Differential diagnosis of lesions of variable radiopacity in the jaws
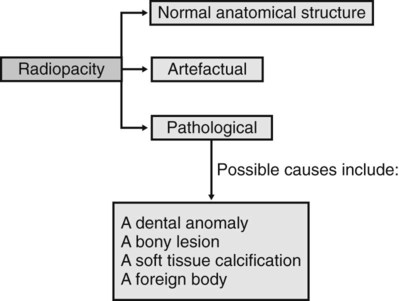
As explained in Chapter 25, a variety of conditions that can affect the jaws are radiopaque relative to the surrounding bone, although the degree of opacity can be very variable. A step-by-step guide, similar to that suggested for radiolucent lesions in Chapter 26, is outlined to emphasize the importance of a methodical approach when producing a differential diagnosis. The suggested approach is summarized in Fig. 27.1. Although most lesions are still detected using plain radiographs, this process can be greatly facilitated in many cases if advanced imaging modalities, described in Chapters 16 and 18, such as computed tomography (CT), cone beam CT or magnetic resonance (MR) are available.
Step I
Describe the variable radiopacity noting in particular:
• Site or anatomical position – is the opacity actually within bone or is it within the surrounding soft tissues and thus superimposed on the bone? To localize the opacity, two radiographs are usually required, ideally at right angles to one another.
• Outline or periphery – a particularly useful differentiating feature, since if the opacity is surrounded by a thin radiolucent line, it is invariably of dental tissue origin.
Step II
Decide whether the variable radiopacity is:
1. A normal anatomical feature
– An area of dense bone sometimes referred to as a dense bone island
– A bony prominence such as the external oblique ridge, mylohyoid line or genial tubercles
These depend largely on the type of radiograph, but examples include:
Step IV
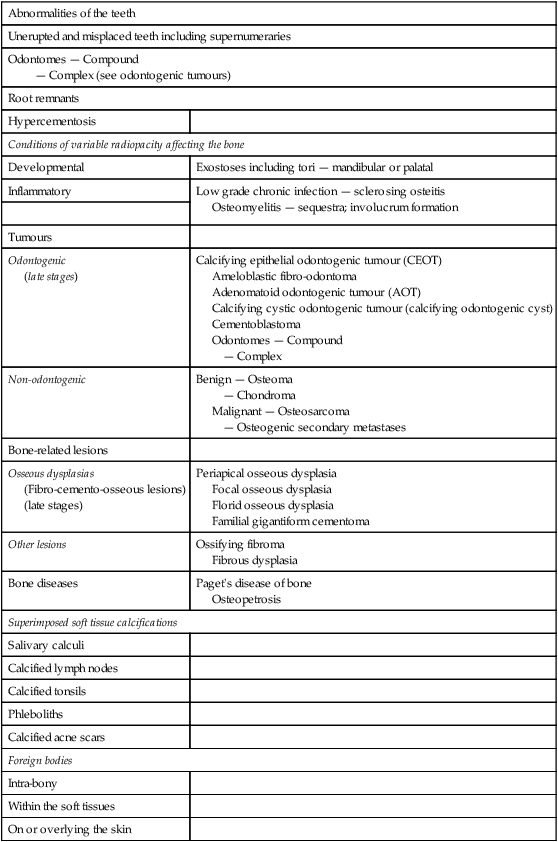
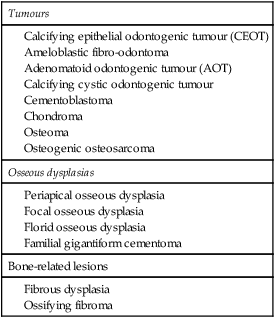
Consider the subdivisions of these pathological categories. A typical list is shown in Table 27.1.
