[level-membership-for-pediatrics-category]
Chapter 438 Diseases of the Blood Vessels (Aneurysms and Fistulas)
438.1 Kawasaki Disease
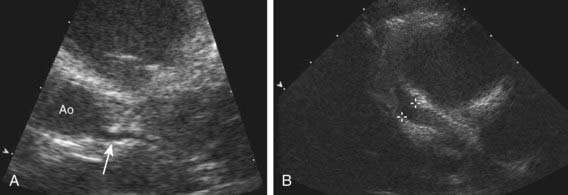
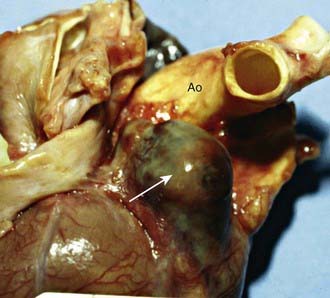
Aneurysms of the coronary or systemic arteries may complicate Kawasaki disease and are the leading cause of morbidity in this disease (Figs. 438-1 and 438-2 on the Nelson Textbook of Pediatrics website at www.expertconsult.com  ). Other than in Kawasaki disease, aneurysms are not common in children and occur most frequently in the aorta in association with coarctation of the aorta, patent ductus arteriosus, and Marfan syndrome and in intracranial vessels (Chapter 594). They may also occur secondary to an infected embolus; infection contiguous to a blood vessel; trauma; congenital abnormalities of vessel structure, especially the medial wall; and arteritis, for example, polyarteritis nodosa, Behçet syndrome, and Takayasu arteritis (Chapter 161.2).
). Other than in Kawasaki disease, aneurysms are not common in children and occur most frequently in the aorta in association with coarctation of the aorta, patent ductus arteriosus, and Marfan syndrome and in intracranial vessels (Chapter 594). They may also occur secondary to an infected embolus; infection contiguous to a blood vessel; trauma; congenital abnormalities of vessel structure, especially the medial wall; and arteritis, for example, polyarteritis nodosa, Behçet syndrome, and Takayasu arteritis (Chapter 161.2).
438.2 Arteriovenous Fistulas
Arteriovenous fistulas may be limited to small cavernous hemangiomas or may be extensive (Chapters 499 and 642). The most common sites in infants and children are within the cranium, in the liver, in the lung, in the extremities, and in vessels in or near the thoracic wall. These fistulas, though usually congenital, may follow trauma or be a manifestation of hereditary hemorrhagic telangiectasia (Osler-Weber-Rendu disease). Femoral arteriovenous fistulas are a rare complication of percutaneous femoral catheterization.
Clinical Manifestations
Large intracranial arteriovenous fistulas most often occur in newborn infants in association with a vein of Galen malformation. The large intracranial left-to-right shunt results in heart failure secondary to the demand for high cardiac output. Patients with smaller communications may not have cardiovascular manifestations but may later be disposed to hydrocephalus (Chapter 585.11) or seizure disorders. The diagnosis can often be made by auscultation of a continuous murmur over the cranium. Older children with more diffuse intracranial arteriovenous malformations may be recognized on the basis of intracranial calcification and high cardiac output without cardiac failure.
Abernethy LJ. Classification and imaging of vascular malformations in children. Eur Radiol. 2003;13:2483-2497.
Faughnan ME, Thabet A, Mei-Zahav M, et al. Pulmonary arteriovenous malformations in children: outcomes of transcatheter embolotherapy. J Pediatr. 2004;145:826-831.
Fong LV, Lee SH, Salmon AP. Diagnosis of cerebral arteriovenous malformations by colour Doppler examination. Eur Heart J. 1992;13:415-417.
Friedman DM, Verma R, Madrid M, et al. Recent improvement in outcome using transcatheter embolization techniques for neonatal aneurysmal malformations of the vein of Galen. Pediatrics. 1993;91:583-586.
[/level-membership-for-pediatrics-category][not-level-membership-for-pediatrics-category]
Chapter 438 Diseases of the Blood Vessels (Aneurysms and Fistulas)
438.1 Kawasaki Disease
Aneurysms of the coronary or systemic arteries may complicate Kawasaki disease and are the leading cause of morbidity in this disease (Figs. 438-1 and 438-2 on the Nelson Textbook of Pediatrics website at www.expertconsult.com ). Other than in Kawasaki disease, aneurysms are not common in children and occur most frequently in the aorta in association with coarctation of the aorta, patent ductus arteriosus, and Marfan syndrome and in intracranial vessels (Chapter 594). They may also occur secondary to an infected embolus; infection contiguous to a blood vessel; trauma; congenital abnormalities of vessel structure, especially the medial wall; and arteritis, for example, polyarteritis nodosa, Behçet syndrome, and Takayasu arteritis (Chapter 161.2).
