared to the more defined lesions of erythema multiforme. Lesions are also more frequently purpuric. As in the case of erythema multiforme major, the patients may have fever and systemic symptoms. In contrast to erythema multiforme major, the lesions are more likely to become confluent and develop large areas of blisters and detachment of the epidermis. While some cases are idiopathic or induced by infections, the majority are drug induced. Histologically, the findings are identical to erythema multiforme in that the keratinocytes demonstrates satellite cell necrosis. Some dermatologists arbitrarily define this condition as affecting less than 30% of the body surface, and some authorities even recognize a Stevens-Johnson syndrome/toxic epidermal necrosis overlap syndrome.
• Toxic epidermal necrosis is best defined as a blistering disorder with extensive detachment of the skin that is almost always drug induced, although there are exceptions. Many of the drugs that produce classic Stevens-Johnson syndrome also produced toxic epidermal necrolysis. Targetoid lesions are not usually present but if present are atypical. Microscopically, biopsies are cell poor and cells usually appear to become necrotic without evidence of satellite cell necrosis, suggesting a soluble factor. Some dermatologists arbitrarily differentiate this from Stevens-Johnson syndrome if more than 30% of the cutaneous surface is involved, although many dermatologists feel that toxic epidermal necrolysis and Stevens-Johnson syndrome represent a spectrum of disease.
13. Which type of drug reaction can result in a quick death?
Systemic anaphylaxis, which is IgE mediated, may present with variable findings, including mild pruritus, erythema, urticaria, asthma, circulatory collapse, laryngeal edema, and death. When a patient gives a history of reaction to a drug, the health care provider must ask for details about the previous reaction, particularly seeking a history of urticaria, breathing problems, collapse, and hospitalization.
14. What class of drugs is the most common cause of anaphylaxis?
Beta-lactam antibiotics. Anaphylactic reactions occur in 1 to 5 per 10,000 administrations of penicillin. Most allergic reactions to beta-lactam antibiotics produce urticaria and angioedema, but 10% may result in life-threatening hypotension, bronchospasm, or laryngeal edema. Approximately 1% of all anaphylactic reactions are fatal. Fatal reactions may occur within minutes of parenteral administration of these drugs.
15. Name the drugs most likely to induce urticaria.
Angiotensin-converting enzyme (ACE) inhibitors, gamma-globulin, NSAIDs, penicillins, and sulfonamides. Urticaria produced by drugs is clinically indistinguishable from urticaria produced by other allergens. Aspirin can exacerbate a preexisting urticaria. If possible, aspirin should be discontinued and not utilized in patients with active urticaria.

Figure 14-3. Classic lesions of erythema multiforme secondary to co-trimoxazole, demonstrating targetoid appearance.
(Courtesy of James E. Fitzpatrick, MD.)
Mathelier-Fusade P: Drug-induced urticarias, Clin Rev Allergy Immunol 30:19–23, 2006.
16. How is drug-induced urticaria mediated?
Urticaria may be produced by both nonimmunologic and immunologic mechanisms. Drugs such as codeine, morphine, amphetamine, hydralazine, quinine, vancomycin, and x-ray contrast media produce urticaria by the nonimmunologic release of histamine by mast cells. Allergic urticaria may be due to a type I (Coombs and Gell) reaction mediated by IgE, causing the release of histamine. This usually develops within minutes to hours (usually within 1 hour) after giving the offending drug, and may precede or be associated with anaphylaxis. Urticaria may also be produced by a type III reaction mediated by antigen-antibody complexes. In contrast to type I reactions, which occur within hours, type III urticaria usually develops 1 to 3 weeks after beginning the drug. The clinical appearance of urticaria is often mistaken for erythema multiforme.
17. A 45-year-old white man comes to the emergency room with large areas of nonpitting edema over the face, eyelids, neck, tongue, and mucous membranes, which developed 6 hours ago. Ten days earlier, he started a new drug for hypertension. What is the most likely cause of his reaction?
The clinical description is that of a patient who has angioedema. An ACE inhibitor, such as captopril, enalapril, or lisinopril, is the most likely antihypertensive drug to produce this reaction. A recent study reported that 35% of 17 patients seen for angioedema during a 5-year period were on ACE inhibitors. In another study, 77% of patients experienced the reaction within 3 weeks of starting treatment.
18. A patient is evaluated for a several-day history of fever, malaise, urticaria, arthralgias, lymphadenopathy, and a peculiar erythema along the sides of his palms and soles. He has been started on several new medications in the last few weeks. What is the most likely diagnosis?
The patient most likely has a serum sickness–like drug eruption caused by immune complexes and complement activation. The diagnostic cutaneous finding is the characteristic erythema on the sides of the palms and soles, a finding seen in 75% of cases of serum sickness–like drug eruptions. Other typical findings include fever and malaise (100%), urticaria (90%), arthralgias (50% to 67%), and lymphadenopathy (13%). Glomerulonephritis is common in serum sickness reactions in animals but uncommon in humans. Reactions occur 7 to 21 days after the drug is given but may occur with the first administration of the drug. Commonly implicated drugs include beta-lactam antibiotics, sulfonamides, thiouracil, cholecystographic dyes, and hydantoin.
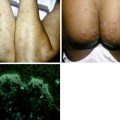
19. A man complains of a recurrent burning eruption on his penis. He develops a single blister over the glans penis that heals over 1 to 2 weeks with hyperpigmentation. This same pattern has happened on three occasions in the last 2 years. What does he have?
The history is characteristic of a fixed drug eruption. Fixed drug eruptions are cutaneous reactions that recur at the same site with each administration of the drug, typically within 6 to 48 hours of initiation of the causative agent. Characteristically, it occurs on the face or genitalia but may occur anywhere (Fig. 14-4). It is a well demarcated erythematous lesion that often blisters and heals with hyperpigmentation. Drugs commonly associated include phenolphthalein in laxatives, sulfonamides, β-lactam antibiotics, tetracycline, barbiturates, gold, oral contraceptives, diazepam, and aspirin. Foods have also been implicated in fixed drug reactions.

