Chapter 17 Differences in Neuromuscular Characteristics between Male and Female Athletes
INTRODUCTION
Joint stability may be defined as the state of a joint remaining or promptly returning to proper alignment through an equalization of forces.71 This requires a synergy between bones, joint capsules, ligaments, muscles, tendons, and sensory receptors.83 The static components of joint stability include the ligaments, joint capsule, cartilage, friction, and the bony geometry of the articulation.35,48 These components are typically assessed through joint stress testing and have commonly defined clinical joint stability.71 These static components provide the foundation for joint stability during functional activities by guiding joint arthrokinematics. However, during physically demanding tasks such as running, jumping, and cutting, these components may not provide the restraint necessary to prevent joint injury. During these tasks, stability is provided by dynamic components that include the neuromuscular control of the skeletal muscles crossing the joint.71 The functional joint stability accomplished through the integration and complementary relationship between the static and the dynamic components of joint stability is referred to as dynamic joint stability.
Dynamic joint stability is influenced by the neuromuscular control of the muscles crossing the joint. Relative to joint stability, neuromuscular control is the unconscious activation of the dynamic restraints occurring in preparation for and in response to joint motion and loading for the purpose of maintaining and restoring functional joint stability.71 Neuromuscular control of joint stability is a complex interaction between components of the nervous system and those of the musculoskeletal system and typically is accomplished through two different control systems, feedback and feed-forward control.23 In a system that uses feedback control, sensors continually measure the parameter of interest based on an optimal value. A deviation from this optimal value will initiate an error signal. In response to this error signal, the system will trigger a compensatory response. Feed-forward systems also require measurement of a parameter, but measurement occurs only intermittently. The sensory components of this system are designed to measure a potential disturbance or change in the parameter of interest. Once a potential disturbance has been detected, the system initiates an error signal. In response to this error signal, the system institutes commands to counteract the anticipated effects of the disturbance. The commands instituted by this system are largely shaped by previous experience with similar disturbances. Feed-forward control systems are considered to be anticipatory in nature compared with feedback control systems, which are characterized by responses only to current stimulus. Both are essential for optimal maintenance of dynamic knee stability.
NONCONTACT ANTERIOR CRUCIATE LIGAMENT INJURIES AND FEMALE ATHLETES
The role of dynamic joint stability in the prevention of knee injuries has been a focus of research at the University of Pittsburgh and the Neuromuscular Research Laboratory since 1995 in response to the demonstrated differences in noncontact anterior cruciate ligament (ACL) injury rates between male and female athletes. Female athletes suffer ACL injuries at a significantly higher rate than male athletes in matched sports.1–3,9,15,17,26–28,59,63 The majority of these injuries occur through a noncontact mechanism of injury in which no external forces are applied directly to the knee joint.10,57,64 The forces that cause the injury are applied to the knee joint through ground reaction forces and internal soft tissue and muscle forces. An examination of gender-specific characteristics is an important first step in determining potential risk factors and prevention of these injuries. Researchers have investigated numerous potential risk factors for noncontact ACL injuries including anatomic, hormonal, environmental, neuromuscular, and biomechanical characteristics. The primary and current focus in female noncontact ACL injury prevention (risk factor identification and training) is on the neuromuscular and biomechanical factors of joint stability owing to their potential for modification through intervention programs.12,29,31,50,52,62,70,87
PROPRIOCEPTION
Proprioception is the afferent information arising from the internal peripheral areas of the body that contribute to postural control, joint stability, and conscious sensations. These include the conscious submodalities of proprioception: joint position sense, active and passive kinesthesia, the sense of heaviness or resistance, and appreciation of movement velocity. Proprioception is an important component to establish and maintain functional joint stability.45,67 Alterations in the acquisition, processing, and integration of proprioceptive information can affect functional joint stability. The presence of knee joint proprioception deficits in females may contribute to their increased rate of ACL injury, because the lack of proprioception inhibits recruitment of the dynamic stabilizers that prevent anterior tibial translation.
Critical Points PROPRIOCEPTION
The proprioceptive characteristics of male and female athletes were examined in 34 collegiate-level athletes.75 Knee joint proprioception was measured by assessing the threshold to detect passive motion with a custom-built testing device (Department of Engineering, University of Pittsburgh). The device was capable of rotating the knee joint at 0.5°/sec, which is necessary to reduce the input of musculotendinous mechanoreceptors. Subjects were tested in a seated position while wearing a pneumatic sleeve on their tested lower leg, a blindfold over their eyes, and headphones with white noise in order to reduce cutaneous input, visual input, and auditory input, respectively (Fig. 17-1). Participants were instructed to signal (with a button signal) when joint motion was sensed. Direction of movement was randomized across six trials (three in each direction), with data averaged for each direction. The amount of rotation before the participants’ signal was recorded as the threshold to detect passive motion. Testing was performed at a knee flexion angle of 15° with movement into both flexion and extension. This position was chosen because most noncontact ACL injuries occur with the knee close to full extension.10,57,65 Reliability of the device was demonstrated to be high.47

No differences were observed between male and female athletes when the knee was rotated into flexion, but a significant difference was found when the knee was rotated toward full extension (Fig. 17-2). The ACL becomes tauter as the knee extends, and although the female subjects in this study had greater knee joint laxity, this may provide evidence for the increased risk of ACL injury (noncontact) in female athletes. The decreased ability to detect motion toward a dangerous position10,57,65 of full extension could prevent preactivation of protective muscle forces such as the hamstrings.
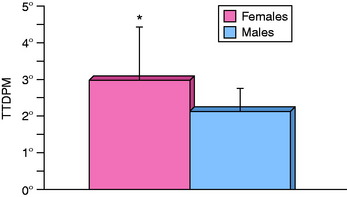
FIGURE 17-2 Gender differences in TTDPM (*P = .039).