Table 27.1
Classification of the more common lesions that can present as variable radiopacities in the jaws
| Abnormalities of the teeth | |
| Unerupted and misplaced teeth including supernumeraries | |
| Odontomes — Compound — Complex (see odontogenic tumours) |
|
| Root remnants | |
| Hypercementosis | |
| Conditions of variable radiopacity affecting the bone | |
| Developmental | Exostoses including tori — mandibular or palatal |
| Inflammatory | Low grade chronic infection — sclerosing osteitis Osteomyelitis — sequestra; involucrum formation |
| Tumours | |
| Odontogenic (late stages) |
Calcifying epithelial odontogenic tumour (CEOT) Ameloblastic fibro-odontoma Adenomatoid odontogenic tumour (AOT) Calcifying cystic odontogenic tumour (calcifying odontogenic cyst) Cementoblastoma Odontomes — Compound — Complex |
| Non-odontogenic | Benign — Osteoma — Chondroma Malignant — Osteosarcoma — Osteogenic secondary metastases |
| Bone-related lesions | |
| Osseous dysplasias (Fibro-cemento-osseous lesions) (late stages) |
Periapical osseous dysplasia Focal osseous dysplasia Florid osseous dysplasia Familial gigantiform cementoma |
| Other lesions | Ossifying fibroma Fibrous dysplasia |
| Bone diseases | Paget’s disease of bone Osteopetrosis |
| Superimposed soft tissue calcifications | |
| Salivary calculi | |
| Calcified lymph nodes | |
| Calcified tonsils | |
| Phleboliths | |
| Calcified acne scars | |
| Foreign bodies | |
| Intra-bony | |
| Within the soft tissues | |
| On or overlying the skin | |
Step V
Compare the radiological features of the unknown opacity with the typical radiological features of these possible conditions. Then construct a list showing, in order of likelihood, all the conditions that the lesion might be. As mentioned in Chapter 26, this list forms the radiological differential diagnosis.
The typical radiographic features of the important radiopacities are described below using a similar style to that adopted in Chapter 26. It must be emphasized that this is a simplified approach and that most lesions can produce a variety of appearances.
Typical radiographic features of abnormalities of the teeth
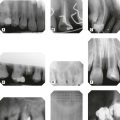
Unerupted or misplaced teeth including supernumeraries (Fig. 27.2)
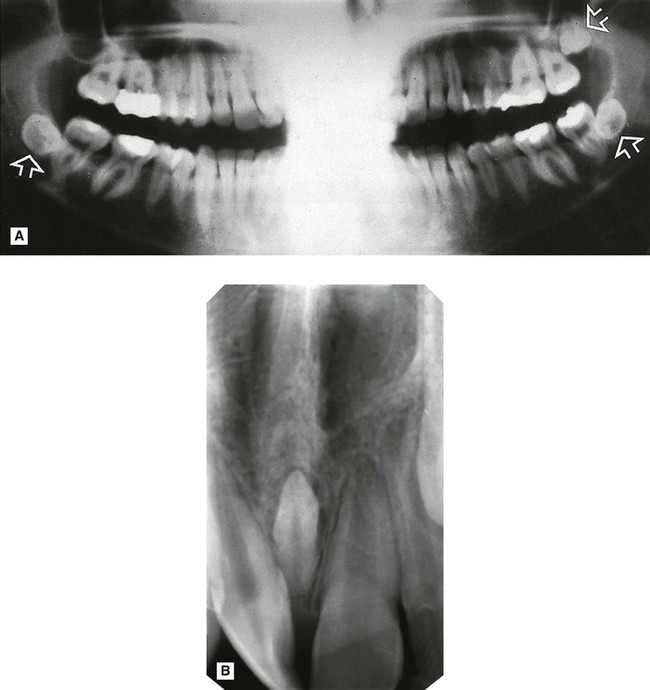
 are positioned transversely. B Periapical showing a conically shaped mesiodens (arrowed) between
are positioned transversely. B Periapical showing a conically shaped mesiodens (arrowed) between  . Density, shape and outline confirm that the opacity is composed of dental tissue.
. Density, shape and outline confirm that the opacity is composed of dental tissue.