20. How does drug-induced lupus erythematosus (LE) differ from idiopathic systemic lupus erythematosus (SLE)?
Drug-induced LE is generally milder than idiopathic SLE. Drug-induced LE usually manifests as fever, malaise, pleuritis, pneumonitis, and arthralgias. Skin, mucous membrane, central nervous system findings, and renal disease are more commonly seen in idiopathic SLE. The antinuclear antibodies in drug-induced LE are usually antihistone and single-stranded DNA antibodies, whereas idiopathic SLE is associated with double-stranded DNA and Sm antibodies. Drug-induced LE usually resolves simply by stopping the drug. Drug-induced LE constitutes 5% to 10% of all cases of SLE. Less commonly patients may have drug-induced subacute cutaneous lupus erythematosus with anti-Ro/SSA antibodies or classic systemic lupus with drug-induced double-stranded DNA antibodies.
21. What drugs are usually associated with drug-induced LE?
Of patients treated continuously with procainamide, 90% develop antinuclear antibodies after 2 years, and 10% to 20% develop symptoms of LE. Other commonly implicated drugs include hydralazine, isoniazid, chlorpromazine, procainamide, hydantoin, d-penicillamine, methyldopa, quinidine, and minocycline.
22. Which drug is usually associated with erythema nodosum?
Erythema nodosum, which is a form of panniculitis that characteristically presents as tender erythematous nodules over the shins, is most commonly associated with oral contraceptives. Sulfonamides, bromides, iodides, tetracycline, penicillin, and 13-cis retinoic acid have also been associated with erythema nodosum.
23. What drugs are associated with lichenoid drug eruptions?
Lichenoid drug eruptions clinically and histologically resemble lichen planus. The lesions are usually multiple, purple, discrete, flat-topped polygonal papules and plaques. As in the case of lichen planus, this reaction may also affect or even be limited to the oral mucosa. This differs from other drug reactions in that it may take weeks to years following administration of the drug to develop the lesions. Sulfonamides (especially thiazide diuretics), gold, captopril, propranolol, and antimalarials are the most common drugs that produce these reactions. It may take months for the rash to resolve following discontinuation of the drug.
25. What drugs can produce subepidermal bullae and erosions on the dorsum of the hands?
The description is characteristic of the eruption seen in porphyria cutanea tarda and, less commonly, in variegate porphyria and hereditary coproporphyria. This reaction is called pseudoporphyria since the porphyrin levels are normal (Fig. 14-6). Tetracycline, nalidixic acid, oral contraceptives, cyclosporine, furosemide and other sulfonamides, dapsone, NSAIDs, 5-fluorouracil, isotretinoin, and pyridoxine are most likely to induce pseudoporphyria.
Table 14-2. Drugs Producing Changes in Skin Pigmentation
| COLOR | DRUG |
|---|---|
| Slate-gray | Chloroquine Hydroxychloroquine (see Fig. 14-5A) Minocycline (see Fig. 14-5B) Phenothiazines |
| Slate-blue | Amiodarone |
| Blue-gray | Gold (chrysoderma) |
| Yellow | Beta-carotene Quinacrine |
| Red | Clofazimine |
| Brown (hyperpigmentation) | Adrenocorticotropic hormone (ACTH) Bleomycin Oral contraceptives Zidovudine |

