Chapter 16 Deposition disorders
1. How is “deposition disorder” defined?
Deposition disorders comprise a diverse group of conditions or diseases in which there is accumulation, deposition, or production of substances in the skin. Typically, these substances are products of abnormal metabolism or degenerative phenomena occurring locally or systemically. The major cutaneous deposits may be subdivided into the hyalinoses, mucinoses, and mineral salts.
Touart DM, Sau P: Cutaneous deposition diseases. Part I, J Am Acad Dermatol 39:149–171, 1998.
2. What is amyloid?
Amyloid is a protein with distinct tinctorial and ultrastructural properties found as extracellular deposits. It is composed of a nonfibrillary protein known as the amyloid P component and a fibrillary component that is derived from various sources. The amyloid fibril has an antiparallel, β-pleated sheet configuration. Ultrastructurally, amyloid is composed of rigid, nonbranching fibrils measuring 6 to 10 nm in diameter.
3. How is amyloid identified?
With light microscopy, amyloid appears as amorphous, hyaline-like, eosinophilic deposits. Amyloid demonstrates green birefringence with the alkaline Congo red stain, reddish metachromasia with crystal violet, and yellow-green fluorescence with thioflavin-T stain (Fig. 16-1). These stains are not absolutely specific for amyloid, as false-positive results may occur with the other hyaline-like deposition disorders.
4. Name the various types of amyloidosis.
Amyloidosis may be classified according to clinical presentation and type of amyloid fibril protein deposition (Table 16-1). The amyloid in the macular and lichenoid variants is derived from degenerated tonofilaments of keratinocytes. Nodular amyloidosis is formed from light-chain–derived AL protein produced locally by plasma cells. It cannot be distinguished from primary systemic amyloidosis, and therefore, systemic disease should be excluded in all patients with nodular amyloidosis. There are also rare forms of hereditary systemic amyloidoses that have less frequent skin manifestations.
5. What are the cutaneous manifestations of primary or myeloma-associated systemic amyloidosis? How often do they occur?
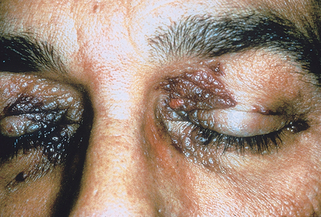
Cutaneous lesions are seen in about 30% of cases of primary or myeloma-related systemic amyloidosis. The most common skin lesions are petechiae or ecchymoses due to amyloid deposition within blood vessel walls with subsequent fragility and dermal hemorrhage. These are often seen at sites predisposed to trauma, such as the hands or intertriginous areas. Pinching the skin gives characteristic purpuric lesions known as “pinch purpura.” Purpura around the eyes may occur spontaneously but is also seen following proctoscopy or vomiting (“postproctoscopic purpura”) (Fig. 16-2). Waxy papules, nodules, or plaques may be present. Less common manifestations include sclerodermoid plaques, bullae, alopecia, and nail dystrophy.
6. Name the other organ systems that may be involved in primary or myeloma-associated amyloidosis.
Mucous membrane involvement with macroglossia occurs in 20% of cases. Hepatomegaly is found in about 50% of cases. Cardiac involvement may manifest as a restrictive cardiomyopathy or constrictive pericarditis. Peripheral nerve involvement results in paresthesias, peripheral neuropathy, and median nerve entrapment (carpal tunnel syndrome). Proteinuria is found in 80% to 90% of patients at some time during their course. Renal failure usually develops late in the disease course but may be a cause of death.

| CLINICAL DISORDER | AMYLOID PROTEIN PRECURSOR | AMYLOID PROTEIN |
|---|---|---|
| Primary systemic amyloidosis | Immunoglobulin light chain | AL |
| Myeloma-associated amyloidosis | Immunoglobulin light chain | AL |
| Secondary systemic amyloidosis | Serum amyloid A lipoprotein | AA |
| Primary localized cutaneous amyloidosis | ||
| Macular amyloidosis | Keratinocyte tonofilaments | − |
| Lichen amyloidosis | Keratinocyte tonofilaments | − |
| Nodular amyloidosis | Immunoglobulin light chain (produced locally by plasma cells) | AL |
7. Compare lichen amyloidosis and macular amyloidosis.
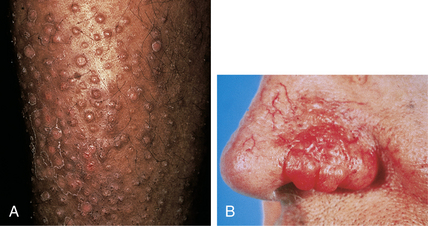
Lichen amyloidosis is the most common form of localized cutaneous amyloidosis. Lesions are pruritic, flesh-colored to brown papules, often with overlying scale (Fig. 16-3A). Papules may coalesce into verrucous plaques. The shins are the most common site of involvement. In macular amyloidosis, pruritic macular hyperpigmentation occurs most commonly in the interscapular area. The chest or extremities are less commonly involved. The lesions have a characteristic reticulate or rippled appearance. Both of these variants of primary localized cutaneous amyloidosis occur more frequently in patients from the Middle East, Asia, and Central and South America. The etiology of both lichen and macular amyloidosis is unclear but thought to be related to chronic scratching or frictional exposure. An autosomal dominant family history may be found in up to 10% of patients with lichen amyloidosis. Lichen amyloidosis is occasionally associated with multiple endocrine neoplasia type 2A.
