Chapter 4 Disorders of Sex Development
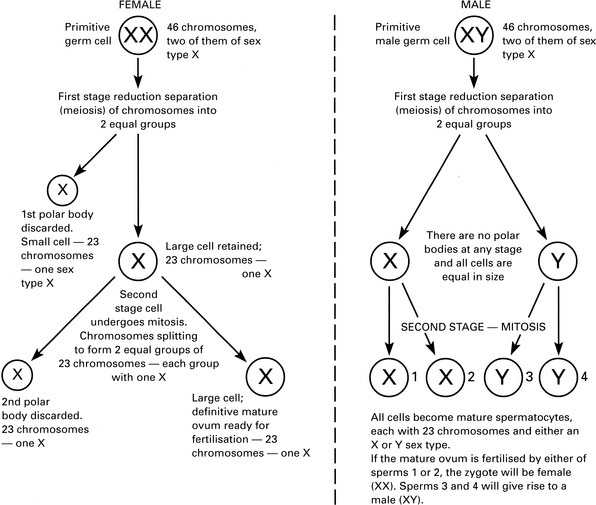
Genetic abnormalities
Congenital abnormalities
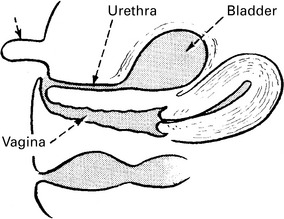
Complete androgen insensitivity (cais)
This condition was previously known as testicular feminisation and may be mistaken for a sex chromosome abnormality. The chromosomal pattern is 46XY; however, there is insensitivity of the androgen receptor to respond to androgenic stimulation. As a Y chromosome is present, the testes form normally, producing anti-Müllerian hormone (AMH) and testosterone. AMH causes the regression of the Müllerian ducts (see Chapter 1), and the uterus, fallopian tubes and upper part of vagina therefore do not form. As the tissues are insensitive to androgens, the lower genital tract fails to virilise and a short vagina is formed. The patient is phenotypically female. Usually the diagnosis is made in early adult life when the patient complains of amenorrhoea.
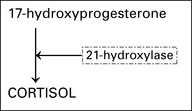
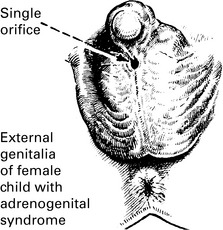
Congenital adrenal hyperplasia (cah)
Abnormalities of ovary and tube
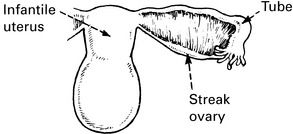
Abnormalities of the uterus
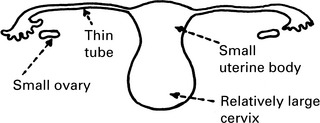
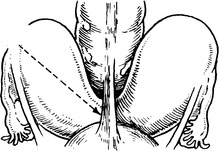
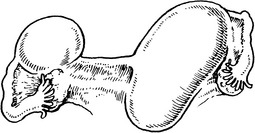
Absent or rudimentary uterus
This can be associated with atresia of the vagina (Mayer–Rokitansky syndrome).
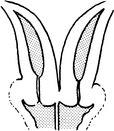
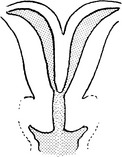
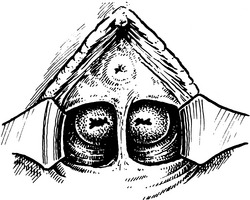
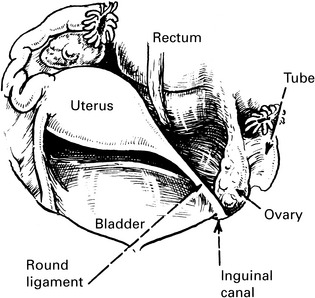
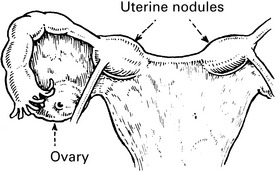
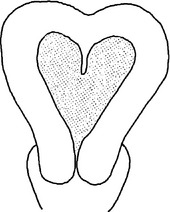
Bicornuate uterus or uterus bicornis
Note the ligament, which may pass from rectum to bladder. There is a cleft present at the fundus.


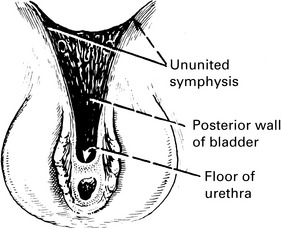
Abnormalities of the vagina