(From Rozzi, S. L.; Lephart, S. M.; Gear, W. S.; Fu, F. H.: Knee joint laxity and neuromuscular characteristics of male and female soccer and basketball players. Am J Sports Med 27:312–319, 1999.)
Although proprioception differences exist between genders, differences also exist in proprioception abilities within the female athletic population.44 A comparison of the threshold to detect passive motion was conducted between female gymnasts and a group of healthy, age-matched participants. The instrumentation and methodology of testing were similar to that of the gender comparison study described previously. Gymnasts recognized movement significantly faster than the nongymnasts (Fig. 17-3). It is recognized that the superior kinesthetic awareness observed in the gymnasts may be due to one or multiple factors:
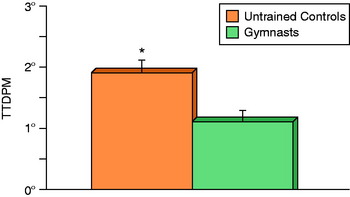
FIGURE 17-3 Gymnasts demonstrate superior TTDPM compared with untrained controls (*P = .011).
(From Lephart, S. M.; Giraldo, J. L.; Borsa, P. A.; Fu, F. H.: Knee joint proprioception: a comparison between female intercollegiate gymnasts and controls. Knee Surg Sports Traumatol Arthrosc 4:121–124, 1996.)
BALANCE AND POSTURAL STABILITY
Postural stability is the ability to maintain the body in equilibrium by maintaining the projected center of mass within the limits of the base of support.81 Similar to joint stability, maintenance of postural stability is a dynamic process that involves establishing an equilibrium between destabilizing and stabilizing forces.56 Sensory information for this stability is derived from vision, the vestibular system, and somatosensory feedback.38 Somatosensory feedback is also necessary for dynamic knee stability and is incorporated into the sensorimotor system in order to maintain stability both in dynamic tasks and in static posture.38,71 Although researchers have cautioned against extrapolating data from static conditions to dynamic athletic situations, postural stability testing can provide valuable information regarding sensory integration, processing, and motor planning.85
The sensorimotor system provides the sensory information and action components that influence the perception, cognition, and action processes that are paramount to dynamic knee stability.71 Sensorimotor processes involved in dynamic knee stability include the neurosensory and neuromuscular mechanisms involved in the acquisition of a sensory stimulus, the conversion of the stimulus to a neural signal, transmission of the signal to the central nervous system (CNS), processing and integration of the signal within the CNS, and the motor responses resulting in muscle activation for joint stability during locomotion and functional tasks.46 Accurate sensory information is critical to this system.71 Without accurate sensory information, the proper corrective actions cannot be planned and executed.
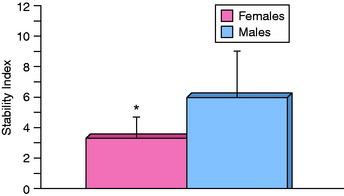
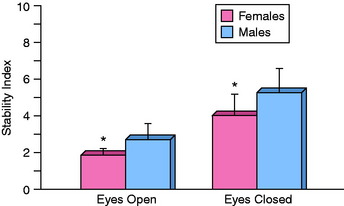
Overall, the authors’ research demonstrates that female athletes have superior balance than male athletes. A study was conducted that measured and compared the balance of male college-aged athletes and female National Collegiate Athletic Association (NCAA) Division I athletes using the Biodex Stability System (Biodex, Inc., Shirley, NY).75 The Biodex software generates a stability index value that is based on the amount of time the platform is off-level. Female athletes had a significantly greater stability index than their male counterparts (Fig. 17-4). In another study, single-leg balance was measured on a traditional force plate (Kistler Corporation, Worthington, OH; Model #4060-1011000).80 Testing methodology and data processing were based on that described by Goldie and coworkers24,25 and included both an eyes-closed and an eyes-open condition. Comparisons were made between male and female high school basketball players. Females demonstrated significantly better single-leg balance scores for both the eyes-closed and the eyes-opened conditions (Fig. 17-5).
Critical Points BALANCE AND POSTURAL STABILITY
It is interesting to note that many noncontact ACL injury prevention training programs include activities designed to improve balance12,29,31,42,51,62 despite the fact that females have significantly better single-leg balance and that single-leg balance deficits have not been identified as a risk factor for ACL injury. The lack of balance deficits seems to contradict the research demonstrating that females have proprioceptive deficits. The authors proposed that the measurement of static single-leg balance might not adequately challenge the underlying motor control and peripheral somatosensory system. A more dynamic test of postural control would be more appropriate and likely to reveal potential deficits related to the acquisition, processing, and integration of somatosensory information and functional joint stability. Currently, the authors are conducting a study examining single-leg balance (static) and dynamic postural control. The goals of this study are to establish the reliability of a test of dynamic postural control, determine the relationships between static balance tests and dynamic balance tests, and determine whether gender differences are present in dynamic postural control.
EMG ACTIVITY
The electromyogram measures the electrical manifestation of the contracting muscle.4 It is the electrical signal that propagates from the neuromuscular junction along the muscle fiber and is termed the muscle action potential.33 Measurement of EMG activity provides information regarding the amount of electrical activity in the contracting muscle, which provides insight into the magnitude of tension developed.86 Many variables can influence this signal and thus create difficulty in interpreting these data. These variables include velocity of muscle shortening or lengthening, rate of tension buildup, fatigue, and reflex activity.89 Muscle activation patterns, amplitude, and quantity provide important insight into the neuromuscular control of joint stability.