8. How does nodular amyloidosis present? With what is it associated?
Nodular amyloidosis typically presents as solitary or multiple waxy nodules (Fig. 16-3B). Common sites of involvement include the face, scalp, lower extremities, and genitalia. It may be associated with the subsequent development of systemic amyloidosis up to 15% of cases. Rarely, it is found in association with Sjögren’s syndrome.
10. What are the systemic manifestations of secondary systemic amyloidosis?
11. What is lipoid proteinosis?
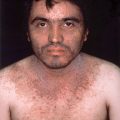
Lipoid proteinosis, also known as hyalinosis cutis et mucosae and Urbach-Wiethe disease, is a rare autosomal recessive genodermatosis in which skin and mucous membranes are infiltrated with a hyaline scleroprotein. The presenting symptom, hoarseness, develops in infancy due to involvement of the vocal cords with hyaline deposits. Bullae, pustules, and crusts, followed by acneiform scars, are seen on the face and extremities. Waxy papules develop along the eyelids, producing a characteristic “string of beads” appearance. Later, verrucous plaques occur on the elbows and knees. Lipoid proteinosis is caused by loss-of-function mutations in the extracellular matrix protein 1 gene (ECM1).
12. What is colloid milium?
Colloid milium is a cutaneous eruption characterized by flesh-colored to yellow-brown translucent papules that may coalesce into plaques. The eruption is most commonly found in adults in areas of chronic sun exposure, but a rare juvenile form is also recognized. Amorphous fissured eosinophilic material in the papillary dermis is seen on histopathology. Excessive sun exposure is a likely etiologic factor in adult colloid milium.
13. Which histologic feature or “deposit” is common to all porphyrias?
The porphyrias are a group of diseases resulting from defects in the enzymes that regulate heme biosynthesis. The biochemical and clinical features are different for each type of porphyria, yet all demonstrate similar cutaneous histology with deposits of eosinophilic, hyaline material around blood vessels. This material stains positively with the periodic acid–Schiff stain and represents reduplicated basal lamina or type IV collagen.
14. Which porphyria classically demonstrates the largest deposits? What are its cutaneous features?
Erythropoietic protoporphyria, also termed protoporphyria, has the largest eosinophilic deposits in cutaneous lesions. This autosomal dominant disorder of porphyrin metabolism is caused by a deficiency of the enzyme ferrochelatase (heme synthetase). Symptoms begin in early childhood and include photosensitivity, pruritus, burning, erythema, and edema. Chronic changes include a waxy, “cobblestone” thickening of the skin and shallow scars or pits. Increased protoporphyrin may be identified in the feces and blood, although urinary porphyrins are usually normal.
Lecha M, Puy H, Deybach JC: Erythropoietic protoporphyria, Orphanet J Rare Dis 4:19, 2009.
15. Name some of the cutaneous mucinoses.
The mucinoses are a heterogeneous group of disorders characterized by dermal mucin deposition. This mucin is largely hyaluronic acid, an acid mucopolysaccharide, with smaller amounts of chondroitin sulfate and heparin. Disorders resulting in diffuse mucin deposition include generalized myxedema, pretibial myxedema, lichen myxedematosus, scleredema, reticular erythematous mucinosis, and the mucopolysaccharidoses (storage diseases). Mucin deposition may also be focal or localized, as with follicular mucinosis (alopecia mucinosa), cutaneous focal mucinosis, and digital mucous cyst.
Jackson EM, English JC 3rd: Diffuse cutaneous mucinoses, Dermatol Clin 20:493–501, 2002.
16. Describe the clinical lesions seen in pretibial myxedema and its disease associations.
Patients with pretibial myxedema develop nodules or diffuse plaques usually on the anterior lower legs, although involvement of other sites has been rarely reported (Fig. 16-4A). The lesions result from large amounts of dermal mucin deposition. Pretibial myxedema is seen in 1% to 4% of patients with Graves’ disease and, less commonly, in patients with autoimmune thyroiditis.

17. Describe the clinical lesions seen in lichen myxedematosus.
In lichen myxedematosus, also known as papular mucinosis, numerous flesh-colored to erythematous, densely grouped lichenoid papules are found primarily on the face and arms. Rare cases have been reported in association with human immunodeficiency virus or hepatitis C infection. In the scleromyxedema variant, lesions coalesce into indurated plaques resulting in diffuse skin thickening. Scleromyxedema can involve internal organs resulting in neurologic, musculoskeletal, gastrointestinal, pulmonary, renal, and cardiovascular sequelae. Lesions of lichen myxedematosus/scleromyxedema result from an increase in both dermal mucin and fibroblasts.