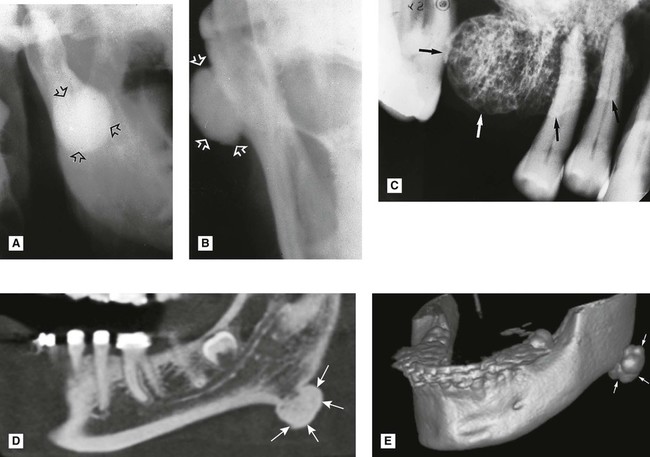
Odontomes
Although both compound and complex odontomes are more accurately classified as epithelial odontogenic tumours with odontogenic ectomesenchyme showing dental hard tissue formation (WHO Classification 2005), they are often also described as dental developmental anomalies (see Ch. 24).
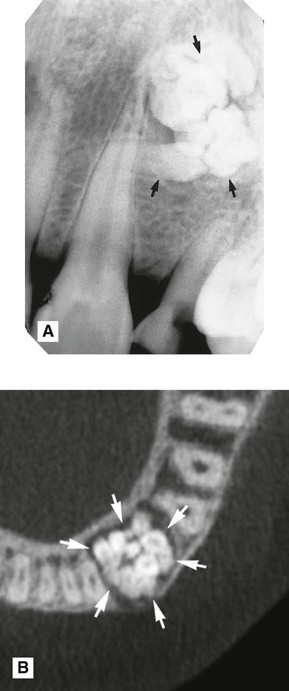
 region showing a radiopaque compound odontome (arrowed), consisting of small denticles. B Axial CBCT scan showing another compound odontome in the
region showing a radiopaque compound odontome (arrowed), consisting of small denticles. B Axial CBCT scan showing another compound odontome in the  region (arrowed).
region (arrowed).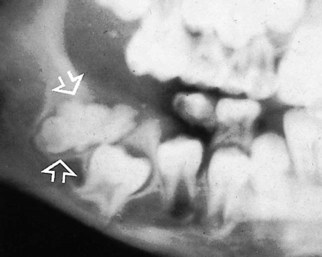
 (arrowed). It is preventing the eruption of
(arrowed). It is preventing the eruption of  . The opacity shows the characteristic surrounding radiolucent line, confirming its dental tissue origin.
. The opacity shows the characteristic surrounding radiolucent line, confirming its dental tissue origin.
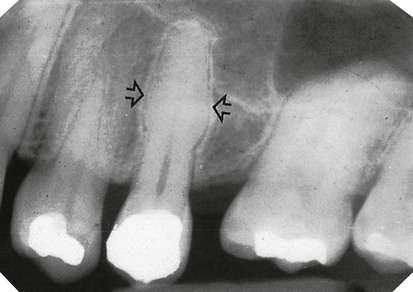
 root caused by the root remnants of the deciduous
root caused by the root remnants of the deciduous  .
.
 (arrowed).
(arrowed).Typical radiographic features of conditions of variable opacity affecting bone
Developmental
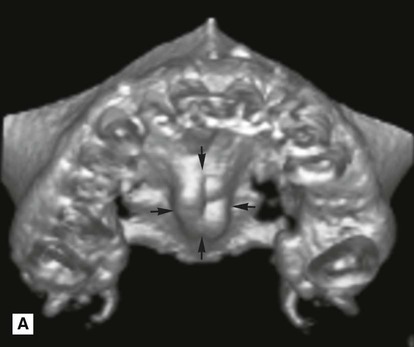
Exostoses, including tori (mandibular or palatal)
Exostoses are small, irregular overgrowths of bone sometimes developing on the surface of the alveolar bone. They consist primarily of compact bone and produce an ill-defined radiopacity when superimposed over the bulk of the alveolar bone. Usually two views are required to establish the exact site (see Fig. 27.7).