Dynamic knee stability is dependent on the neuromuscular control over the musculature of the knee in order to reduce strain in the ACL. For this control to be effective, the CNS must be able to anticipate destabilizing forces and act appropriately.8 Benvenuti and associates6 examined EMG activity of upper arm musculature during reaction-time arm movements and demonstrated that when destabilizing forces are anticipated, the CNS is capable of adjusting muscle activation patterns to oppose these forces, supporting the notion that anticipatory postural adjustments are planned in detail. EMH activity of the knee musculature has been investigated and compared between genders during athletic tasks in an attempt to quantify the role of the knee extensors and flexors in dynamic knee stability.7,14,49
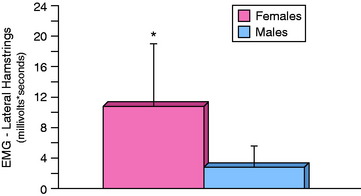
The authors measured the EMG activity of the vastus medialis, vastus lateralis, medial hamstrings, lateral hamstrings, and gastrocnemius with surface electrodes while athletes performed a drop-land task.75 Comparisons between genders were performed for the activity onset time after initial contact and peak amplitude after initial contact. In addition, the area of activity (integrated) for the first 1 second of the contraction after landing was calculated for each muscle. No significant differences were observed for onset time for any of the muscles. Analysis of the peak amplitude and integrated electromyographic (IEMG) activity revealed a significant difference between genders for the lateral hamstrings; females had a greater peak amplitude and IEMG activity (Fig. 17-6) than males. Activation of the lateral hamstrings in response to the landing is an attempt by female athletes to prevent the anterior tibial translation that occurs as the knee flexes. It may also be an attempt to counteract potential anterolateral subluxations due to its insertion on the fibular head.
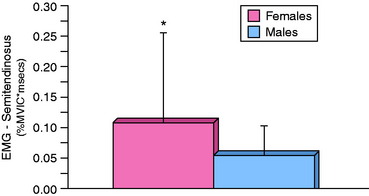
Gender differences have also been observed in EMG activation during reactive stop-jump tasks and stop-jump tasks designed to simulate tasks during which noncontact ACL injuries occur.78 The IEMG activity of the vastus lateralis and semitendinosus was measured during the 150 msec prior to peak posterior ground reaction force (maximum deceleration) while male and female high school basketball players performed reactive jumps. This particular time point was chosen because deceleration is the most common characteristic among those tasks during which noncontact ACL injuries occur.10,65 In addition, a co-contraction value (vastus lateralis and semitendinosus) was calculated during this same time period. Female athletes performed these reactive jumps with a greater IEMG activity of the semitendinosus (Fig. 17-7) and a higher co-contraction value.
Similar gender differences were observed during an examination of stop-jump tasks to the medial aspect of the knee. The authors’ biomechanical analyses of jump direction demonstrated that stop-jump tasks directed to the medial aspect of the knee (such as an inside cut) are more dangerous than vertical jumps and stop-jump tasks to the lateral aspect of the knee.78 Athletes perform these jumps with the greatest vertical and posterior ground reaction forces, greatest proximal anterior tibia shear force, highest valgus and flexion moments, and lowest knee flexion angles. Female athletes use the same IEMG activation patterns during these jumps as during the reactive jumps. The gender differences observed in semitendinosus activity during these stop-jump tasks are consistent with a previous study75 and reinforce the concept that females use compensatory strategies to counter the decreased knee joint proprioception in order to achieve functional joint stabilization.
STRENGTH
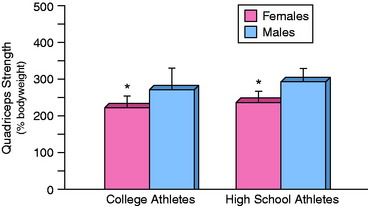
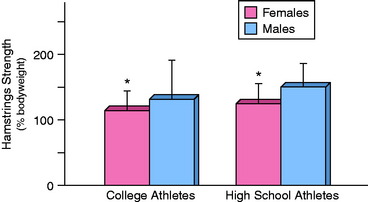
Muscular strength can assist dynamic knee stability by producing force that aids to counteract the destabilizing forces occurring during dynamic activities. For the knee joint, these forces are primarily provided by knee flexors and knee extensors. Knee strength testing provides information regarding the potential force production capabilities of those muscles crossing the knee joint. The authors’ research has consistently demonstrated gender differences in athletes for both the knee extensors and the knee flexors. The isokinetic knee extensor and flexor strength of 15 female NCAA Division I volleyball, basketball, and soccer athletes was tested (60°/sec) and compared with those of males of similar age and activity level who had previously participated in soccer and basketball.43 A Biodex System III Dynamometer (Biodex Medical Inc., Shirley, NY) provided scores of peak torque that were normalized to each participant’s body weight. Females produced significantly less peak torque for both the knee extensors and the knee flexors compared with males (Figs. 17-8 and 17-9). Similar observations of isokinetic strength (60°/sec) have been made in high school athletes for knee extensors and knee flexors.80 Male high school basketball players demonstrated significantly stronger knee extensors and flexors than female basketball players when normalized to body weight (see Figs. 17-8 and 17-9).
The authors recognize the significant contributions, including strength, of the joints proximal and distal (to the knee) to functional joint stability of the knee. An analysis and gender comparison was conducted of hip strength of high school basketball players.18 Hip external rotation and abductor strength was assessed with a hand-held dynamometer. Measurements of strength were normalized to each participant’s segment length and body weight. No significant gender differences were observed in hip abductor strength, although females had less strength than males. Females demonstrated significantly less hip external rotation strength than males. These differences in hip strength reinforce the need to include proximal strengthening exercises for the knee joint.
BIOMECHANICS
The differences observed in proprioception, EMG activity, and strength can lead to differences in neuromuscular control of the knee during dynamic tasks. The result of this difference in neuromuscular control is evident in biomechanical differences observed in dynamic tasks. The authors have examined the biomechanics of males and females performing several different tasks (Fig. 17-10) to determine how neuromuscular control (deficits) affects landing kinematics and kinetics.

