Chapter 3 Debridement of the Injured Cartilage
Introduction
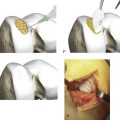
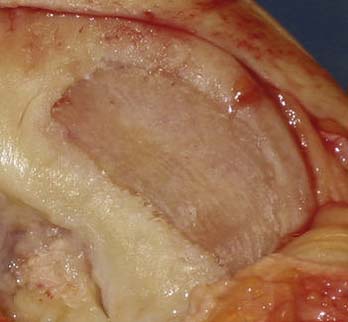
Cartilage lesions could be either traumatic or nontramatic. Common for all lesions are that they are irregular and need to be cleaned for a secure repair possibility, irrespective of which type of repair is to be used (Fig. 3-1):

FIGURE 3-1 An irregular defect to be debrided. The defect has been treated before with bone marrow stimulation.
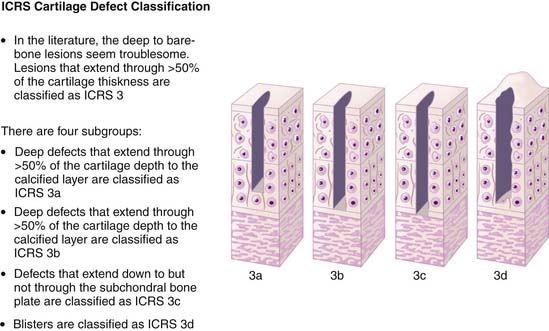
There are four subgroups of this grade:
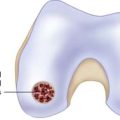
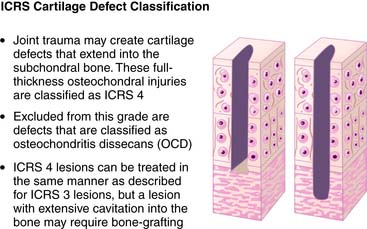
Joint trauma may create cartilage defects that extend into the subchondral bone. These full-thickness osteochondral injuries are classified as ICRS 41,2 (Fig. 3-5). ICRS-4 lesions can be treated in the same manner as described for ICRS-3 lesions, but a lesion with extensive cavitations into the bone may require bone-grafting.
The Debridement Procedure in Defects Grade 3 and 4
After adequate exposure is obtained, the defect must be thoroughly debrided of all unhealthy cartilage surrounding the lesion. This includes all fissures and undermined cartilage, in addition to any fibrocartilage present in the base of the defect (Fig. 3-6).

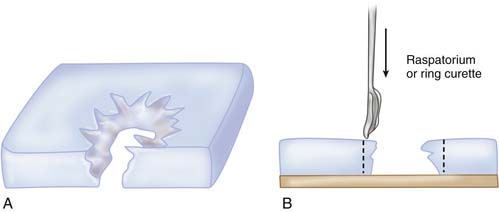
The zone of damaged cartilage surrounding the chondral defect needs to be fully excised, and if you perform open surgery use a fresh scalpel blade, cutting vertically through the cartilage down to the level of, but not into, the subchondral bone (Fig. 3-7). A ring curette or a raspatorium can be used to remove the damaged cartilage or any fibrocartilage in the base of the defect.

When arthroscopic debridement is done, a raspatorium or ring curette is used.
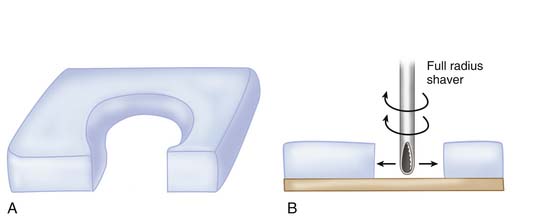
Vertical walls are formed with the raspatorium. A full radius shaver can be used after vertical walls have been formed. The shaver is used from the central part of the defect and conducted with sweeping movements, cleaning the defect toward the periphery (Figs. 3-8, A-B and 3-9, A-B).
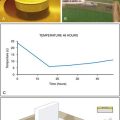
Thermal debridement is also possible.3 Electrocautery, laser, and radiofrequency energy devices can be used. However, earlier it was shown that these devices cause greater chondrocyte death compared to mechanical debridement and shaver use.4 Recent publications show that the new radiofrequency devices now reach similar results regarding cell death as mechanical debridement:5

Pearls and Pitfalls
Radical excision is crucial. All flaps and fissures must be excised. The most common error is not to be radical enough (Fig. 3-11).
1. Brittberg M. Evaluation of cartilage injuries and cartilage repair. Osteologie. 2000;9:17-25.
2. Brittberg M., Winalski C.S. Evaluation of cartilage injuries and repair. J Bone Joint Surg Am. 2003;85-A(Suppl 2):58-69.
3. Lu Y., Markel M.D. Thermal treatment for articular cartilage: basic science and clinical review. In: Zanasi S., Brittberg M., Marcacci M., editors. Basic science. Clinical repair and reconstruction of articular cartilage defects: current status and prospects. Bologna, Italy: Timeo Editore; 2006:135-148.
4. Kääb M.J., Bail H.J., Rotter A., Mainil-Varlet P., Gwynn I., Weiler A. Monopolar radiofrequency treatment of partial-thickness cartilage defects in the sheep knee joint leads to extended cartilage injury. Am J Sports Med. 2005 Oct;33(10):1472-1478. Epub 2005 Jul 11
5. Voloshin I., Morse K.R., Allred C.D., Bissell S.A., Malony M.D., De Haven K.E. Arthroscopic evaluation of radiofrequency chondroplasty of the knee. Am J Sports Med. 2007 Oct;35(10):1702-1707. Epub 2007 Jul 20