 />
/> />
/>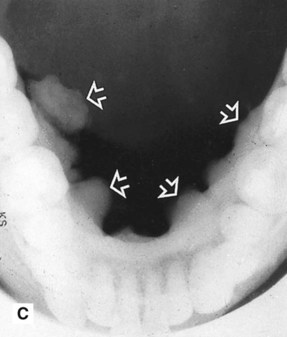
 showing ill-defined areas of radiopacity (arrowed) overlying the teeth. C Lower 90° occlusal of the same patient showing the large irregular exostoses (mandibular tori) on the lingual aspect of the mandible (arrowed).
showing ill-defined areas of radiopacity (arrowed) overlying the teeth. C Lower 90° occlusal of the same patient showing the large irregular exostoses (mandibular tori) on the lingual aspect of the mandible (arrowed).Specific exostoses develop in particular sites and are often bilateral:
• Torus mandibularis – lingual aspects of the mandible, in the premolar/molar region
• Torus palatinus – either side of the midline towards the posterior part of the hard palate.
Tumours
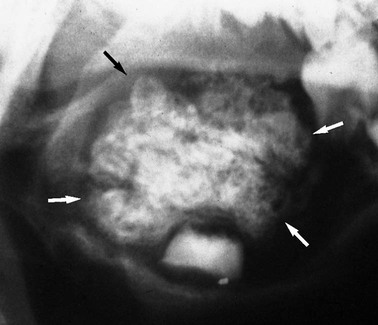
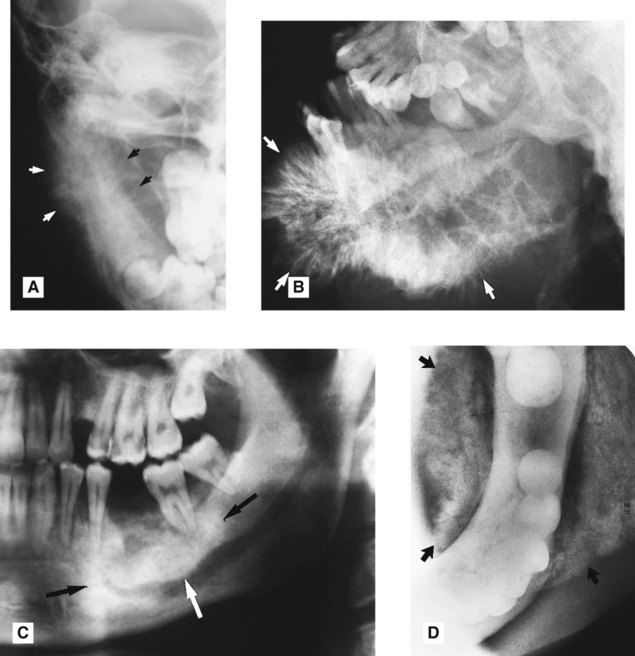
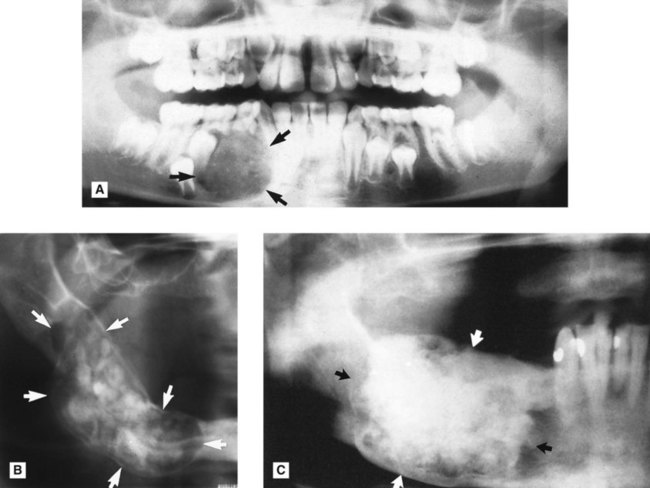
Calcifying epithelial odontogenic tumour (CEOT or Pindborg tumour) (Fig. 27.8)
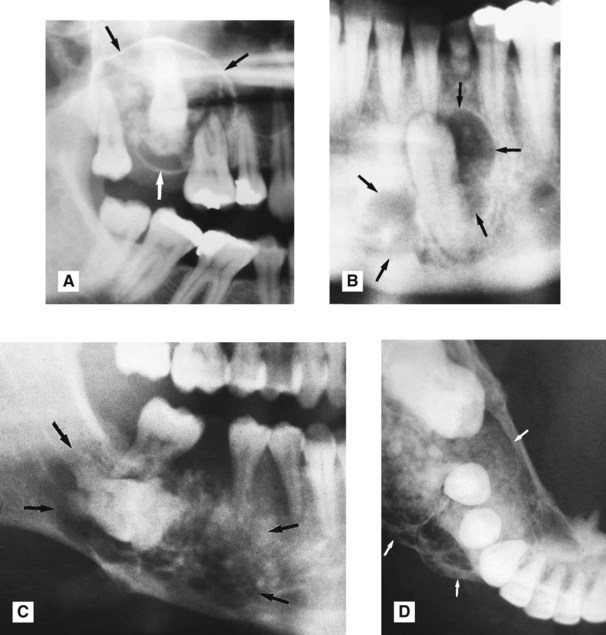
 . There are obvious areas of calcification within the lesion. B Part of a panoramic radiograph showing another CEOT (arrowed) associated with the unerupted lower left canine, with only faint internal calcification. C Right side of a panoramic radiograph showing a poorly defined calcifying epithelial odontogenic tumour (arrowed) associated with the unerupted molar. D Lower 90° occlusal of the same patient showing the expansive, multilocular nature of the lesion and the discrete internal calcifications.