The landing kinematics and ground reaction forces of 15 female NCAA Division I collegiate basketball, volleyball, and soccer athletes were measured.43 These data were compared with those of male recreational athletes matched for age and activity level. Landing kinematics and vertical ground reaction forces were examined while the participants performed single-leg landings and forward hops. During the single-leg hops, the female athletes demonstrated greater internal rotation of the hip, less knee flexion (Fig. 17-11), less lower leg maximum angular displacement, and decreased time to maximum angular displacement (flexion) than their male counterparts. Females also demonstrated less knee flexion, lower leg internal rotation, and decreased time to maximum angular displacement (flexion) than males during the forward hop. Ground reaction forces were not significantly different between genders during the two tasks studied.
A series of jump tasks were developed to better replicate those tasks during which noncontact ACL injuries occur.10,57,65 Two of the most common components include a sharp deceleration, such as a cutting maneuver or stop-jump, and a quick change in direction. Olsen and colleagues65 also described that many of these injuries occur with a valgus collapse of the knee. The joint kinematic, joint kinetics, and ground reaction forces were examined during the stop-jump in three different directions (left, right, and vertical). Each jump began with a two-legged broad jump to two force plates, followed by an immediate (as fast as possible) jump in the designated direction. The results of this study indicated that direction had a significant effect on biomechanics during these stop-jump tasks. Jumps to the medial aspect of the studied knee (e.g., jumps to the left during an examination of the right knee) resulted in the highest vertical ground reaction forces, greatest deceleration forces (posterior ground reaction forces), highest proximal anterior tibia shear force, highest valgus and flexion moments, and lowest knee flexion angles. They concluded that this particular jump was the most dangerous owing to the potential risk of injury30 and increased ACL strain.19,53,76 This type of jump also mirrors the observations of Olsen and colleagues.65
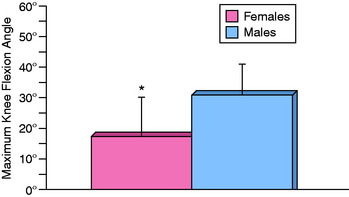
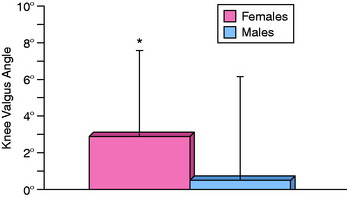
Based on the results of the comparison of jump direction, the authors examined the potential differences in joint kinematics, joint kinetics, and ground reaction forces between genders when performing the most dangerous of the three jumps, jumps to the medial aspect of the knee. Females performed jumps to the left with significantly less flexion at the time of peak posterior ground reaction force (PPGRF) and had less total flexion. Females also performed these tasks with a significantly greater knee valgus angle at PPGRF (Fig. 17-12). PPGRF was chosen as a time point because it is a common characteristic across the multitude of tasks that have been identified as those during which noncontact ACL injuries occur.10,57,65 Tasks such as landing, stopping, stop-jump, and cutting all have one common component—a sharp deceleration. Deceleration during a dynamic task can be measured by posterior ground reaction forces. They concluded that female athletes perform the most dangerous of landing tasks differently than males and in a manner that increases their susceptibility to ligament injury.
The majority of biomechanical analyses of dynamic tasks have been performed during controlled laboratory experiments.13,20,31,43,49,68,77 Whereas these studies have been valuable, they may not represent the best simulation of actual athletic competition. Actual athletic competition requires the participant to react on a millisecond-by-millisecond basis to unanticipated events. Knowledge of the task to be performed allows individuals to preplan movement patterns. To better replicate these unanticipated events, the authors designed and implemented a novel testing model.78 Eighteen male and 17 female high school basketball players performed a series of 30 jumps in three different directions under two different conditions (planned and reactive). The task was a stop-jump maneuver that began with a two-legged broad jump to two force plates, followed by an immediate jump in one of three directions (left, right, or vertical). For half of the jumps (randomized order), the participants had to react to a visual cue for jump direction. The visual cue was triggered by a laser coupled with a photocell that was instrumented with a videographic monitor via a Matlab program (Release 12, The MathWorks, Natick, MA). Comparisons between the planned and the reactive tasks revealed significant differences for most of the biomechanical variables. During the reactive jumps, female participants landed with less knee flexion at PPGRF and a greater maximum knee flexion angle and experienced greater deceleration forces, knee flexion moments, and knee valgus moments (Table 17-1). These differences indicate that these laboratory experiments may be different from actual game situations.
TABLE 17-1 Comparison between Jump Tasks (Planned vs. Reactive)
| Planned* | Reactive* | |
|---|---|---|
| Knee flexion angle at PPGRF (°)† | 29.5 ± 11.8 | 24.4 ± 10.4 |
| Maximum knee flexion angle (°)† | 68.6 ± 12.8 | 71.7 ± 11.0 |
| Knee valgus angle at PPGRF (°) | 0.4 ± 6.4 | 0.5 ± 5.6 |
| Maximum knee valgus angle (°) | –4.7 ± 8.7 | –5.8 ± 9.3 |
| Maximum vertical ground reaction force (body weight) | 2.23 ± 0.90 | 2.18 ± 0.88 |
| Maximum posterior ground reaction force (body weight)† | –0.70 ± 0.24 | –0.81 ± 0.29 |
| Proximal anterior tibia shear force at PPGRF (body weight) | 0.318 ± 0.198 | 0.283 ± 0.171 |
| Maximum proximal anterior shear force (body weight) | 0.97 ± 0.23 | 0.93 ± 0.23 |
| Knee flexion moment at PPGRF (body weight x height)† | –0.040 ± 0.045 | –0.054 ± 0.039 |
| Maximum knee flexion moment (body weight x height) | –0.152 ± 0.037 | –0.161 ± 0.047 |
| Knee valgus moment at PPGRF (body weight x height) | –0.017 ± 0.025 | –0.013 ± 0.025 |
| Maximum knee valgus moment (body weight x height)† | –0.044 ± 0.019 | –0.050 ± 0.020 |
| Vastus lateralis IEMG | 0.122 ± 0.338 | 0.076 ± 0.054 |
| Semitendinosus IEMG | 0.077 ± 0.099 | 0.068 ± 0.097 |
| Co-contraction value | 0.088 ± 0.089 | 0.073 ± 0.063 |
IEMG, integrated electromyogram; PPGRF, peak posterior ground reaction force.
