Dermoid Cyst
Synonyms/Description
Mature cystic teratoma
Etiology
This is a benign germ cell tumor containing ectoderm, mesoderm, and endoderm, thought to arise from a single germ cell. Components may include hair, teeth, fat, and bone. These tumors represent 25% of all ovarian neoplasms and 60% of all benign ovarian tumors. They are bilateral and or recurrent in 10% of cases. These lesions are benign and typically occur in teenagers and young adults, although approximately 1% may be immature teratomas with malignant components mixed with mature elements.
Ultrasound Findings
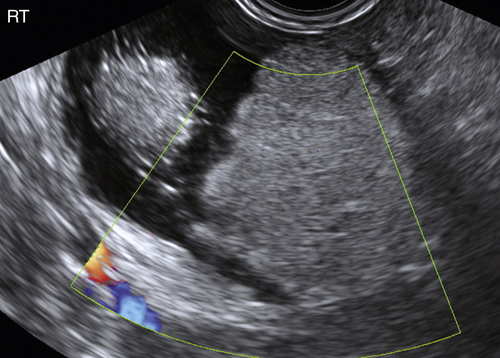
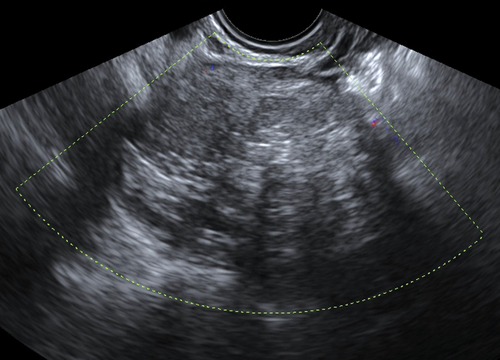
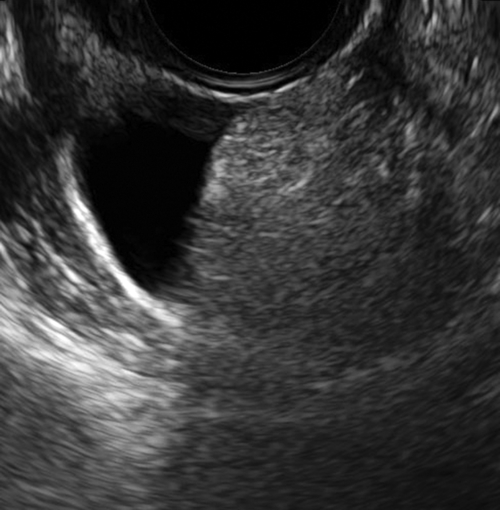
The classic sonographic appearance of a dermoid is an echogenic mass with intense acoustic shadowing obscuring the back wall. A finding coined “tip of the iceberg” refers to this characteristic, which can make obtaining accurate measurements of the mass difficult. The intensely echogenic components of dermoid cysts represent varying combinations of fat, sebaceous material, hair, teeth, and bone. There are often a multitude of thin echogenic lines emanating from the echogenic center representing strands of hair within the mass. The so-called “Rokitansky nodule” is a very echogenic, discrete, rounded protuberance characteristic of a dermoid. There is typically no demonstrable blood flow within these lesions.
Less commonly, dermoids can be predominantly cystic with only a small echogenic nodule that is easy to miss and that indicates the correct diagnosis. There can be septations and low-level echoes, which may be confused as findings consistent with an endometrioma. Occasionally, dermoids can be made up of a multitude of small round balls within a mass, like a cluster of billiard balls. This is rare but when visualized is a characteristic appearance of a dermoid cyst.
Differential Diagnosis
The diagnosis of a dermoid is very specific when the appearance is characteristic. When the appearance is not typical, dermoids can be mistaken for endometriomas, fibromas, and struma ovarii. The absence of color flow on Doppler examination is a very important and helpful feature of dermoids. If a dermoid is suspected but color flow is observed in the solid areas, other etiologies must be considered. The sonographic appearance of the rarer malignant teratoma is similar to the mature lesions except for the Doppler pattern of blood flow. This is rarely seen in the benign lesions but common in malignancies. The short growth interval of the lesion may also suggest a malignancy.
Clinical Aspects and Recommendations
Most dermoid cysts are asymptomatic. If symptoms are present, it often depends on the size of the mass. Such ovarian pathology is not usually associated with adhesion formation, and adnexal torsion can occur, especially if the cyst is large. They rarely rupture, but when they do, spillage of sebaceous material into the abdominal cavity may cause chemical peritonitis and development of dense intra-abdominal adhesions. This rare complication can present with acute symptoms, but the most common cause of acute pelvic pain in the presence of a dermoid is torsion.
Malignant transformation, although extremely rare (quoted to be 0.2% to 2% in such benign teratomas), can occur. This is unlike epithelial ovarian neoplasms, in which benign growths do not transform into malignant ones.
Ovarian cystectomy is the treatment of choice in reproductive-age women when intervention is indicated. This allows for a definitive diagnosis, preservation of ovarian tissue, and decreased risk of torsion or rupture. For those women who have completed their child bearing, salpingo-oophorectomy is an acceptable treatment option. There is a 10% to 20% incidence of bilaterality, and a thorough ultrasound examination of the nonaffected ovary preoperatively should be carried out rather than the historical approach of bivalving that ovary.
Figures


Suggested Reading
Outwater E.K., Siegelman E.S., Hunt J.L. Ovarian teratomas: tumor types and imaging characteristics. Radiographics. 2001;21:475–490.
Sokalska A., Timmerman D., Testa A.C., Van Holsbeke C., Lissoni A.A., Leone F.P., Jurkovic D., Valentin L. Diagnostic accuracy of transvaginal ultrasound examination for assigning a specific diagnosis to adnexal masses. Ultrasound Obstet Gynecol. 2009;34:462–470.
Ushakov F.B., Meirow D., Prus D., Libson E., BenShushan A., Rojansky N. Parasitic ovarian dermoid tumor of the omentum. A review of the literature and report of two new cases. Eur J Obstet Gynecol Reprod Biol. 1998;81:77–82 Review.