27. A 30-year-old white woman is evaluated with a new case of “acne.” Over the last few days, she has suddenly developed erythematous follicular papules and pustules over her upper trunk. She was admitted 3 weeks earlier with an acute exacerbation of SLE that is now improving. What is the most likely diagnosis?
Steroid acne is the most likely diagnosis. Her history indicates a high probability that she was started on corticosteroids during the admission. Steroid acne typically presents with inflammatory papules and pustules, but comedones and cysts are typically absent. In contrast to acne vulgaris, steroid acne preferentially involves the trunk and demonstrates lesions in the same stage of development. Other drugs associated with similar eruptions include lithium, isoniazid, bromides, and iodides. Many chemotherapeutic agents have also been associated with acneiform reactions. These include cetuximab, dactinomycin, erlotinib, fluoxymesterone, gefitinib, medroxyprogesterone, and vinblastine.
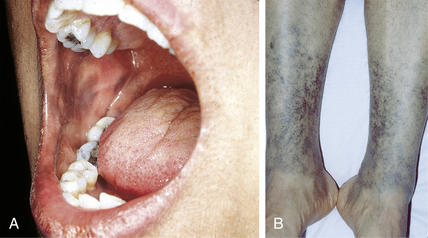
28. A middle-aged man who is a dialysis patient presents to your clinic with a “woody” appearance to his legs. He had an MRI with gadolinum-containing contrast a few months prior. What might he be suffering from?
Nephrogenic systemic fibrosis (formerly called nephrogenic fibrosing dermopathy). Nephrogenic systemic fibrosis is an uncommon disease with cutaneous manifestations that include induration, thickening, and hardening of the skin, most commonly on the extremities. The pathophysiology is related to the exposure of patients with renal insufficiency to gadolinium-based contrast agents.
High HA, Ayers RA, Cowper SE: Gadolinium is quantifiable within the tissue of patients with nephrogenic systemic fibrosis, J Am Acad Dermatol 56:710–712, 2007.
29. Describe a typical presentation of warfarin necrosis.
The patient is typically a woman who has been given a loading dose of warfarin (Coumadin). Between 3 and 5 days after starting the drug, the patient develops one or more lesions over the thighs, buttocks, or breasts. Initially painful and red, the lesions rapidly become necrotic with hemorrhagic bullae and an erythematous edge (Fig. 14-7). A necrotic eschar rapidly develops.

30. Name and describe the two types of photoinduced drug eruptions.
Phototoxic drug reactions and photoallergic drug reactions. Phototoxic reactions occur within minutes to hours after exposure to both the drug and light and occur in all individuals given the specific drug and ultraviolet (UV) exposure. The rash clinically resembles a sunburn and stinging is a prominent feature. Photoallergic drug reactions are mediated by type IV delayed hypersensitivity and occur 24 to 48 hours after UV exposure. Clinically, the lesions are on sun-exposed sites, but are not as well demarcated as phototoxic reactions. They are also eczematous and pruritic.
33. What is AGEP? How does it present?
AGEP is an acronym for acute generalized exanthematous pustulosis. Patients present with an abrupt onset of a generalized, scarlatiniform, erythematous exanthem associated with numerous small, sterile, nonfollicular pustules (Fig. 14-9). There may be associated fever, prostration, and leukocytosis. In one study, 17% of patients had a personal history of psoriasis. The lesions typically occur within a few days of initiating the offending drug. Beta-lactam antibiotics are the most common culprits followed by macrolides and mercury. The reaction is typically short lived. Resolution usually occurs within 1 to 2 weeks of discontinuing the offending agent and is accompanied by widespread skin desquamation.

Figure 14-8. Demeclocycline-induced phototoxic reaction on the dorsum of the hands.
(Courtesy of James E. Fitzpatrick, MD.)