* Data shown are mean ± standard deviation.
† Significant difference observed between tasks (P < .05).
From Sell, T. C.; Ferris, C. M.; Abt, J. P.; et al.: The effect of direction and reaction on the neuromuscular and biomechanical characteristics of the knee during tasks that simulate the noncontact anterior cruciate ligament injury mechanism. Am J Sports Med 34:43–54, 2006.
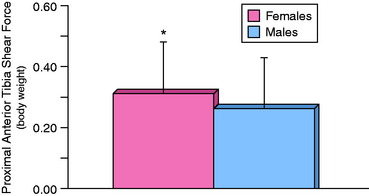
A secondary analysis was performed to compare biomechanical characteristics of males and females during reactive tasks. Females performed the reactive tasks with less flexion, greater valgus angle, greater proximal anterior tibia shear force (Fig. 17-13), and a greater knee flexion moment. The differences observed between genders are consistent with what is observed under planned conditions, but the differences between planned and reactive tasks demonstrate the need to develop testing models that better replicate actual game conditions.
Dynamic knee stability is essential in reducing the destabilizing forces during dynamic activities. Athletes must be able to perform the activities required in their sport while reducing those forces that can lead to joint injury. At the knee, one of those forces is proximal tibia anterior shear force. Proximal tibia anterior shear force is the most direct loading mechanism of the ACL11,53–55 and may be estimated through inverse dynamics. Yu and coworkers89 described how proximal tibia anterior shear force (estimated through inverse dynamics) may be an indicator of ACL loading. Females have been shown to perform dynamic tasks with greater proximal tibia anterior shear force. A regression analysis was conducted to determine the biomechanical and neuromuscular predictors of proximal tibia anterior shear force.79 The analysis included knee flexion angle, knee valgus angle, knee flexion moment, knee valgus moment, PPGRF, IEMG activity of the vastus lateralis and semitendinosus, and gender. These variables were chosen because of their previously identified relationships with ACL strain and/or ACL injury.11,53–55
FATIGUE
The effects of fatigue (both central and peripheral) have been studied on neuromuscular and biomechanical characteristics.5,74 Muscular fatigue may disrupt or degrade the compensatory stabilizing mechanisms necessary to maintain joint stability in the presence of destabilizing forces and moments.74 Numerous studies indicate that athletic injuries are more common in the later stages of activity and competition.16,21,23,61,66,73,84 The reasons for this are unclear, but may be due to the effects of fatigue on decreased motor control,36,88 increased knee joint laxity,34,74,82 decreased balance skill,36 and decreased proprioception.32,40,41,60 The authors conducted two studies examining the effects of fatigue on neuromuscular and biomechanical characteristics.
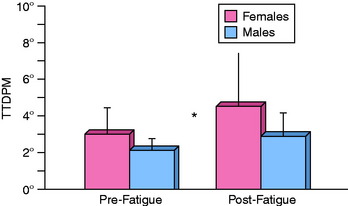
The first study examined knee joint laxity, kinesthesia (via threshold to detect passive motion), lower extremity balance, and surface EMG activity during a landing maneuver of male and female athletes before and after a peripheral muscular fatigue protocol.74 The fatigue protocol was designed to induce peripheral fatigue of the knee flexors and extensors and was implemented using a Biodex Isokinetic Dynamometer. Seventeen male and 17 female collegiate athletes performed three sets of maximum contraction at 180°/sec, or until their torque production fell below 25% of their initial peak torque production. The fatigue protocol had a significant effect on the neuromuscular characteristics of both males and females. The ability to detect joint motion, measured through threshold to detect passive motion, was decreased during knee joint motion toward full extension (Fig. 17-14). In addition, both males and females demonstrated an increase in the contraction onset time for the medial hamstrings and gastrocnemius and increased IEMG activity of the vastus lateralis and vastus medialis. The results of this series of neuromuscular testing indicate that both males and females are at an increased risk for ligamentous injury under fatigued conditions.
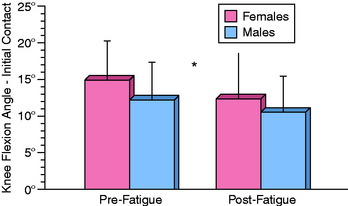
The second study examined the kinematic characteristics of the hip and knee during a single-leg stop-jump task before and after an exhaustive run. The exhaustive run was designed to induce general/central fatigue and was performed on a treadmill using a modified Astrand protocol.39,69 Lower extremity kinematic measurements were taken of male and female college-aged recreational athletes. All subjects demonstrated a decreased knee flexion angle at initial contact and decreased maximum valgus angle (Fig. 17-15).5 Landing with less knee flexion may be an attempt to improve knee stability by decreasing the available knee valgus-varus and internal-external rotation. Unfortunately, this landing may also increase ACL strain19,53–55,76 and place individuals at greater risk for ACL rupture at the latter stages of games/competition. Overall, it appears as though fatigue affects both genders equally.