. There are obvious areas of calcification within the lesion. B Part of a panoramic radiograph showing another CEOT (arrowed) associated with the unerupted lower left canine, with only faint internal calcification. C Right side of a panoramic radiograph showing a poorly defined calcifying epithelial odontogenic tumour (arrowed) associated with the unerupted molar. D Lower 90° occlusal of the same patient showing the expansive, multilocular nature of the lesion and the discrete internal calcifications.• Frequency: Rare – approximately 1% of all odontogenic tumours.
• Site: —Molar/premolar region of the mandible
• Shape: — Unilocular or multilocular
 .
.• Outline: —Variable definition, frequently scalloped
• Radiodensity: —Radiolucent in early stages then numerous scattered radiopacities usually become evident within the lesion, often most prominent around the crown of any associated unerupted tooth
• Effects: —Adjacent teeth sometimes displaced, sometimes resorbed
Ameloblastic fibro-odontoma (Fig. 27.9)
These rare, unilocular or multilocular odontogenic tumours resemble closely ameloblastic fibromas (see Fig. 26.10), and also affect children. However, they are often associated with an unerupted tooth and usually contain enamel or dentine, either as multiple, small opacities or as a solid mass.
Adenomatoid odontogenic tumour (AOT) (Fig. 27.10)
 . Internal calcification is evident. B Periapical of the anterior maxilla showing another adenomatoid odontogenic tumour (arrowed) with internal calcification, associated with an unerupted canine.
. Internal calcification is evident. B Periapical of the anterior maxilla showing another adenomatoid odontogenic tumour (arrowed) with internal calcification, associated with an unerupted canine. • Age: Variable, but 90% develop before the age of 30 with most diagnosed in the second decade.
• Frequency: Rare – approximately 2–7% of all odontogenic tumours.
