Bowel Diseases
Synonyms/Description
Etiology
Ultrasound Findings
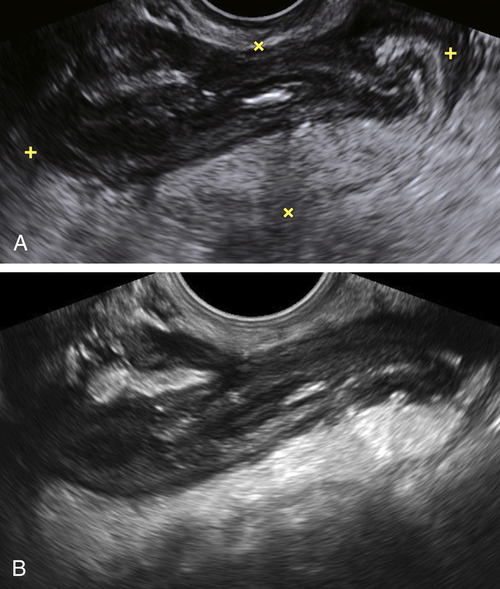
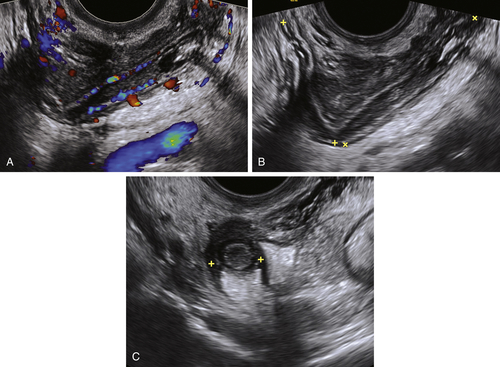
Endometriosis
Appendicitis
Inflammatory Bowel Diseases
Diverticulitis
Duplication Cyst
Lymphoma
Colon Cancer
Gastrointestinal Stromal Tumor
Differential Diagnosis
Clinical Aspects and Recommendations
Figures


Videos
Suggested Reading
Ackerman S.J., Irshad A., Anis M. Ultrasound for pelvic pain. II: Nongynecologic causes. Obstet Gynecol Clin North Am.. 2011;38:69–83.
Gustafsson B.I., Siddique L., Chan A., Dong M., Drozdov I., Kidd M., Modlin I.M. Uncommon cancers of the small intestine, appendix and colon: an analysis of SEER 1973-2004, and current diagnosis and therapy. Int J Oncol.. 2008;33:1121–1131.
Hughes J.A., Cook J.V., Said A., Chong S.K., Towu E., Reidy J. Gastrointestinal stromal tumour of the duodenum in a 7-year-old boy. Pediatr Radiol. 2004;34:1024–1027.
Lee N.K., Kim S., Kim G.H., Jeon T.Y., Kim D.H., Jang H.J., Park D.Y. Hypervascular subepithelial gastrointestinal masses: CT-pathologic correlation. RadioGraphics. 2010;30:1915–1934.
Linam L.E., Munden M. Sonography as the first line of evaluation in children with suspected acute appendicitis. J Ultrasound Med. 2012;31:1153–1157.
Maturen K.E., Wasnik A.P., Kamaya A., Dillman J.R., Kaza R.K., Pandya A., Maheshwary R.K. Ultrasound imaging of bowel pathology: technique and keys to diagnosis in the acute abdomen. AJR. 2011;197:1067–1075.
O’Malley M.E., Wilson S.R. Ultrasound of gastrointestinal tract abnormalities with CT correlation. RadioGraphics. 2003;23:59–72.