CURRENT RESEARCH
The authors continue to conduct research on injury prevention and control in female athletes, but have expanded and applied subject models to Army soldiers and Naval Special Warfare operators. These models use the public health approach to the injury control process.37,58,72 This model integrates a five-step process designed to determine injury patterns and ultimately evaluate the effectiveness of intervention programs to reduce the incidence of injuries. Human performance testing has been incorporated in order to enhance training techniques. The ultimate goals of these projects are to reduce the incidence and severity of injuries, minimize the necessity for surgery, promote longevity, enhance performance, and optimize military readiness.
1 Agel J., Arendt E.A., Bershadsky B. Anterior cruciate ligament injury in National Collegiate Athletic Association basketball and soccer: a 13-year review. Am J Sports Med. 2005;33:524-531.
2 Arendt E., Agel J., Dick R. Anterior cruciate ligament injury patterns among collegiate men and women. J Athl Train. 1999;34:86-92.
3 Arendt E., Dick R. Knee injury patterns among men and women in collegiate basketball and soccer. NCAA data and review of literature. Am J Sports Med. 1995;23:694-701.
4 Basmajian J.V. Muscles Alive, Their Functions Revealed by Electromyography, 4th ed. Baltimore: Williams & Wilkins, 1978.
5 Benjaminse A., Habu A., Sell T.C., et al. Fatigue alters lower extremity kinematics during a single-leg stop-jump task. Knee Surg Sports Traumatol Arthrosc. 2008;16:400-407.
6 Benvenuti F., Stanhope S.J., Thomas S.L., et al. Flexibility of anticipatory postural adjustments revealed by self-paced and reaction-time arm movements. Brain Res. 1997;761:59-70.
7 Besier T.F., Lloyd D.G., Ackland T.R. Muscle activation strategies at the knee during running and cutting maneuvers. Med Sci Sports Exerc. 2003;35:119-127.
8 Besier T.F., Lloyd D.G., Ackland T.R., Cochrane J.L. Anticipatory effects on knee joint loading during running and cutting maneuvers. Med Sci Sports Exerc. 2001;33:1176-1181.
9 Bjordal J.M., Arnly F., Hannestad B., Strand T. Epidemiology of anterior cruciate ligament injuries in soccer. Am J Sports Med. 1997;25:341-345.
10 Boden B.P., Dean G.S., Feagin J.A.Jr., Garrett W.E.Jr. Mechanisms of anterior cruciate ligament injury. Orthopedics. 2000;23:573-578.
11 Butler D.L., Noyes F.R., Grood E.S. Ligamentous restraints to anterior-posterior drawer in the human knee. A biomechanical study. J Bone Joint Surg Am. 1980;62:259-270.
12 Caraffa A., Cerulli G., Projetti M., et al. Prevention of anterior cruciate ligament injuries in soccer. A prospective controlled study of proprioceptive training. Knee Surg Sports Traumatol Arthrosc. 1996;4:19-21.
13 Chappell J.D., Yu B., Kirkendall D.T., Garrett W.E. A comparison of knee kinetics between male and female recreational athletes in stop-jump tasks. Am J Sports Med. 2002;30:261-267.
14 Cowling E.J., Steele J.R. Is lower limb muscle synchrony during landing affected by gender? Implications for variations in ACL injury rates. J Electromyogr Kinesiol. 2001;11:263-268.
15 Cox J.S., Lenz H.W. Women midshipmen in sports. Am J Sports Med. 1984;12:241-243.
16 Feagin J.A.Jr., Lambert K.L., Cunningham R.R., et al. Consideration of the anterior cruciate ligament injury in skiing. Clin Orthop Rel Res. 1987;216:13-18.
17 Ferretti A., Papandrea P., Conteduca F., Mariani P.P. Knee ligament injuries in volleyball players. Am J Sports Med. 1992;20:203-207.
18 Ferris C.M. Relationship of pelvis and hip neuromechanical characteristics to the knee during a stop-jump task. Pittsburgh: Department of Sports Medicine and Nutrition, University of Pittsburgh, 2003. Dissertation
19 Fleming B.C., Renstrom P.A., Beynnon B.D., et al. The effect of weightbearing and external loading on anterior cruciate ligament strain. J Biomech. 2001;34:163-170.
20 Ford K.R., Myer G.D., Toms H.E., Hewett T.E. Gender differences in the kinematics of unanticipated cutting in young athletes. Med Sci Sports Exerc. 2005;37:124-129.
21 Gabbett T.J. Incidence, site, and nature of injuries in amateur rugby league over three consecutive seasons. Br J Sports Med. 2000;34:98-103.
22 Gabbett T.J. Incidence of injury in junior and senior rugby league players. Sports Med. 2004;34:849-859.
23 Ghez C., Krakauer J. The organization of movement. In: Kandel E.R., Schwartz J.H., Jessell T.M., editors. Principles of Neural Science. New York: McGraw-Hill; 2000:653-673. Health Professions Division
24 Goldie P.A., Bach T.M., Evans O.M. Force platform measures for evaluating postural control: reliability and validity. Arch Phys Med Rehabil. 1989;70:510-517.
25 Goldie P.A., Evans O.M., Bach T.M. Steadiness in one-legged stance: development of a reliable force-platform testing procedure. Arch Phys Med Rehabil. 1992;73:348-354.
26 Gomez E., DeLee J.C., Farney W.C. Incidence of injury in Texas girls’ high school basketball. Am J Sports Med. 1996;24:684-687.
27 Gwinn D.E., Wilckens J.H., McDevitt E.R., et al. The relative incidence of anterior cruciate ligament injury in men and women at the United States Naval Academy. Am J Sports Med. 2000;28:98-102.
28 Harrer M.F., Berson L., Hosea T.M., Leddy T.P. Lower extremity injuries: females vs. males in the sport of basketball. FL: Lake Buena Vista, June 16–20, 1996. Paper presented at American Orthopaedic Society for Sports Medicine 22nd Annual Meeting
29 Hewett T.E., Lindenfeld T.N., Riccobene J.V., Noyes F.R. The effect of neuromuscular training on the incidence of knee injury in female athletes. A prospective study. Am J Sports Med. 1999;27:699-706.