18. What serum abnormality has been associated with scleromyxedema?
19. Describe the clinical lesions in scleredema and its disease associations.
Scleredema presents as a firm, woody induration of the skin typically involving the upper trunk, posterior neck, and shoulders. Histologically, it is characterized by an accumulation of dermal mucin and increased sclerosis of dermal collagen. Scleredema may be seen in several different clinical settings, including postinfection, in association with diabetes mellitus, and in the setting of paraproteinemia.
Boin F, Hummers LK: Scleroderma-like fibrosing disorders, Rheum Dis Clin North Am 34:199–220, 2008.
20. What is a digital mucous (myxoid) cyst?
A digital mucous cyst is a common solitary, asymptomatic, semitranslucent, dome-shaped nodule that typically presents in adults and elderly patients on the dorsal finger near the proximal nail fold or distal interphalangeal joint (Fig. 16-4B). It may distort the nail matrix, resulting in a groove in the nail plate. Clear, gelatinous mucoid material can be expressed from the cyst. The pathogenesis is controversial; however, it is often attributed to degenerative changes in the distal interphalangeal joints.
21. What substance is elevated in gout?
Gout is a heterogeneous group of disorders of purine metabolism resulting in elevated levels of uric acid (monosodium urate). Patients have either increased uric acid production or decreased renal excretion. Some risk factors for hyperuricemia include alcohol use, obesity, high purine diets, diabetes, myeloproliferative disorders, renal disease, and/or diuretic therapy.
22. Where is the uric acid deposited in gout? What are the resulting clinical manifestations?
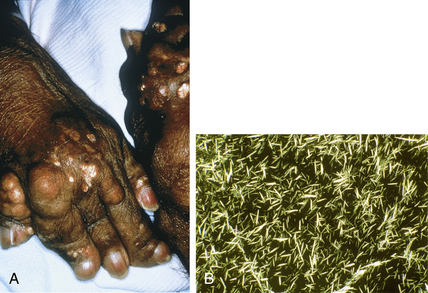
Uric acid crystals in gout are most commonly deposited in the synovium, soft tissues, and skin. The most common site is the synovium of joints, producing acute gouty arthritis. The metatarsophalangeal joint of the great toe is classically involved. Uric acid deposition in the skin and soft tissues results in gouty tophi, which are seen in 20% to 50% of patients. Common sites of involvement include the helix of the ear, elbows, and digits (Fig. 16-5A). These gouty tophi may ulcerate and discharge monosodium urate crystals that appear as a thick chalky material. Under light microscopy, these crystals are needle-shaped and birefringent (Fig. 16-5B).
23. How is gout treated?
Acute attacks of gout may be treated with a variety of agents, including colchicine, nonsteroidal antiinflammatory agents, or systemic corticosteroids. Long-term therapy may include colchicine, allopurinol, probenecid, or urine alkalinization (to increase uric acid solubility).
Eggebeen AT: Gout: an update, Am Fam Physician 76:801–808, 2007.
24. How many types of calcinosis cutis are there?
• Dystrophic calcinosis cutis: Occurs when there is deposition of calcium salts within inflamed or damaged tissue. Calcium and phosphorus metabolism is normal. It may be localized, such as within acne scars or epidermoid cysts, or widespread. Widespread dystrophic calcinosis cutis most often occurs in association with connective tissue disease, such as dermatomyositis or scleroderma.
• Metastatic calcinosis cutis: Is seen with aberrations in calcium or phosphorus metabolism. It usually occurs when the serum calcium-phosphorus product exceeds 60.
26. What is calciphylaxis and who develops it?
Calciphylaxis is a type of metastatic calcification in which there is calcification of the walls of small- and medium-sized blood vessels in the dermis and subcutis resulting in infarction of the overlying skin. Clinically, patients develop livedo reticularis–like mottling, painful hard plaques, and necrotic ulcers. It is usually seen in the setting of chronic renal failure and secondary hyperparathyroidism (Fig. 16-6). Calciphylaxis, however, has uncommonly been reported with normal levels of calcium and phosphate and in the absence of renal disease.

Daudén E, Oñate MJ: Calciphylaxis, Dermatol Clin 26:557–568, 2008.
27. What is osteoma cutis?
Osteoma cutis is the deposition of bone within cutaneous tissues. Primary osteoma cutis involves normal skin and can be associated with several syndromes including Albright hereditary osteodystrophy, fibrodysplasia ossificans progressiva, and congenital platelike osteomatosis. Secondary osteoma cutis or metaplastic ossification occurs in association with or secondary to trauma, inflammatory skin conditions, or neoplasia. Miliary osteoma cutis of the face presents as multiple, small, firm papules on the face, typically in women afflicted with acne, although it may also arise on normal skin.
Touart DM, Sau P: Cutaneous deposition diseases. Part II, J Am Acad Dermatol 39:527–544, 1998.