• Site: — Anterior maxilla – incisor/canine region
• Outline: — Smooth and well defined
• Radiodensity: —Initially radiolucent, but small opacities (snowflakes) within the central radiolucency may be seen peripherally as the lesion matures.
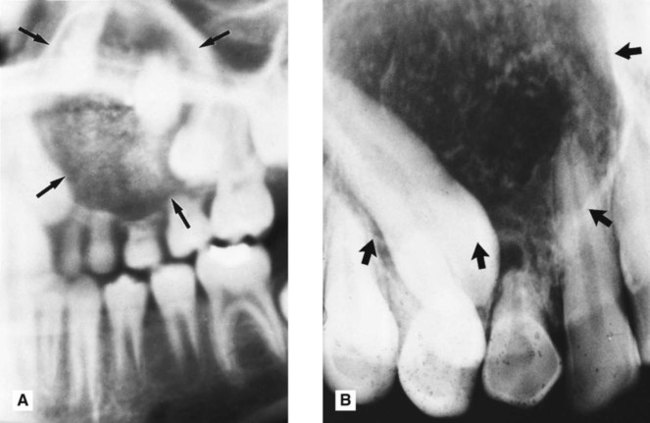
Calcifying cystic odontogenic tumour (calcifying odontogenic cyst or Gorlin’s cyst) (Fig. 27.11)
• Age: Variable, reported in patients between 5 and 92 years old.
• Site: Mandible or maxilla – anterior or premolar regions, one third associated with an unerupted tooth or odontome.
• Size: Usually small, up to 4 cm in diameter.
• Shape: Variable, but usually unilocular.
• Outline: — Smooth, well defined
• Radiodensity: Initially radiolucent but in more advanced stages contains a variable amount of calcified radiopaque material of tooth-like density.
• Effects: —Adjacent teeth usually displaced, causing root divergence, and/or resorbed
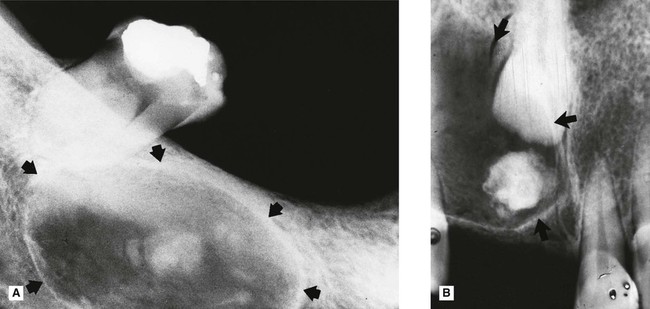
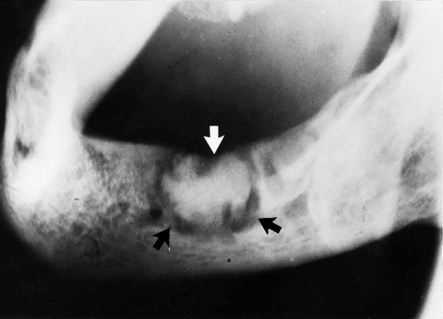
Cementoblastoma (Fig. 27.12)
As indicated in Table 27.1, the cementoblastoma is classified by the WHO as an odontogenic tumour which is characterized by the formation of cementum-like tissue in connection with the root of a tooth.

 of a cementoblastoma, the so-called golf ball appearance. The mass is attached to the root and has a thin radiolucent line around it (arrowed). B Part of a panoramic radiograph showing a radiopaque cementoblastoma at the apex of
of a cementoblastoma, the so-called golf ball appearance. The mass is attached to the root and has a thin radiolucent line around it (arrowed). B Part of a panoramic radiograph showing a radiopaque cementoblastoma at the apex of  (arrowed).
(arrowed).• Age: Reported in patients between 8 and 44 years old, with a mean age of 20.
• Site: Apex of mandibular first permanent molars, occasionally premolars. Exceptionally associated with the primary dentition.