30 Hewett T.E., Myer G.D., Ford K.R., et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33:492-501.
31 Hewett T.E., Stroupe A.L., Nance T.A., Noyes F.R. Plyometric training in female athletes. Decreased impact forces and increased hamstring torques. Am J Sports Med. 1996;24:765-773.
32 Hiemstra L.A., Lo I.K., Fowler P.J. Effect of fatigue on knee proprioception: implications for dynamic stabilization. J Orthop Sports Phys Ther. 2001;31:598-605.
33 Hillstrom H.J., Triolo R.J. EMG theory. In Craik R.L., Oatis C.A., editors: Gait Analysis: Theory and Application, 1st ed., St. Louis: Mosby, 1995.
34 Huston L.J., Wojtys E.M. Neuromuscular performance characteristics in elite female athletes. Am J Sports Med. 1996;24:427-436.
35 Johansson H., Sjolander P. The neurophysiology of joints. In: Wright V., Radin E.L., editors. Mechanics of Joints: Physiology, Pathophysiology, and Treatment. New York: Marcel Dekker; 1993:243-290.
36 Johnston R.B.3rd, Howard M.E., Cawley P.W., Losse G.M. Effect of lower extremity muscular fatigue on motor control performance. Med Sci Sports Exerc. 1998;30:1703-1707.
37 Jones B.H., Knapik J.J. Physical training and exercise-related injuries. Surveillance, research and injury prevention in military populations. Sports Med. 1999;27:111-125.
38 Kandel E.R., Schwartz J.H., Jessell T.M. Principles of Neural Science, 3rd ed. Norwalk, CT: Appleton & Lange, 1991.
39 Kang J., Chaloupka E.C., Mastrangelo M.A., et al. Physiological comparisons among three maximal treadmill exercise protocols in trained and untrained individuals. Eur J Appl Physiol. 2001;84:291-295.
40 Lattanzio P.J., Petrella R.J. Knee proprioception: a review of mechanisms, measurements, and implications of muscular fatigue. Orthopedics. 1998;21:463-470.
41 Lattanzio P.J., Petrella R.J., Sproule J.R., Fowler P.J. Effects of fatigue on knee proprioception. Clin J Sport Med. 1997;7:22-27.
42 Lephart S.M., Abt J.P., Ferris C.M., et al. Neuromuscular and biomechanical characteristic changes in high school athletes: a plyometric versus basic resistance program. Br J Sports Med. 2005;39:932-938.
43 Lephart S.M., Ferris C.M., Riemann B.L., et al. Gender differences in strength and lower extremity kinematics during landing. Clin Orthop Relat Res. 2002;401:162-169.
44 Lephart S.M., Giraldo J.L., Borsa P.A., Fu F.H. Knee joint proprioception: a comparison between female intercollegiate gymnasts and controls. Knee Surg Sports Traumatol Arthrosc. 1996;4:121-124.
45 Lephart S.M., Pincivero D.M., Rozzi S.L. Proprioception of the ankle and knee. Sports Med. 1998;25:149-155.
46 Lephart S.M., Riemann B.L., Fu F.H. Introduction to the sensorimotor system. In: Lephart S., Fu F.H., editors. Proprioception and Neuromuscular Control in Joint Stability. Champaign, IL: Human Kinetics; 2000:xxiv-xxv.
47 Lephart S.M., Warner J.J.P., Borsa P.A., Fu F.H. Proprioception of the shoulder joint in healthy, unstable, and surgically repaired shoulders. J Shoulder Elbow Surg. 1994;3:371-380.
48 Lew W.D., Lewis J.L., Craig E.V. Stabilization by capsule, ligaments, and labrum: stability at the extremes of motion. In: Matsen F.A., Fu F.H., Hawkins R.J., editors. The Shoulder: A Balance of Mobility and Stability. Rosemont, IL: American Academy of Orthopaedic Surgeons; 1993:69-89.
49 Malinzak R.A., Colby S.M., Kirkendall D.T., et al. A comparison of knee joint motion patterns between men and women in selected athletic tasks. Clin Biomech (Bristol, Avon). 2001;16:438-445.
51 Mandelbaum B.R., Silvers H.J., Watanabe D.S., et al. Effectiveness of a neuromuscular and proprioceptive training program in preventing anterior cruciate ligament injuries in female athletes: 2-year follow-up. Am J Sports Med. 2005;33:1003-1010.
52 Mandelbaum B.R., Silvers H.J., Watanabe D.T., et al. Effectiveness of a neuromuscular and proprioceptive training program in preventing the incidence of ACL injuries in female athletes: year two. New Orleans, 2003. Paper presented at American Orthopaedic Society of Sports Medicine
53 Markolf K.L., Burchfield D.M., Shapiro M.M., et al. Combined knee loading states that generate high anterior cruciate ligament forces. J Orthop Res. 1995;13:930-935.
54 Markolf K.L., Gorek J.F., Kabo J.M., Shapiro M.S. Direct measurement of resultant forces in the anterior cruciate ligament. An in vitro study performed with a new experimental technique. J Bone Joint Surg Am. 1990;72:557-567.
55 Markolf K.L., Mensch J.S., Amstutz H.C. Stiffness and laxity of the knee—the contributions of the supporting structures. A quantitative in vitro study. J Bone Joint Surg Am. 1976;58:583-594.
56 McCollum G., Leen T. The form and exploration of mechanical stability limits in erect stance. J Mot Behav. 1989;21:225-238.
57 McNair P.J., Marshall R.N., Matheson J.A. Important features associated with acute anterior cruciate ligament injury. N Z Med J. 1990;103:537-539.
58 Mercy J.A., Rosenberg M.L., Powell K.E., et al. Public health policy for preventing violence. Health Aff (Millwood). 1993;12:7-29.
59 Messina D.F., Farney W.C., DeLee J.C. The incidence of injury in Texas high school basketball. A prospective study among male and female athletes. Am J Sports Med. 1999;27:294-299.
60 Miura K., Ishibashi Y., Tsuda E., et al. The effect of local and general fatigue on knee proprioception. Arthroscopy. 2004;20:414-418.
61 Molsa J., Airaksinen O., Nasman O., Torstila I. Ice hockey injuries in Finland. A prospective epidemiologic study. Am J Sports Med. 1997;25:495-499.
62 Myklebust G., Engebretsen L., Braekken I.H., et al. Prevention of anterior cruciate ligament injuries in female team handball players: a prospective intervention study over three seasons. Clin J Sport Med. 2003;13:71-78.
63 Myklebust G., Maehlum S., Holm I., Bahr R. A prospective cohort study of anterior cruciate ligament injuries in elite Norwegian team handball. Scand J Med Sci Sports. 1998;8:149-153.
64 Noyes F.R., Matthews D.S., Mooar P.A., Grood E.S. The symptomatic anterior cruciate–deficient knee. Part II: the results of rehabilitation, activity modification, and counseling on functional disability. J Bone Joint Surg Am. 1983;65:163-174.
65 Olsen O.E., Myklebust G., Engebretsen L., Bahr R. Injury mechanisms for anterior cruciate ligament injuries in team handball: a systematic video analysis. Am J Sports Med. 2004;32:1002-1012.
66 Pettrone F.A., Ricciardelli E. Gymnastic injuries: the Virginia experience 1982–1983. Am J Sports Med. 1987;15:59-62.
67 Pincivero D.M., Lephart S.M., Karunakara R.A. Reliability and precision of isokinetic strength and muscular endurance for the quadriceps and hamstrings. Int J Sports Med. 1997;18:113-117.
68 Pollard C.D., Davis I.M., Hamill J. Influence of gender on hip and knee mechanics during a randomly cued cutting maneuver. Clin Biomech. 2004;19:1022-1031.
69 Pollock L.M., Wilmore J.H., Fox S.M. Health and Fitness through Physical Activity. New York: Wiley, 1978.
70 Prapavessis H., McNair P.J. Effects of instruction in jumping technique and experience jumping on ground reaction forces. J Orthop Sports Phys Ther. 1999;29:352-356.
71 Riemann B.L., Lephart S.M. The sensorimotor system. Part I. The physiologic basis of functional joint stability. J Athl Train. 2002;37:71-79.
72 Robertson L.S. Injury Epidemiology. New York: Oxford University Press, 1992.
73 Rodacki A.L., Fowler N.E., Bennett S.J. Vertical jump coordination: fatigue effects. Med Sci Sports Exerc. 2002;34:105-116.
74 Rozzi S.L., Lephart S.M., Fu F.H. Effects of muscular fatigue on knee joint laxity and neuromuscular characteristics of male and female athletes. J Athl Train. 1999;34:106-114.
75 Rozzi S.L., Lephart S.M., Gear W.S., Fu F.H. Knee joint laxity and neuromuscular characteristics of male and female soccer and basketball players. Am J Sports Med. 1999;27:312-319.
76 Sakane M., Fox R.J., Woo S.L., et al. In situ forces in the anterior cruciate ligament and its bundles in response to anterior tibial loads. J Orthop Res. 1997;15:285-293.
77 Salci Y., Kentel B.B., Heycan C., et al. Comparison of landing maneuvers between male and female college volleyball players. Clin Biomech (Bristol, Avon). 2004;19:622-628.
78 Sell T.C., Ferris C.M., Abt J.P., et al. The effect of direction and reaction on the neuromuscular and biomechanical characteristics of the knee during tasks that simulate the noncontact anterior cruciate ligament injury mechanism. Am J Sports Med. 2006;34:43-54.
79 Sell T.C., Ferris C.M., Abt J.P., et al. Predictors of proximal tibia anterior shear force during a vertical stop-jump. J Orthop Res. 2007;25:1589-1597.
80 Sell T.C., Myers J.B., Youk A.O., et al. Neuromechanical Predictors of Dynamic Stability. Pittsburgh: Department of Sports Medicine and Nutrition, University of Pittsburgh, 2004. Dissertation
81 Shumway-Cook A., Woollacott M.H. Motor Control: Theory and Practical Applications, 2nd ed. Philadelphia: Lippincott Williams & Wilkins, 2001.
82 Skinner H.B., Wyatt M.P., Stone M.L., et al. Exercise-related knee joint laxity. Am J Sports Med. 1986;14:30-34.
83 Solomonow M., Krogsgaard M. Sensorimotor control of knee stability. A review. Scand J Med Sci Sports. 2001;11:64-80.
84 Stuart M.J., Smith A. Injuries in Junior A ice hockey. A three-year prospective study. Am J Sports Med. 1995;23:458-461.
85 Williams G.N., Chmielewski T., Rudolph K., et al. Dynamic knee stability: current theory and implications for clinicians and scientists. J Orthop Sports Phys Ther. 2001;31:546-566.
86 Winter D.A. Biomechanics and Motor Control of Human Movement, 2nd ed. New York: Wiley, 1990.
87 Wojtys E.M., Huston L.J., Taylor P.D., Bastian S.D. Neuromuscular adaptations in isokinetic, isotonic, and agility training programs. Am J Sports Med. 1996;24:187-192.
88 Wojtys E.M., Wylie B.B., Huston L.J. The effects of muscle fatigue on neuromuscular function and anterior tibial translation in healthy knees. Am J Sports Med. 1996;24:615-621.
89 Yu B., Chappell J.D., Garrett W.E. Letters to the editor: author’s response. Am J Sports Med. 2006;34:313-315.