• Size: Variable, but up to 2–3 cm in diameter.
• Shape: —Round or irregular, sometimes described as resembling a golf ball
• Radiodensity: —Radiopaque but often surrounded by a thin radiolucent line owing to an outer zone of osteoid.
• Effects: —Attached to the tooth root which is usually obscured as a result of resorption and fusion to the tooth
Osteosarcoma (Fig. 27.14)
• Osteolytic – no neoplastic bone formation.
• Osteogenic/osteosclerotic – neoplastic osteoid and bone formed.
• Mixed lytic and sclerotic – patches of neoplastic bone formed.
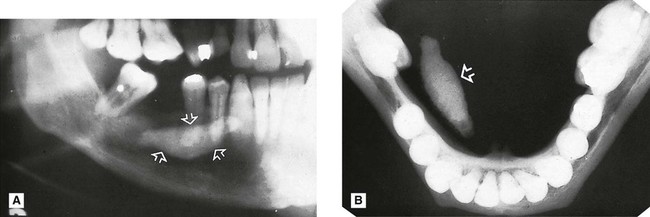
Osseous dysplasias
Periapical osseous dysplasia (Fig. 27.15)

• Age: Middle-aged adults (typically black women).
• Site: Apices of several lower incisor teeth.
• Size: Small, usually only up to 5–6 mm in diameter.
• Outline: Variable but usually poorly defined and not corticated.
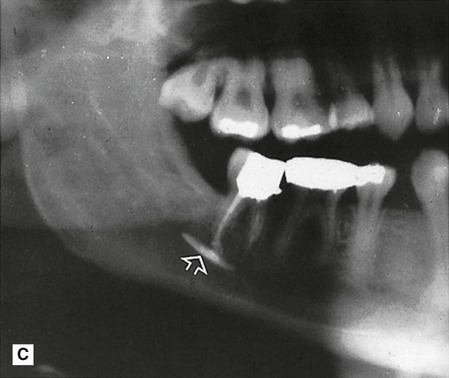
Focal osseous dysplasia (Fig. 27.16)
 extraction site (arrowed). An appreciable amount of internal calcification is evident.
extraction site (arrowed). An appreciable amount of internal calcification is evident.• Age: Adults between 40 and 50 years old (typically white women).
• Site: Any areas of the jaws (dentulous or edentulous), but mainly posterior mandible, and often in extraction sites.
• Size: Small, less than 1.5 cm in diameter.
• Outline: — Well defined but irregular
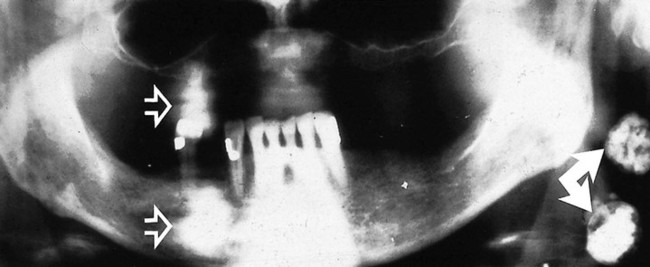
Florid osseous dysplasia (Fig. 27.17)
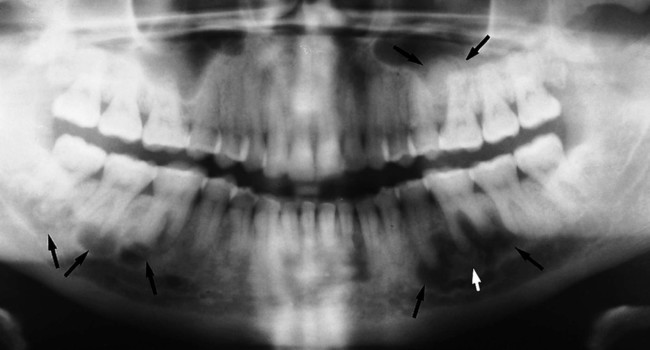
• Age: Middle-aged adults (typically black women).
• Site: Widespread, often in all four quadrants (dentulous and edentulous) but associated with the apices of the teeth if present.
• Size: Variable, but individual lesions up to 2–3 cm in diameter.
• Outline: — Smooth but lobular
Bone-related lesions
As shown in Table 27.1, the WHO classifies a number of different conditions under the general heading bone-related. Two of these can present as mixed radiolucent/radiopaque lesions in the jaws, including:
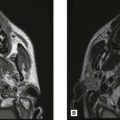
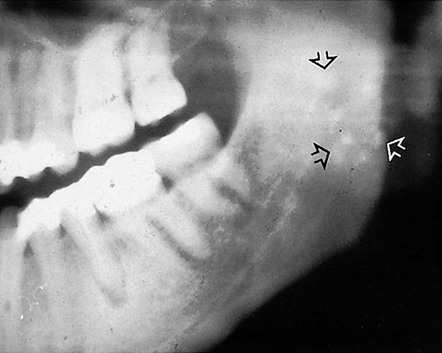
Fibrous dysplasia (Fig. 27.18)
Fibrous dysplasia is described by the WHO as a genetically based sporadic disease of bone affecting single or multiple bones. The jaws and other bones in the skull can be affected as well as other bones in the skeleton. The general radiological features of fibrous dysplasia are covered in Chapter 28.

The radiographic features of jaw lesions include:
• Age: 10–20-year-old adolescents.
• Site: Maxilla – usually posteriorly, more commonly than the mandible. Maxillary lesions may spread to involve adjacent bones such as the zygoma, sphenoid, occiput and base of skull.
• Size: Variable and difficult to define.
• Outline: —Poorly defined, with the margins merging imperceptibly with adjacent normal bone
• Radiodensity: —Initially radiolucent (but rarely seen clinically at this stage)
Ossifying fibroma (Fig. 27.19)
• Age: Variable, but usually in the 2nd–4th decades (particularly women).
• Site: Usually posterior mandible, but different variants can affect the maxilla and paranasal sinuses.
• Size: Variable, may grow to several cm in diameter and cause facial asymmetry.
• Outline: — Smooth, well defined
Summary
It is worth repeating that the radiodensity of many of the lesions mentioned in this chapter changes as they mature. During their early stages of development, there may be no evidence of internal calcification, making radiological differential diagnosis more difficult. For revision purposes, Table 27.2 summarizes the main lesions of variable radiodensity that can develop internal radiopaque calcifications and so present with mixed radiolucent/radiopaque appearances.
Table 27.2
Typical radiographic features of soft tissue calcifications
Radiopaque salivary calculi (see Ch. 32)
Submandibular gland calculi (Fig. 27.20) are often radiopaque and develop within the main duct or in the gland itself. Those in the main duct can be superimposed on the alveolar bone producing an opacity apparently within the bone. Stones in the gland present usually below the lower border of the mandible.

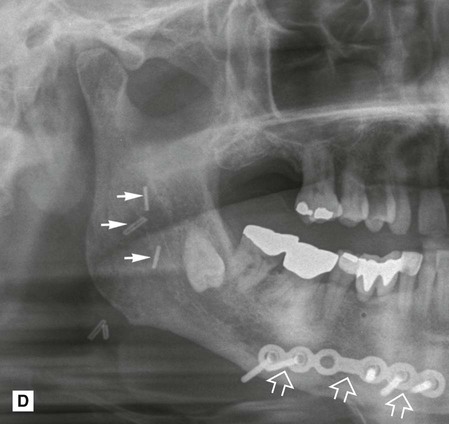
Typical radiographic features of foreign bodies
A variety of foreign bodies can produce radiopacities. The appearance depends obviously on the nature of the foreign body, its density and its location. Figure 27.24 shows a selection of foreign bodies.
 />
/> />
/> />
/>
To access the self assessment questions for this chapter please go to www.whaitesessentialsdentalradiography.com